Biometric Evaluation of Intracapsular Structures of the Temporomandibular Joint Before and After Orthesis Installation
Objective: The objective of this study was to evaluate the biometric modifications to intracapsular structures that occur after installation of orthoses of modified “Planas” type, in patients with TMD, by means of MRI of the TMJ. Methods and Material: Twelve patients with diagnoses of TMD were selected and clinically examined. They underwent TMJ examination using MRI before and after installation of the modified “Planas” orthoses. The examinations were performed using Siemens Concerto equipment with a magnetic field of 0.2 T and gradient of 20 mT and the image acquisition in the sagittal plane with a Flash-3D sequence, weighted in T1, with and without the orthosis, with the open and closed mouth. The following measurement reference points were established: upper condyle, upper glenoid and lower glenoid. From these points, the distances between the upper glenoid and upper condyle and between the lower glenoid and upper condyle for closed and open mouth were measured on both joints. Results: The mean value for the closed mouth without appliance was 0.34 cm, and with the orthosis installed, it was 0.56 cm (increase of 0.22 cm). The value for open mouth without appliance was 1.15 cm and this was also the value for open mouth with appliance. Conclusion: We concluded that installation of the modified “Planas” orthosis significantly increased the upper glenoid and upper condyle spaces and that the increase in these spaces presented a significant correlation with clinical improvement of the patients.
Introduction
Temporomandibular disorders (TMD) are manifested by signs and symptoms that are attributed to occlusal, psychological and neuromuscular imbalances, in combination or separately. These consequently lead to changes in the oral motor sensory system and, more intensively, in stomatognathic functions: mastication, deglutition and even breathing [1]. Even though studied long ago, there are still many controversies in relation to etiology, diagnosis and treatment [1]. Among the most characteristic clinical signs of TMD is muscle and joint sensitivity to palpation and limitations on and/or difficulty in mandibular movement [2]. Diagnosis by means of imaging of the temporomandibular joint (TMJ) and other craniofacial structures is frequently an important phase in collecting data from patients with TMD. The technological advances in this area have established less invasive methods for showing the muscle abnormalities that result from TMD, although there are few studies in this field [3]. Magnetic resonance imaging (MRI) is the best method for noninvasive TMJ investigation. It clearly shows how the upper portion of the lateral pterygoid muscle is attached to the joint capsule and the anterior portion of the disc, and how the lower portion of this muscle is attached to the mandibular condyle [4]. Occlusal plates are widely used for treating TMD, in order to modify the occlusal relationship, redistribute the forces, avoid tooth wear, change the structural relationships between forces and TMJ, improve muscle and joint function and relieve associated pain. If TMD is diagnosed due to loss of vertical occlusal dimension (VOD), intraoral orthosis is indicated as a form of treatment, to increase or recover this measurement, thereby providing symptom improvement and proprioceptive pathological muscle memory for the patient [5, 6]. The aims of this study were to investigate, by means of MRI, whether installation of an intraoral orthosis of modified “Planas” type would increase the distance between the cortical points of the condyle head and the glenoid fossa, and to evaluate whether such increases would decrease the painful symptoms after 30 days [7].
Material and Methods
For this study developed in the Department of Imaging Diagnostics of UNIFESP, twelve patients of both genders and aged between 18 and 70 years were selected. They presented Angle class I, with a diagnosis of TMJ pain syndrome and complaints of localized pain for more than five years. This study was approved by the Research Ethics Committee of UNIFESP, and all patients were clearly informed about the aims and methodology of the study. They gave their consent for participating in the study, in accordance with a free and informed consent statement.
The patients underwent a clinical examination protocol, in which palpation was performed by means of pressure from the index finger for three to four seconds on the following muscles: posterior, medial and anterior portions of the temporal muscle on the right and left sides; superficial and deep portions of the masseter muscle on the right and left sides; upper, medial and lower portions of the sternocleidomastoid muscle on the right and left sides; and cervical and cervicoacromial portions of the trapezoid muscle on the right and left sides. The TMJ was also palpated with the mouth closed, functioning and open, on the right and left sides. Standard responses of “yes” and “no” were used to determine whether pain was present. The lab confection of the modified “Planas” appliance was made up in the laboratory, using chemically activated acrylic resin, with smooth neutral tracks over the upper and lower occlusals. The appliance raised the bite when installed and changed the vertical dimension of the occlusion. The patients were instructed to use the orthosis for 12 hours/day for 30 days, with reexamination after this period.
Acquisition of Images from Magnetic Resonance Imaging
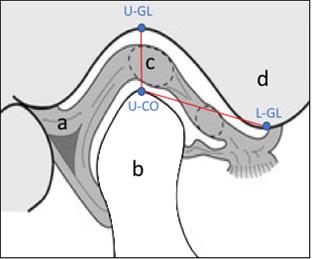
The selected patients underwent bilateral MRI examination of the TMJ. Images were acquired in the sagittal plane, weighted in T1, with cutoffs of 3mm,using the Concerto equipment (Siemens Company, Erlanger, Germany), with 0.2 T and a gradient of 20 mT. The examinations were performed using gradient-echo sequences weighted in T1, in the sagittal plane at the level of the TMJ, with the Flash-3D sequence, with the mouth open and closed, before and after placement of the modified “Planas” appliance. The intra-joint TMJ spaces were evaluated bilaterally, and the craniometric condyle point was marked out (highest posterior point of the head of the mandibular condyle in each joint). On the highest anterior face of the condyle, another point was marked: the anterior condyle. These two points, i.e. the condyle and anterior condyle, which marked the most posterior and anterior points of the condyle, were joined with a straight line. A line perpendicular to this determined the upper condyle point (U-CO), i.e. the highest point of the condyle head or the most distant point from this line Figure 1. In the mandibular fossa or glenoid cavity, the highest point in relation to the condyle head or the apex of the ellipse within the mandibular fossa of the temporal bone was marked. We named this the upper glenoid (U-GL). At the lowest anterior point of the anterior joint eminence or transverse root of the zygoma, we marked a point that we named the lower glenoid (L-GL) Figure 1.
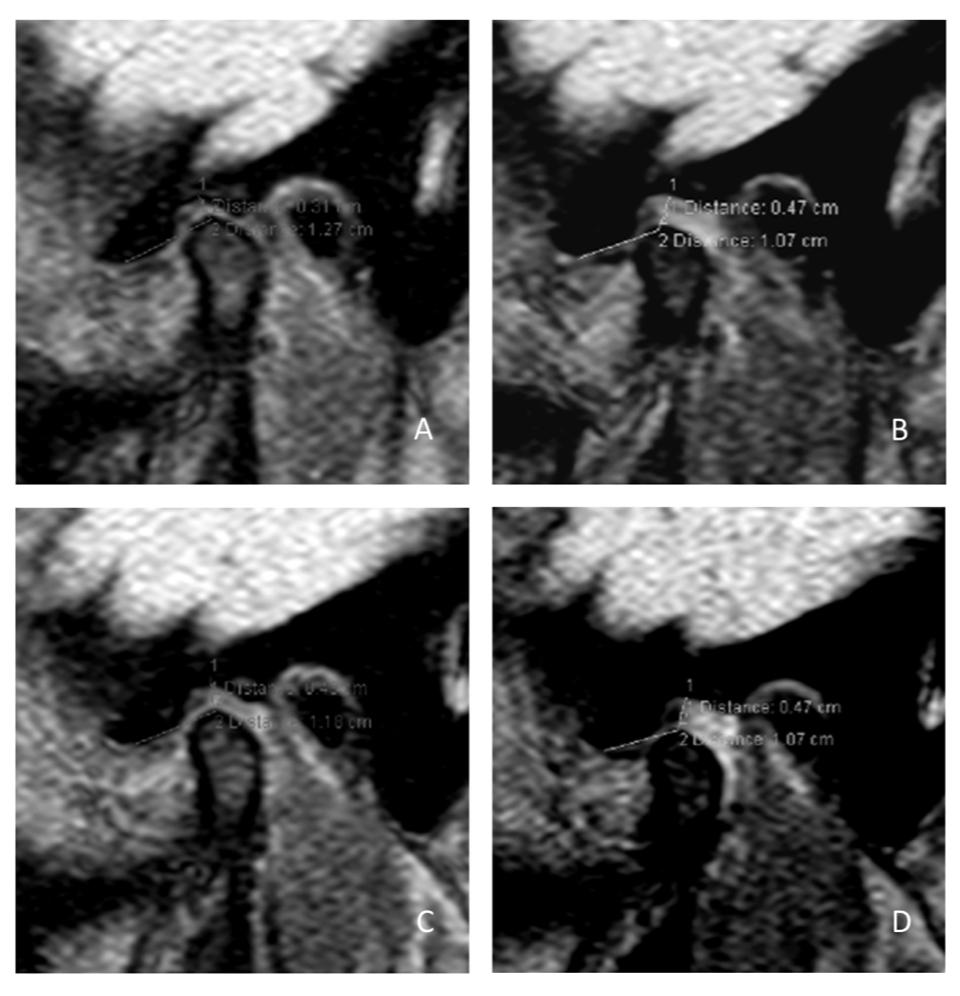
After establishing these points, the following measurements were made between them: 1. TMJ, with closed mouth without appliance (CMWOA, Figures 2 – A and C) and closed mouth with appliance (CMWA, Figures 2B and D): measurements of the points in cm and then CMWA – CMWOA = difference between U-GL and U-CO with and without appliance, i.e. the distance from the mandibular fossa to the mandibular condyle head with the mouth closed; 2. Right and left TMJ, with open mouth without appliance (OMWOA) and open mouth with appliance (OMWA):
measurements of the U-GL and U-CO in cm and then
$$ O M W A - O M W O A = d i f f e r e n c e b e t w e e n t h e $$
measurements with and without appliance, in the open
mouth with appliance;
3. Right and left TMJ, with closed mouth with and without appliance: measurements of the points in cm and then CMWA – CMWOA = difference between the L-GL and U- CO, in the closed mouth with appliance; 4. Right and left TMJ, with open mouth with and without appliance: measurements of the L-GL and U-CO in cm and then OMWA – OMWOA = difference between the measurements with and without appliance, in the open mouth with appliance.
After establishing the craniometric point values for each TMJ, we classified the disc positions as A (normal position) or B (anterior position in the closed mouth without appliance or in occlusion for the right and left TMJ). For statistical analysis, the chi-square test was used to compare the differences between U-GL/U-CO and L-GL/U- CO, with and without appliance, with open and closed mouth, on the right and left sides. The rejection level for the null hypothesis was set at 5%.
The results found are shown in Tables 1-5. The mean value for the closed mouth without appliance was 0.34 cm, and with the orthosis installed, it was 0.56 cm, or an increase of 0.22 cm, as shown in Table 2. The mean value for open mouth without appliance was 1.15 cm and this was also the value for open mouth with appliance, even though there were changes in a few single measurements, as can be seen in Table 3.
Results
| Pain Side | TMJ | TMJ after 30 days | ||
| Pain Side | CM | OM | CM | OM |
| Right | (9) 75% | (11) 91.6% | (1) 8.3% | (6) 50% |
| Left | (10) 83.3% | (11) 91.6% | (3) 25% | (4) 33% |
| Both | (8) 66% | (11) 91.6% | (0) 0% | (2) 16.6% |
| Without Pain | (0) 0% | (1) 8.3% | (8) 66% | (4) 33% |
Table 1: Percentages and numbers of patients with painful symptoms in the TMJ, in open and closed mouth situations, Table 1: Perc
| Samples Compared | Differences between Means | p | ||
| SCMWOA-R | X | SCMWA-R | 16.5 | 1% |
| SCMWOA-R | X | SCMWOA-L | 1.75 | ns |
| SCMWOA-R | X | SCMWA-L | 14.25 | 1% |
| SCMWOA-R | X | SCMWOA-L | 14.75 | 1% |
| SCMWA-R | X | SCMWA-L | 2.25 | ns |
| SCMWOA-L | X | SCMWA-L | 12.5 | 5% |
Table 2: Comparison between means from samples in the closed mouth position with and without appliance Table 2: Comparison betwee
Table 2: Comparison between means from samples in the closed mouth position with and without appliance Table 2: Comparison between means from samples in the closed mouth position with and without appliance SCMWOA – Closed mouth without appliance in relation to the “S” point; SCMWA - Closed mouth with appliance in relation to the “S” point; R- right; L- left; ns – not significant
| Samples Compared | Differences between Means | p | ||
| SOMWOA-R | X | SOMWA-R | 1.625 | ns |
| SOMWOA-R | X | SOMWOA-L | 1.1667 | ns |
| SOMWOA-R | X | SOMWA-L | 2.2917 | ns |
| SOMWA-R | X | SOMWOA-L | 2.7917 | ns |
| SOMWA-R | X | SOMWA-L | 3.9167 | ns |
| SOMWOA-L | X | SOMWA-L | 1.125 | ns |
Table 3: Comparison between means from samples in the open mouth position with and without intraoral appliance.
| Samples Compared | Differences between Means | p | ||
| ICMWOA-R | X | ICMWA-R | 12.9583 | 5% |
| ICMWOA-R | X | ICMWOA-L | 5.375 | ns |
| ICMWOA-R | X | ICMWA-L | 18.3333 | 0.10% |
| ICMWA-R | X | ICMWOA-L | 7.5833 | ns |
| ICMWA-R | X | ICMWA-L | 5.375 | ns |
| ICMWOA-L | X | ICMWA-L | 12.9583 | 5% |
Table 4: Comparison between means from samples in the closed mouth position with and without appliance in relation to Table 4: Co
Table 4: Comparison between means from samples in the closed mouth position with and without appliance in relation to Table 4: Comparison between means from samples in the closed mouth position with and without appliance in relation to the “I” point: ICMWOA - Closed mouth without appliance in relation to the “I” point; ICMWA - Closed mouth with appliance in relation to the “I” point; R- right; L- left; ns – not significant
| Samples Compared | Differences between Means | p | ||
| IOMWOA-R | X | IOMWA-R | 0.125 | ns |
| IOMWOA-R | X | IOMWOA-L | 1.2917 | ns |
| IOMWOA-R | X | IOMWA-L | 1.8333 | ns |
| IOMWA-R | X | IOMWOA-L | 1.4167 | ns |
| IOMWA-R | X | IOMWA-L | 1.9583 | ns |
| IOMWOA-L | X | IOMWA-L | 0.5417 | ns |
Table 5: Comparison between means from samples in the open mouth position in relation to the “I” point.
Table 5: Comparison between means from samples in the open mouth position in relation to the “I” point. IOMWOA – Table 5: Comparison between means from samples in the open mouth position in relation to the “I” point. IOMWOA – Open mouth without appliance in relation to the “I” point; IOMWA – Open mouth with appliance in relation to the “I” point; R- right; L- left; ns – not significant
Discussion
Many studies have sought to identify morphological changes in the TMJ through analyzing magnetic resonance imaging from patients with TMD. These studies have defined whether the disease was present or not, quantified the pathological tissue involved, quantified the magnitude of the degenerative process, and determined whether it was reversible or not, i.e. whether the process could be stabilized. Some studies have emphasized the importance of magnetic resonance imaging, with special attention to intra-joint pathological conditions of the TMJ, disc apposition, excursion, morphologic abnormalities, etc, thereby enabling diagnoses of internal TMJ disorders that are more specific [4, 5, 6, 7, 8, 9, 10]. The present study aimed to objectively show the clinical efficiency of an orthosis that the authors modified from the classic “Planas” model of functional orthopedic appliance [7]. This consisted of constructing two contact orthoses that were smooth on the occlusal faces and fitted onto the teeth, thus increasing the VOD and simulating a scenario of vertical increase. All of the dental fit or engagement represented by maximal centric intercuspation (MCI) was lost. This release of movement allowed the TMJ and related muscles to function and return to better spatial positioning without interference and without intracapsular compressive forces while at rest, in situations with the mouth closed, therefore justifying its nighttime use for 12 hours. In addition to presenting a significant clinical condition, the patients that showed chronic pain have led us to study the correlation between clinical diagnostic hypotheses and correlations by means of MRI examinations. This has become a field for many studies, which have affirmed that there is a connection between pain and MRI signs [11, 12]. In other words, the existence of morphological abnormalities is closely related to clinical pain. At the same time, disc positions and the morphological state, function, dislodgement and inflammation of such discs have been studied. Our study had precisely the aim of measuring the values of a new predictive intracapsular cephalometric tracing that would allow radiologists to evaluate whether installed orthoses confer intracapsular measurements that bring therapeutic efficacy. The clinical results showed that installing the “Planas” modified orthosis improved the muscle algic pattern, thereby confirming the results in the literature [7, 13, 14]. In analyzing our results in relation to localized pain in the TMJ, we found obtained pain in 75% and 83.3% of the right and left sides, respectively, with the mouth closed. After thirty days, our results showed pain in only 8.3% and 25%, which was a large decrease. Regarding the open mouth position, we found pain in 91.6% for both sides and, after thirty days, this decreased to 50% and 33%. Therefore, the present study concurs with previous affirmations with regard to investigating the tissue response to degenerative abnormalities in the TMJ [5, 13, 14, 15]. It also affirmed that, just like the joint disc, the joint cartilage that covers the condyle (joint eminence) could be affected by degenerative processes such as osteoarthrosis. These processes harm shape and function, thereby causing compensatory or pathological responses regarding the disc and adjacent tissues. The distance between the cortex of the condyle head and the mandibular fossa is a relevant factor in procedures relating to temporomandibular disorders, as also confirmed by other studies [16, 17, 18, 19]. In our study, we observed that an increase in the distance of the craniometric points led to a clinical improvement for the patients. The mean distance between U-GL and U-CO in closed mouth situations without appliance was 0.34 cm, and for this same measurement, we found a value of 0.56 cm with the appliance installed. In other words, the orthosis installation increased the distance between the mandibular fossa and the condyle head by an average of 0.22 cm. Associated with this result, there was an improvement in symptoms in all the cases studied. Moreover, this should also provide functional or compressive rest for intracapsular TMJ structures. This increase can also be measured during the first MRI examination for installing the orthosis. The TMJ can be measured with and without the orthosis installed, thereby confirming the views of authors who advocate the use of intraoral orthoses, which could be single or double, anterior, posterior or covering the whole occlusion. These authors affirm that the increase invertical occlusal dimension caused by these orthoses promotes intra-joint decompression in the TMJ, thus increasing or promoting better translation conditions for the condylar meniscus [6, 7, 13, 15, 19]. In the light of the methods used, our results showed that incremental installation of standardized orthoses and the acquisition of images from the first MRI examination brings new data for the radiological evaluation of TMJ, thus allowing radiologists and clinicians to analyze the intra-joint space situation. This turns MRI before and after the orthosis installation into a predictive examination with regard to the possibility of clinical improvement.
Conclusions
The installation of intraoral modified “Planas” orthoses increased the distance between the craniometrical points of the cortex of the condyle head and mandibular fossa. With this increased distance, we observed a clinical improvement in all cases, after thirty days.
References
-
Kraus H (1973) Métodos físicos. In: Schwartz LL, Chaves CM (Eds.), Dolor facial y disfunción mandibular. Buenos Aires: Mundi pp: 300-308.
-
Donlon WC, Moon KI (1987) Comparison of magnetic resonance imaging, arthrotomography and clinical and surgical findings in temporomandibular joint internal derangements. Oral Surg Oral Med Oral Pathol 64(1): 2-5.
-
Nassri LFG (2005) Análise comparativa entre os achados de ressonância magnética e de eletromiografia do músculo facial masseter, em indivíduos com e sem disfunção temperomandibular. São Paulo, Universidade Federal de São Paulo, pp: 66.
-
Katzberg RW, Schenck J, Roberts D, Tallents RH, Manzione JV, et al. (1985) Magnetic resonance imaging of the temporomandibular joint meniscus. Oral Surg Oral Med Oral Path 59(4): 332-335.
-
Widmalm SE (1999) Use and abuse of bite splints. Comp Continuing Educ Dent 20(3): 249-259.
-
Kurita H, Ikeda K, Kurashina K (2000) Evaluation of the effect of a stabilization splint on occlusal force in patients with masticatory muscle disorders. J Oral Rehab 27(1): 79-82.
-
Planas P (1992) Equilibrium and neuro-occlusal rehabilitation. Orthod Fr 63(Pt 2): 435-441.
-
Yatani H, Sonoyama W, Kuboki T, Matsuka Y, Orsini MG, et al. (1998) The validity of clinical examination for diagnosing anterior disk displacement without reduction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85(6): 647-653.
-
Helms CA, Gillespy T, Sims RE, Richardson ML (1986) Magnetic resonance imaging of internal derangement of the temporomandibular joint. Radiol Clin North Am 24(2): 189-192.
-
Taskaya-Yilmaz N, Ogütcen-Toller M (2001) Magnetic resonance imaging evaluation of temporomandibular joint disc deformities in relation to type of disc displacement. J Oral Maxillofac Surg Aug 59(8): 860- 866.
-
Bertram S, Rudisch A, Innerhofer K, Pümpel E, Grubwieser G, et al. (2001) Diagnosing TMJ internal derangement and osteoarthritis with magnetic resonance imaging. J Am Dent Assoc 132(6): 753-761.
-
Cholitgul W, Nishiyama H, Sasai T, Uchiyama Y, Fuchihata H, et al. (1997) Clinical and magnetic resonance imaging findings in temporomandibular joint disc displacement. Dentomaxillofac Radiol 26(3): 183-188.
-
Stegenga B, de Bont LG, Boering G, van Willigen JD (1991) Tissue responses to degenerative changes in the temporomandibular joint: a review. J Oral Maxillofac Surg 49(10): 1079-1088.
-
McNamara JA, Okeson JP, Seligman DA (1995) Occlusion, orthodontic treatment and temporomandibular disorders. J Orofacial Pain 9(1): 73-90.
-
Seedorf H, Weinterdorf H, Scholz A, Kirsch I (2009) Effected of non-working occlusal contacts on vertical condyle position. J Oral Rehabil 36(6): 435-441.
-
Cirbus MT, Smilack MS, Beltran J, Simon DC (1987) Magnetic resonance imaging in confirming internal derangement of the temporomandibualr joint. J Prosth Dent 57(4): 488-494.
-
Emshoff R, Innerhofer K, Rudisch A, Bertram S (2001) Relationship between temporomandibular joint pain and magnetic resonance imaging findings of internal derangement. Int J Oral Maxillofac Surg 30(2): 118- 122.
-
Paesani D, Westesson PL, Hatala M, Tallents RH, Kurita K (1992) Prevalence of temporomandibular joint internal derangement in patients with craniomandibular disorders. Am J Orthod Dentofacial Orthop 101(1): 41-47.
-
Marguelles-Bonnet RE, Carpentier P, Yung JP, Defrennes D, Pharaboz C (1995) Clinical diagnosis compared with findings of magnetic resonance imaging in 242 patients with internal derangement of the TMJ. J Orofacial Pain 9(3): 244-253.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage