Imaging of Langerhans Cell Histocytosis in an Adult
Langerhans Cell Histocytosis (LCH) is a rare disease of clonal dendritic cells which may affect any organ of the body. The disease is more common in children aged 0-15 years. It is very rare in adults. The current knowledge about the diagnosis and treatment is mostly based on pediatric studies. Here, I report the case of an adult with multiple bony lesions for which she was referred for palliative radiotherapy for metastatic malignancy of unknown primary. It is paramount to have a tissue confirmation for suspected metastatic cancer with non-confirmed primary.
Introduction
The pathogenesis of LCH is unclear although some evidence indicates that it may be more a neoplastic disease than a reactive disorder since LCH cells are clonal (except primary pulmonary LCH) and a cancer-associated mutation (BRAFV600E) was found in more than half of the investigated specimens [1, 2, 3, 4]. The management of adult LCH has been standardized based on the recent recommendation [5].
Case Report
A 60 years old woman presented with a sharp pain in the right shoulder after being thrown to the ground by her boyfriend about 6 months earlier. A referral to orthopedics was put in. Four months before seen by us, X- ray showed a large lytic lesion in the proximal right humerus and head with no underlying fracture (Figure1).

There is a large lytic lesion in the proximal humeral metaphysis on its medial aspect, identified by white arrows.
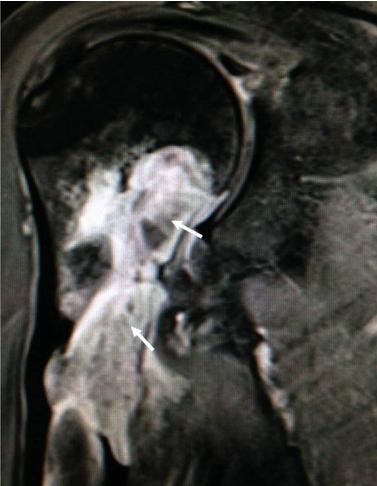
A bone scan showed uptake in the right proximal humerus and the left eighth rib (Figure 2). The orthopedics did not feel that surgical intervention was warranted as the underlying pathology was unknown. A CT scan of the humerus, chest, abdomen and pelvis demonstrated the destructive osseous lesion in the right humeral head and neck measuring 2.3x2.4x6.0 cm (Figure 3). Only the lateral wall of the cortex was intact with extra osseous proliferation around it. There was minimal soft tissue breach medially in relation to this lesion. The CT scan of the chest showed a lytic lesion in the posterolateral right eighth rib with a fracture concerning for malignancy. In the CT scan of the pelvis, bilateral lytic lesions were seen in the iliac bones adjacent to the sacroiliac joints (Figure 4). No soft tissue lesions were noted throughout the body and all solid organs appeared normal. There were no enlarged lymph nodes. MRI of the right arm reported a large aggressive soft tissue mass within the proximal humerus extending from the metaphysis into the proximal humeral shaft with extra- cortical extension (Figure 5). MRI brain and spine showed three enhancing granulomatous lesions of the skull involving the left parietal bone measuring up to 2.8 cm in size. There was no spinal lesion identified. Skeletal survey showed several lucent lesions in the left calvarium, a healing fracture involving in the right proximal right humerus. PET scan showed hyper metabolic activities at the left calvarium with a SUV of 6.7, left maxillary sinus with a SUV of 4.6, right mandible with a SUV of 5.1, right humerus with a SUV of 2.9, right eighth rib with a SUV of 3.8, and bilateral iliac bone with a maximal SUV of 7.4 (Figure 6).

The increased uptake is seen in the proximal right humeral shaft extending to the humeral head. Degenerative changes are seen in the left knee, asymmetric uptake in the skull shows the left side is more intense than the right. Focally increased uptake is seen at the left 8th rib posterolateral identified by the white arrows.

There is a destructive osseous lesion involving the humeral head extending into the surgical neck and proximal diaphysis, measuring 2.3x2.4x6.0 cm (anteroposterior by transverse by craniocaudad), minimal soft tissue component is seen breaching into the cortex medially, identified by the white arrows.
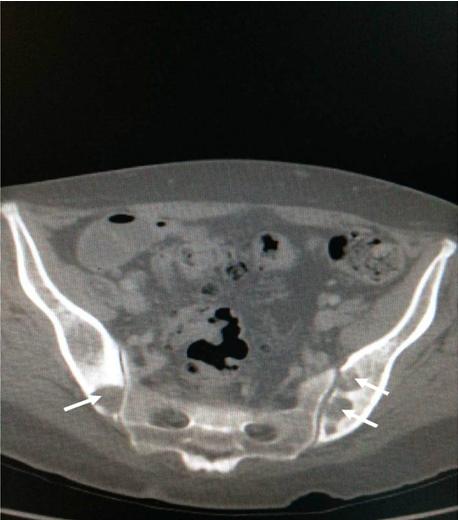
Within the ilium adjacent to the sacroiliac joints bilaterally, there are multiple well defined irregular lytic lesions, identified by the white arrows.
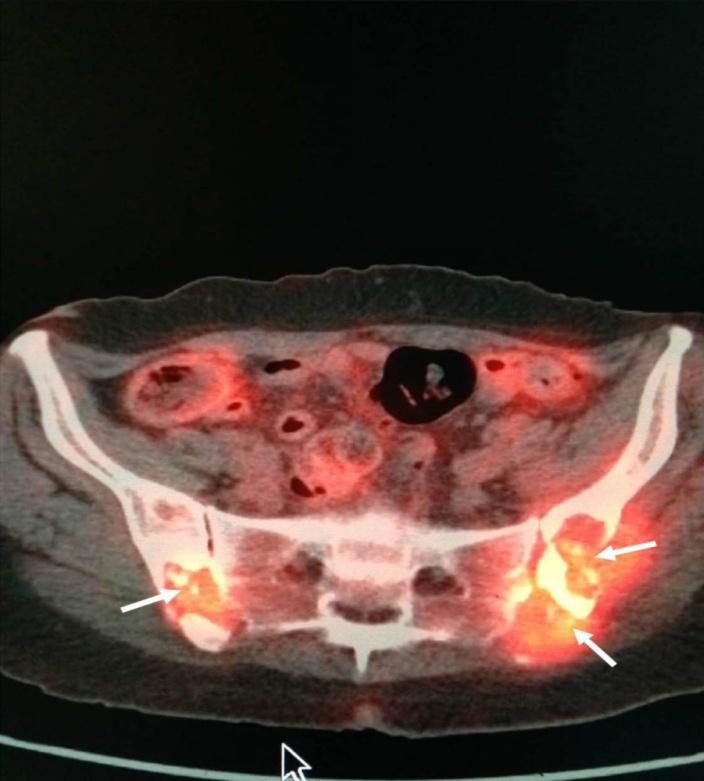
Intense metabolic activity within the iliac bone bilaterally with SUV of 7.4 is seen, identified by the white arrows. In the meantime, she had also had blood work done for work-up including multiple myeloma, which was essentially negative. Notably, her calcium was normal. Clinically, other than the moderate pain from the right upper arm, she had significant weight loss and she attributed this to having to puree all of her food secondary to the problem with the pain in her jaw. Physical examination reveals no adenopathy or organomegaly. She had mildly limited movement of her right arm. There was no overt swelling or erythema in her proximal right arm. She had no sensory or motor deficits in the right arm. Biopsy from the right proximal humerus confirmed Langerhans cell histocytosis. The cells are positive for S100 and CD1a. The patient received a course of radiotherapy, 20 Gy in 10 fractions over 10 days to the right proximal humerus before being referred to hematology for systemic therapy. She was initially treated with Cytarabine for five cycles. Due to disease progression, she was switched to Cladribine and she has completed 7 cycles so far. The recent follow-up PET scan showed interval improvement in the lesions of the skull and the rib but there were two new hypermetabolic osseous lesions in the superior pubic ramus bilaterally.
Discussion
This case showed that it is difficult to make a diagnosis simply based on radiological imaging, without biopsy for tissue confirmation. The images were unspecific. In fact the image findings were very similar to those of metastatic cancer. However the relative slow progression and indolent characteristics of this case does not match with most of metastatic malignancies. It has been over two years now since the initial presentation. The fact she has not achieved a remission although she has received extensive systemic chemotherapy indicates that this disease can be refractory to treatment. Radiotherapy can be an effective treatment option for adult patients with LCH [6, 7, 8]. The local control rates ranges from 75-100% with a complete remission from 79- 100%, respectively [9]. The generally accepted dose ranging from 10 to 20 Gy in 5 to 10 fractions is recommended in adults [10, 11].
References
-
Willman CL, Busque L, Griffith BB, Favara BE, McClain KL, et al. (1994) Langerhans’-cell histocytosis (histocytosisX)-a clonal proliferative disease. N Eng J Med 331(3): 154-160.
-
Yousem SA, Colby TV, Chen YY, Chen WG, Weiss LM (2001) Pulmonary Langerhans’ cell histocytosis: molecular analysis of clonality. Am J Surg Pathol 25(5): 630-636.
-
Badalian-Very G, Vergilio JA, Degar BA, MacConaill LE, Brandner B, et al. (2010) Recurrent BRAF mutations in Langerhans cell histocytosis. Blood 116(11): 1919- 1923.
-
Badalian-Very G, Vergilio JA, Fleming M, Rollins BJ (2013) Pathogenesis of Langerhans Cell Histocytosis. Annu Rev Pathol 24(8): 1-20.
-
Girschikofsky M, Arico M, Castillo D, Chu A, Doberauer C, et al. (2013) Management of adult patients with Langerhans cell histocytosis: recommendations from an expert panel on behalf of Euro-Histio-Net. Orphanet J Rare Dis 8: 72.
-
Atalar B, Robert C Miller, Fazilet Oner Dincbas, Jan Henning Geismar, Oliver Micke, et al. (2010) Adult Langerhans cell histocytosis of bones: a rare cancer network study. Acta Orthop Belg 76 (5): 663-668.
-
Gaundone Mbethe GL, Dejean C, Henriques de Figueiredo B, Sargos P, Italiano A, et al. (2010) Multifocal Langerhans cell histocytosis of bone: indications for radiotherapy. Cancer Radiother 14(8): 759-762.
-
Greenberger JS, Cassady JR, Jaffe N, Vawter G, Crocker AC (1919) Radiation therapy in patients with histocytosis: management of diabetes insipidus and bone lesions. Int J Radiat Oncol Biol Phys 5(10): 1749- 1755.
-
Micke O, Seegenschmiedt MH (2002) Consensus guidelines for radiation therapy of benign diseases a multicenter approaches in Germany. Int J Radiat Oncol Biol Phys 52(2): 496-513.
-
Brady LW (2008) Langerhans Cell Histocytosis. In: Olschewski T, Seegenschmiedt MH, MickeO, (Eds) Springer Verlag, pp 397-423.
-
Cassady JR (1987) Current role of radiation therapy in the management of histiocytosis-X. Hematol Oncol Clin North Am 1(1): 123-129.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage