An Unusual Case of Delayed Periosteum Physeal Interposition: Diagnosis and Surveillance by Imaging and its Role in Clinical Decision Making
One of the most serious complications of fractures involving the physis is future growth disturbance, resulting from transphyseal bar formation and/or premature physeal closure. An uncommon cause of bar formation is uncorrected interposition of soft tissue into the acutely fractured physis. We present the first case of delayed soft tissue interposition, which occurred following displacement across an initially nondisplaced fracture of the proximal tibia that was detected on serial radiographs and confirmed with magnetic resonance imaging (MRI). Although open surgical correction is recommended for acute interposition, our case was successfully managed with a combination of surveillance and guided-growth. This case illustrates the importance of serial surveillance and the use of imaging to guide patient-centered care and achieve optimal outcome.
Introduction
In skeletally immature children, 30% of all fractures involve the physis (growth plate). The most clinically- utilized classification system to describe these fractures is that of Salter and Harris. Originally described in 1963, it subdivides physeal fractures into 5 types based on radiographic appearance and/or mechanism. Regardless of the fracture type, in the acute setting, the goal of treatment is to restore and maintain anatomic alignment utilizing either closed or open reduction techniques and, if indicated, internal and/or external fixation [1]. Physeal injury can produce angulation deformity and limb-length discrepancy through a combination of asymmetric growth, focal transphyseal bar formation, and/or diffuse premature physeal closure, which becomes apparent months to years after the initial injury. The severity of the resultant growth disturbance ranges from those that are radiographically-detectable but clinically- insignificant to those with severe functional impairment requiring multi-staged, open surgical correction. The magnitude of the deformity and the projected remaining growth at the physis determine the necessity and timing for surgical intervention, ranging from less-invasive guided-growth to more invasive osteotomy and/or transphyseal bar resection. The ultimate goal is to correct the deformity, preserve limb-length symmetry, and restore function [1, 2]. Acute interposition of soft tissue into the fractured physis is an uncommon, but surgically-correctable, potential cause of growth disturbance. The most commonly entrapped soft tissue is an avulsed sleeve of metaphyseal periosteum, but less common entities include ligaments and tendons [3, 4]. An irreducible fracture with persistent physeal widening of more than 3mm should raise concern for soft tissue interposition. If
undiagnosed or left untreated, the interposed periosteum has a natural propensity to form bone and can progress to transphyseal bar formation [5]. To date, published cases of soft tissue interposition have occurred and been diagnosed in the acute setting. We present a case of sub acute displacement of periosteum into an initially non- displaced, anatomically aligned Salter-Harris type II fracture of the proximal tibia. This case emphasizes the importance of imaging in the surveillance of even non- displaced physeal fractures as well as its subsequent use to detect early growth disturbance, allowing for prompt surgical intervention.
Clinical Summary
A 10-year-old male was referred to the orthopedic clinic with persistent right knee pain 2 months after an injury while playing football. His initial radiographs showed subtle asymmetric widening of the posteromedial physis of the proximal tibia, but without displacement, which was unfortunately not reported (Figure 1).
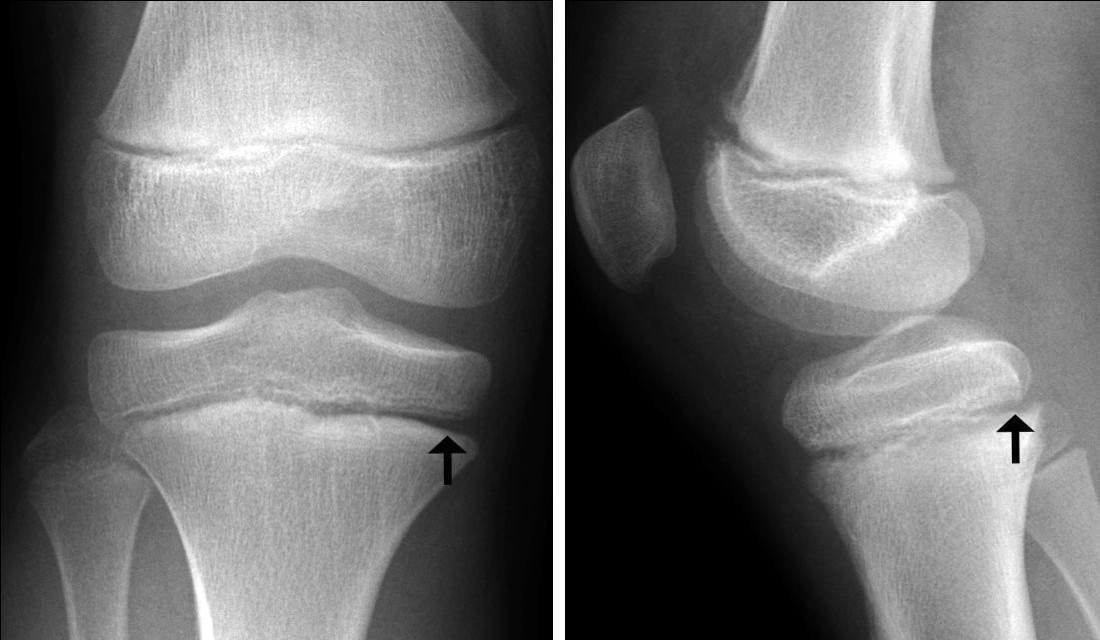
On the day of the referral appointment, follow-up radiograph showed new posterior displacement and asymmetric posterior physeal widening, which, on the subsequent MRI, contained a sleeve of avulsed metaphyseal periosteum (Figure 2).

Figure 2: Fracture displacement with periosteum interposition. Lateral radiograph (a) shows new posterior displacement and physeal widening (arrow). Note the surrounding healing response (wiggly arrows). Subsequent sagittal T2-weighted magnetic resonance (MR) image (b) at the level of the intercondylar notch shows interposition of periosteum (arrowheads). PCL = posterior cruciate ligament.
Given the knee stability on physical examination, he was treated with serial imaging monitoring over the next 2 years, during which time he developed mild progressive genu valgum (5°) and leg-length discrepancy (+3mm).
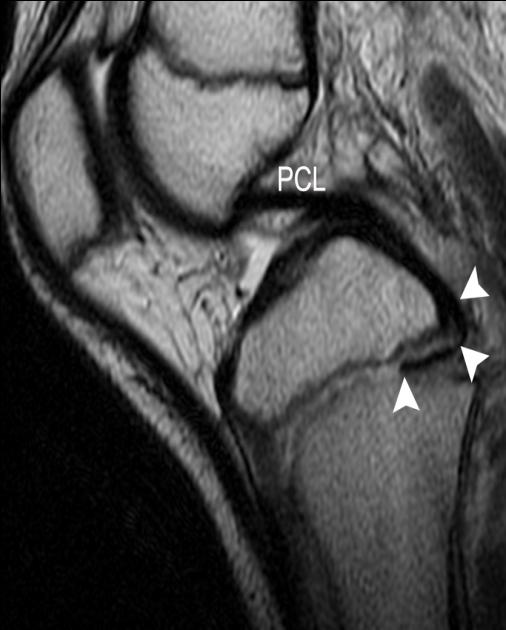
Figure 3: Healed fracture without osseous transphyseal bar. Coronal (a) and sagittal (b) computed tomography (CT) images show physeal irregularity (brackets), but no interval development of an osseous bar. Note the slightly asymmetrically faster growth across the medial proximal tibial physis relative to the lateral physis, which led to the clinically observed valgus deformity.

Pre-operative computed tomography (CT) showed mild physeal irregularity reflecting underlying disorganization, resolved asymmetric physeal widening, and no transphyseal osseous bar (Figure 3a).

Given his young age and projected multiple remaining years of growth, medial proximal tibial hemiepiphysiodesis and fixation using a Peanut® Plate (Zimmer Biomet™, Warsaw IN)were elected to prevent further progression of the growth disturbance (Figure 3b). Over the next 2 years, his valgus alignment resolved and his leg-length discrepancy stabilized.
Discussion
The most common mechanism of injury to the proximal tibia often involves a combination of hyperextension and valgus-directed forces [6]. Although the incidence of proximal tibial physeal fractures is low, accounting for <2% of all physeal fractures, up to 20% of these fractures result in subsequent growth arrest with approximately one third of these patients requiring surgical correction for delayed growth disturbance. Growth disturbances are often less well-tolerated in the lower-extremity because of its weight-bearing function and in younger children because of their longer remaining growth potential [7]. Soft tissue interposition is a correctable cause of malalignment and a potentially correctable cause of future growth disturbance [6]. The current accepted recommendation of prompt open surgical intervention is based on cases that occurred and were diagnosed in the acute setting [3, 4]. With our patient, periosteal tearing could have occurred either at the time of the initial injury or during the subsequent displacement. Unfortunately, when this patient presented to us for his referral, knee stability has already been re-established, reflecting underlying interval healing and making this patient a poor surgical candidate. This unique delayed presentation has not been previously described in the published literature and reinforces the need for short-term (1-2 weeks) radiographic and clinical surveillance of patients with suspected physeal or periphyseal injury with persistent pain. A variety of imaging modalities were used to evaluate our patient starting with radiographs. However, acute non-displaced physeal fractures can be subtle or even occult on initial radiographs. Radiographic findings can include cortical discontinuity, soft tissue swelling, subtle physeal widening, and/or joint effusion [8]. Although comparison with the contralateral symptomatic side can be helpful, it is not uncommon that a confident diagnosis is only rendered retrospectively, following the development of a healing response (periosteal reaction, peri-fractural reabsorption, and later sclerosis). While physeal widening on radiographs is non-specific, persistent widening of more than 3mm should raise the suspicion for soft tissue interposition. Barmada et al. showed an increased incidence of premature physeal closure in cases with physeal widening (60%) as opposed to cases without widening (17%) [5]. When radiographs remain normal and the patient continues to have post-traumatic pain, MRI remains the preferred problem-solving imaging modality to detect occult fractures, bone contusions, soft tissue injury, and/or internal joint derangements [8]. On MRI, acute physeal fracture can produce increased intra-physeal signal on fluid-sensitive sequences and a cleft of non- enhancement on post-contrast T1-weight fat-saturated sequences as well as the loss of the normal bright physeal signal on gradient-recalled echo (GRE) sequences [9]. If present, an entrapped periosteum appears as a well- defined band of low signal on all pulse sequences. Despite its superior anatomic resolution, routine use of MRI to screen cases of suspected physeal injury or to evaluate known cases of physeal injury (without concern for soft tissue interposition) is neither practical (with the possible need for sedation and often limited immediate availability) nor shown to consistently and substantially alter patient management and outcome [10]. CT has traditionally been reserved for pre-surgical planning, to identify and quantify the extent of transphyseal osseous bar, which appears as focal loss of the normal physeal lucency and can have adjacent reactive sclerosis from altered biomechanics [8]. However, CT can miss fibrous bridges and uses radiation. This has led to the increasing use of MRI with 3- dimensional (3D) GRE sequences which allow multiplanar reformations [11]. Interestingly, our patient did not develop a transphyseal bar, but rather developed asymmetrical growth leading to mild valgus alignment, which was subsequently corrected with medial hemiepiphysiodesis. To conclude, growth disturbance is a possible complication of physeal fractures and soft tissue interposition should be considered when the fracture resists complete reduction and there is persistent physeal widening. Delayed presentation of soft tissue interposition can be successfully managed with a combination of imaging surveillance and guided-growth. Our case illustrates the use of advanced imaging to help customize patient-centered treatment and to ensure the most optimal outcome.
References
-
Arkader A, Skaggs DL (2015) Physeal Injuries. In: Mencia GA, Swiotkowski MF (Eds) Green's Skeletal Trauma in Children. 5th edn. Elsevier, Philadelphia, PA, pp: 16-35.
-
Escott BG, Kelley SP (2012) Management of traumatic physeal growth arrest. Orthopaedics and Trauma 26 (3): 200-211.
-
McAnally JL, Eberhardt SC, Mlady GW, Fitzpatrick J, Bosch P (2008) Medial collateral ligament tear entrapped within a proximal tibial physeal separation: imaging findings and operative reduction. Skeletal Radiol 37(10): 943-946.
-
Wood KB, Bradley JP, Ward WT (1991) Pes anserinus interposition in a proximal tibial physeal fracture. A case report. Clin Orthop Relat Res 264: 239-242.
-
Barmada A, Gaynor T, Mubarak SJ (2003) Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor. J Pediatr Orthop 23(6): 733-739.
-
Mayer S, Albright JC, Stoneback JW (2015) Pediatric Knee Dislocations and Physeal Fractures About the Knee. J Am Acad Orthop Surg 23(9): 571-580.
-
Ecklund K, Jaramillo D (2001) Imaging of growth disturbance in children. Radiol Clin North Am 39(4): 823-841.
-
Miller E, Davila J, Rotaru C, Koujok K (2012) Pediatric Skeletal Trauma. In: Imaging Musculoskeletal Trauma. John Wiley & Sons, Ltd, p: 31-59.
-
Jaramillo D, Kammen BF, Shapiro F (2000) Cartilaginous path of physeal fracture-separations: evaluation with MR imaging--an experimental study with histologic correlation in rabbits. Radiology 215(2): 504-511.
-
Petit P, Panuel M, Faure F, Jouve JL, Bourliere-Najean B, et al. (1996) Acute fracture of the distal tibial physis: role of gradient-echo MR imaging versus plain film examination. AJR Am J Roentgenol 166(5): 1203- 1206.
-
Lurie B, Koff MF, Shah P, Feldmann EJ, Amacker N, et al. (2014) Three-dimensional magnetic resonance imaging of physeal injury: reliability and clinical utility. J Pediatr Orthop 34(3): 239-245.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage