Bleeding During CT Guided Percutaneous Transgastric Drainage of Pancreatic Necrotic Collection
Endoscopic internal drainage of pancreatic necrosis is considered as a first line therapeutic approach to tackle this pathology. Percutaneous drainage remains the second option if the above procedure fails or expertise is not available. Many centers are however still averse to doing the percutaneous drainage due to high risk of various complications and technical intricacies such as pancreatico-cutaneous fistula, risk of intraperitoneal leakage around the tube and lack of safe access route in all cases. CT guided transgastric drainage of pancreatic collection conflates the advantage of both internal and percutaneous drainage, and is offered as a primary management approach at our Institute. The transgastric approach minimizes risk of formation of pancreaticocutaneous fistula, as the contents of the collection leak into gastric lumen. Previous studies have shown that the tube removal following the transgastric drainage can be done after 6 weeks during which a mature track is formed between the collection and stomach. Thick gastric wall prevents the leakage of gastric content into the peritoneum and the gastrocutaneuous fistula eventually heals. We discuss a specific emergency clinical situation and our modus operandi thereby during one such procedure. The informed consent has been taken from the patient and manuscript has been approved by Institutional Review Board (IRB).
Letter to Editor
Endoscopic internal drainage of pancreatic necrosis is considered as a first line therapeutic approach to tackle this pathology. Percutaneous drainage remains the second option if the above procedure fails or expertise is not available. Many centers are however still averse to doing the percutaneous drainage due to high risk of various complications and technical intricacies such as pancreatico-cutaneous fistula, risk of intraperitoneal leakage around the tube and lack of safe access route in all cases [1, 2, 3, 4]. CT guided transgastric drainage of pancreatic collection conflates the advantage of both internal and percutaneous drainage [1], and is offered as a primary management approach at our Institute. The transgastric approach minimizes risk of formation of pancreaticocutaneous fistula, as the contents of the collection leak into gastric lumen [1, 2, 3, 4]. Previous studies have shown that the tube removal following the transgastric drainage can be done after 6 weeks during which a mature track is formed between the collection and stomach [2]. Thick gastric wall prevents the leakage of gastric content into the peritoneum and the gastrocutaneuous fistula eventually heals [3]. We discuss a specific emergency clinical situation and our modus operandi thereby during one such procedure. The informed consent has been taken from the patient and manuscript has been approved by Institutional Review Board (IRB).
A 35-year old female was hospitalized with acute necrotizing pancreatitis, on the seventh day of her illness. The patient was septicemic on admission with total WBC counts of 18000/ mm3. Biphasic CT of abdomen revealed an ill-defined necrotic collection anterior to pancreatic Letter to Editor $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} + \frac {1}{2} \mathrm {C} ^ {2} + \frac {1}{2} \mathrm {D} ^ {2} $$ body and tail extending to the lesser sac and along left anterior pararenal fascia. Anteriorly, the collection was abutting posterior gastric wall. Visceral arteries were normally visualised on arterial phase CT. On Portal venous phase, the splenic vein was compressed by the collection and few irregular venous channels were observed near the head of pancreas. Inability to adequately visualise the collection through the sonography and unavailability of endoscopic drainage facility in the Emergency setting persuaded us to opt for CT guided transgastric catheter drainage of necrotic collection. Patient’s coagulation profile was normal. The procedure was performed as per the standard technique with all precautions and a 12 F Malecot catheter was inserted into the collection. A check scan confirmed the position of catheter and guidewire in situ (Figure 1A). However, immediately after the guidewire removal, expulsive hemorrhagic output was noted from the catheter followed by exodus of fresh blood. Considering the possibility of vascular injury, CT angiography was immediately performed using bolus tracking technique after injecting 80 mL of intravenous non-ionic contrast. The arterial phase did not show any evidence of active contrast extravasation, however the portal venous phase showed contrast pooling (Figure 1B) within the lesser sac collection originating from the region of the pancreatic head (precisely where the tuft of abnormal vessels was seen on diagnostic scan). As the bleeder was well outside the field of our current procedure, the venous bleed might have occurred due to sudden rupture of one of the peri- pancreatic collaterals as a consequence of precipitous fall in the compartment pressure following percutaneous access. There are previous reports of vessel rupture during aggressive surgical necrosectomy and percutaneous drainage [5]. Notably, vascular walls that lie in close vicinity to pancreatic juice/necrotized material become friable and can rupture easily (even due to sudden transmural pressure changes). Drainage catheter was sutured to the skin and the patient managed conservatively with regular monitoring of output, counts and general condition. Whole blood transfusion was given twice to counter the low hematocrit. The parameters improved progressively and the sanguineous component in output ceased totally by the third day. Patient condition improved and the Total Leucocyte count reduced to 9000/ mm3on day 10 of the procedure. On 6 weeks follow-up, there was minimal output from the catheter, which was then removed.
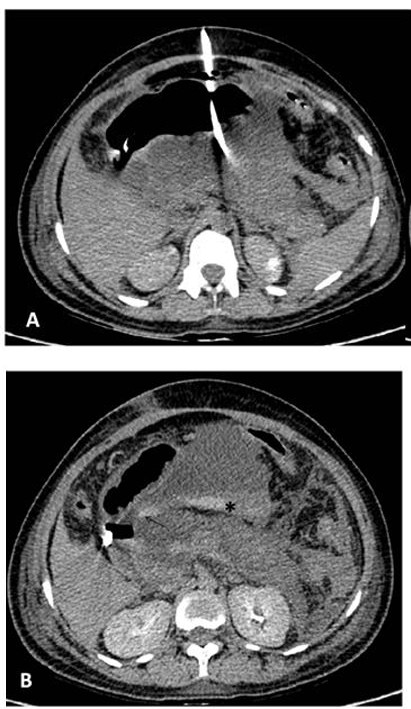
Figure 1A: Non contrast Axial CT of abdomen shows transgastric catheter placed in the lesser sac collection. Note the absence of hyperdense hemorrhagic content within the collection at this stage.
Figure 1B: Biphasic CT was performed after the catheter yielded expulsive hemorrhagic output. Portal venous phase showed contrast pooling (asterisks) within the lesser sac collection originating from the region of pancreatic head (arrow). Note the hyperattenuating nasogastric tube within the gastric lumen.
The present case highlights another advantage of using CT guidance in this procedure as not uncommonly radiologists are tempted to perform pancreatic drainage under sonographic guidance. In case of any inadvertent significant bleed during the procedure, a prompt CT angiography can be performed to rule out an arterial injury while the patient is still on the table. Furthermore, in case abnormal vessels are seen in the field of procedure one should be cautious enough with provision/patient counselling for transfusion and prolonged hospitalization.
Finally we would also like to make our endoscopist brethren aware of the complication as similar pressure dynamics and hemorrhage can occur during endoscopic procedure but may remain occult. Hence during endoscopic procedures in such situations close monitoring of hematocrit and blood pressure should be done so as not to miss this rare but potentially fatal complication.
References
-
Nunez D, Ynzarry JM, Russell E, Sadighi A, Casillas J, et al. (1985) Transgastric drainage of pancreatic fluid collections. AJR Am J Roentgenol 145(4):815-818.
-
Kerlan RK, Jeffrey RB, Pogany AC, Ring EJ (1985) Abdominal abscess with low-output fistula: successful percutaneous drainage. Radiology 155(1): 73-75.
-
Sacks D, Robinson ML (1988) Transgastric Percutaneous Drainage of Pancreatic Pseudocysts. AJR Am J Roentgenol 151(2): 303-306.
-
Ho CS, Taylor B (1984) Percutaneous transgastric drainage for pancreatic pseudocyst. AJR Am J Roentgenol 143(3): 623-625.
-
Mallick IH, Winslet MC (2004) Vascular complications of pancreatitis. JOP J Pancreas 5(5): 328-337.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage