CT Evaluation of the Rupture of the Proximal Collecting System by Distal Ureteral Microlithiasis-Literature Review and Case Report
Ureteral rupture is a potentially dangerous event, the diagnosis of which is often delayed because of its rarity. Spontaneous ureteral rupture is a rare condition and ureteral calculi are the most frequent causes. In some cases, the cause is unknown. The diagnosis is made by computed tomography, the non-contrast phase shows the stone in the ureter and the excretory phase shows contrast extravasation, confirming the rupture. Management of the spontaneous ureteral rupture is not standardized because few systemic reports are available now. The conduct with minimally invasive procedures or conservative treatment yields the best results.
Introduction
Ureteral rupture (UR) is a potentially dangerous event, the diagnosis of which is often delayed because of its rarity [1]. Spontaneous ureteral rupture (SUR) is defined as nontraumatic urinary leakage from the ureter. It is a rare condition and also a potential urologic emergency. It is usually caused by ureteral obstruction by a calculus, stricture, or a tumor. Rupture may occur anywhere along the urinary tract, with the commonest sites being the fornices and upper ureter [2]. The UR may be evaluated by intravenous pyelography (IP), ultrasound (US) or computed tomography (CT). Management of the SUR is not standardized because few systemic reports are available now [3, 4]. We report a case of SUR of the proximal ureter with no evidence of an underlying pathological condition. Review of literature com emphasis in the diagnosis, follow-up and therapeutic approach is discussed.
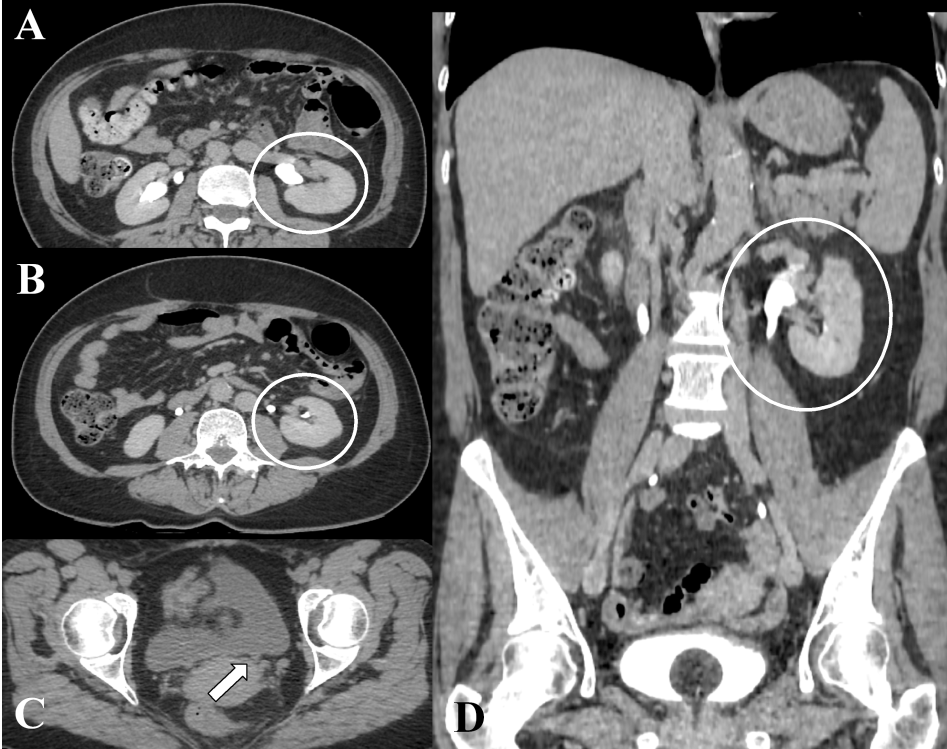
A 55-year-old woman complaining of severe left hypochondrium pain with radiation to perineum associated with nausea and vomiting without fever. She sought emergency medical attention. Denies renal calculus or any previous pathology. Do not use any medication regularly. Her abdomen was non-peritonitic and she was haemodynamically stable and afebrile. She was given analgesia with no effect. Urinalysis revealed microscopic haematuria; whilst blood investigations were within normal limits. A non-contrast abdominal CT was performed which showed a 2 mm stone in the distal part of the left ureter and upstream dilatation (Figures 1A &1B). The left kidney and upper third of the ureter on the same side had poorly defined limits associated with fat densification (Figure 1C). It was complemented with intravenous CT in the arterial, portal and excretory phases showing the extravasation of the venous contrast medium (Figures 2A & 2C). There was also a small aneurysmatic dilatation at the left renal artery near to renal hilum with no inflammatory signs or evidence of perianeurysmatic fibrosis (Figure 2B). The patient was hospitalized for support and conservative treatment was decided. The patient underwent control CT after two days of hospitalization and no longer shown contrast extravasation (Figures 3A, B & D). The stone was eliminated (Figure 3C).
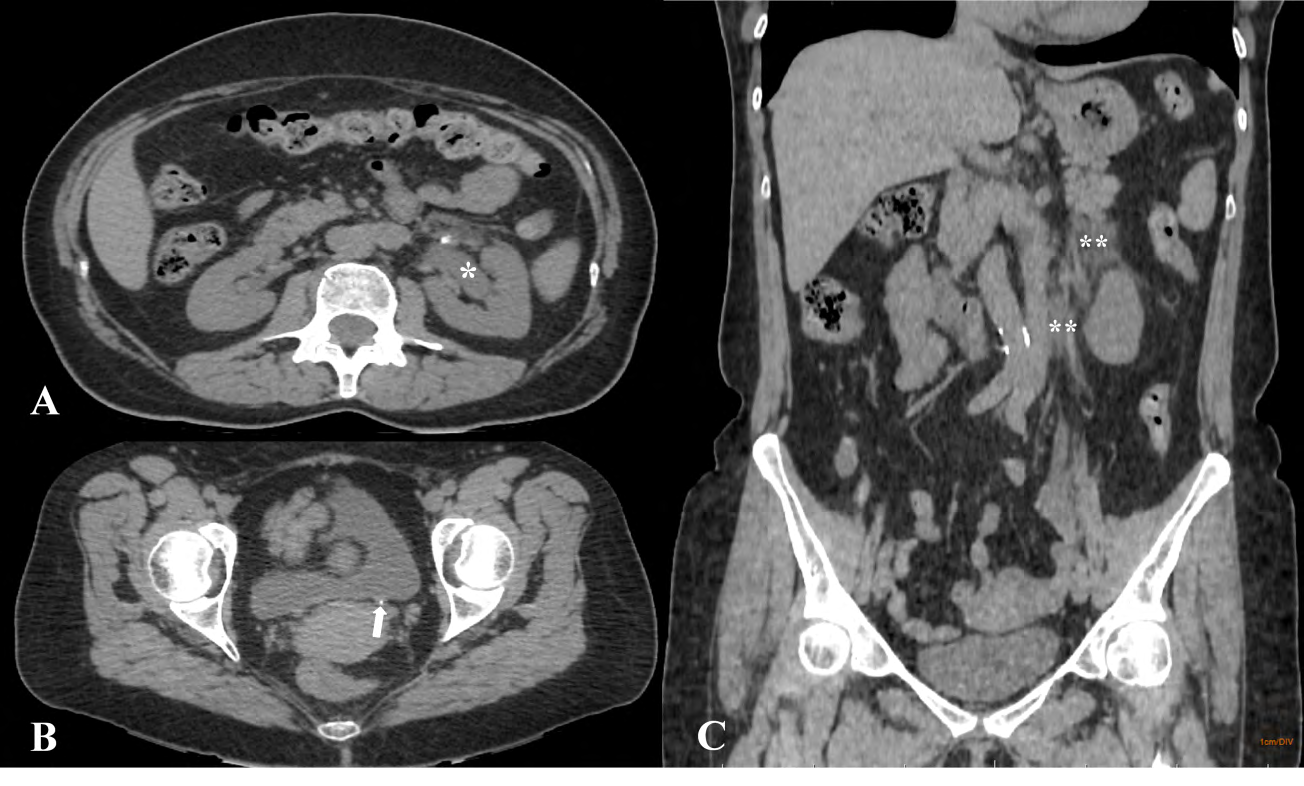
Figure 1: Abdomen CT without contrast, A) Axial plane shows upstream dilatation (white asterisk), B) axial plane shows a 2 mm stone in the distal part of the left ureter (white arrow), C) coronal plane shows the left kidney and upper third of the ureter on the same side had poorly defined limits associated with fat densification (double white asterisk).
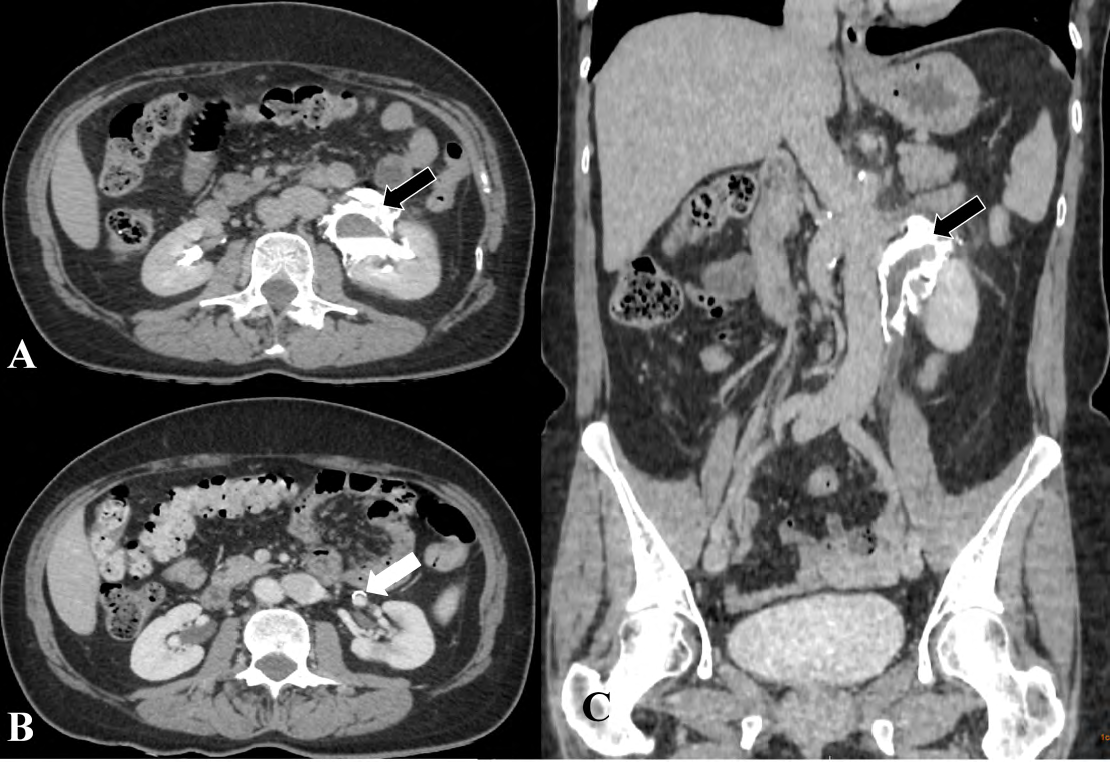
Figure 2: Abdomen CT with intravenous contrast, A) Axial plane, C) Coronal plane: the excretory phases showing the extravasation of the venous contrast medium after venous contrast (black arrow), B) Axial plane: the arterial phases showing small aneurysmatic dilatation at the left renal artery near to renal hilum with no inflammatory signs or evidence of perianeurysmatic fibrosis (white arrow).
Discussion
Ureteral rupture (UR) is in itself an infrequently entity. Its may be spontaneous or posttraumatic. The SUR is even rarer [5]. First cases of SUR were described in 1856 by Diaz and Buenrostro [4] and ureteral calculi is the most frequent causes [3, 4, 5, 6]. No plausible explanation has yet been published in the literature to explain a SUR and only theoretical mechanisms have been proposed. Impaction of stones on the ureter wall, or a downward moving calculus, which may cause erosion and ulceration of the ureteral wall, may lead to UR at the distal ureteral obstruction [6]. It’s no any gender differences [3, 4, 5, 6].
Others causes are tumors, retroperitoneal fibrosis, pregnancy, bladder outlet obstruction, connective tissue disease, high-dose corticosteroid treatment and chemotherapy [3, 4, 5, 6, 7]. It also might occur when the upper third of the ureter is fixed in its position by an ectopic vessel or scars because of previous trauma [7]. In some cases, the cause is unknown. Disorders causing fibrotic changes such as Klinefelter syndrome have also been proposed to be causes of SUR [6]. Out of 91 reported cases of SUR gathered by Akpinar H, et al. [8], 72% of cases reported stone disease as the etiology [3, 4]. Koga S, et al. [9] Reported 11 cases of spontaneous peripelvic extravasation due to ureteral calculus. Stravodimos K, et al. [10] reported five cases of SUR; one patient had a stone, but four had no obvious cause of rupture.
Schwartz A, et al. [11] reported a case of rupture of the ureter and used the term ‘spontaneous’ when there was: (a) no external trauma; (b) no cystoscopic ureteral manipulation; (c) no external compression; (d) an absence of destructive kidney disease; and (e) no history of any previous surgery. Choi SK, et al. [1] reported a case of upper UR, caused by urinary retention due to neurogenic bladder, and Yoshii T, et al. [12] reported a patient with malignant lymphoma, which was the cause of SUR [6]. In 2016 Bolat D, et al. [13] reported a case of SUR in a patient with polyarteritis nodosa.
Sato H, et al. [14] in 2018 reported a case of SUR caused by iliac aneurysm. The majority of ureteral obstruction cases involve inflammatory aneurysms or retroperitoneal fibrosis associated with perianeurysmal fibrosis that ultimately results in the structural compromise of the urinary tract. Similarly entrapment of the ureter can occur due to the extension of perianeurysmal inflammation into the surrounding tissue in degenerative aneurysms. Serra RM, et al. [15] reported that ureteral obstruction does not occur from the bulging of the aneurysm itself, but rather from the perianeurysmal inflammatory and fibrotic processes. However, with a rapid expansion of an aneurysm with impending rupture, the bulge might induce ureteral extravasation before the compensatory mechanisms of the ureter can function [14]. Our patient had a small left renal artery aneurysm without associated inflammatory characteristics and with-out fibrosis, so it cannot correlate the SUR with the presence of aneurysm.
A retrospective study by Gershman B, et al. [16] with 108 patients who were identified with the CT diagnosis of renal “forniceal” or “calyceal” rupture showed that the distal calculi in the ureter had a higher rate of spontaneous ureteral rupture than proximal stones (24.3% vs 76.7%). One possibility would be that smaller distal stones create higher intraureteral pressures than larger proximal stones because of the greater length of obstructed ureter and the smaller diameter of the distal ureter. The same author reported forniceal rupture was most commonly associated with distal ureteric calculi, with 75.7% of offending stones being located below the sacroiliac vessels. Calculi were small, with a mean stone size of 4.09 mm, and stone size decreased significantly from proximal-to-distal, with proximal calculi being significantly larger than distal calculi, which in turn were significantly larger than vesico-ureteric junction (VUJ) calculi.
A possible explanation for these findings is selection bias, in which smaller stones are more likely to pass distally to the VUJ where they ultimately obstruct. A study by Eisner BH, et al. [17] showed no significant difference in proximal vs distal ureteric caliber for normal ureters in patients with contralateral obstructing stones, suggesting that the caliber of the ureter itself is probably not responsible for these findings. When comparing stone size by ureteric location, proximal stones, with a mean (SD) diameter of 5.34 (1.87) mm were larger than distal stones, with a mean (SD) diameter of 4.08 (1.69) mm, which in turn were larger than VUJ stones, with a mean diameter of 3.53 (1.96) mm (P=0.005). In our case, the patient presents calculus measuring 2.0 mm; therefore, it has size and location compatible with cases of sur described in the literature.
SUR often produces symptoms such as sudden onset severe abdominal or flank pain associated with nausea and vomiting. Chen GH, et al. [3] reported most of the patients had acute flank pain (66.7%), and acute abdominal pain (33.3%). The symptom at presentation, mainly sudden, severe lower abdominal pain is usually not in sync with the clinical signs and may mimic an episode of acute appendicitis or diverticulitis5. Another report described massive urinary leakage into the peritoneal cavity, resulting in abdominal compartment syndrome, respiratory distress, and anuria [1, 3, 7]. Urine extravasation may be clinically occult or lead to acute abdomen symptoms. Hydronephrosis, paralytic ileus, electrolyte imbalances, or abscess formation may accompany the condition [1, 4, 6, 17, 18].
The diagnosis of renal forniceal rupture is made based on the presence of any one of the criteria: irregularity of a single renal calyx; loss of the ability to discern renal sinus fat; asymmetrically-distributed perinephric stranding; and a discreet perinephric fluid collection [5, 16]. Plain X-ray study of the abdomen, serial US and color duplex Doppler US are used to evaluate the urinary system at the initial stage [6, 7, 8, 9, 10, 13, 18]. Plain film of the abdomen may show a loss of retroperitoneal landmark, stone, and signs of paralytic ileus [4, 6]. The US represents the first line of investigation for renal colic. It can identify the presence of hydronephrosis, calculi within the renal pelvis, and perinephric urinoma, which appears as well-defined clear fluid collections [4, 6]. Serial US may show the obstruction site and fluid extravasation. Resistance index and pulsality index values in the renal interlobars arteries evaluated by color duplex Doppler US, significantly increase with acute hydronephrosis, and decrease after the elimination of the obstruction [10, 18]. US could be used as a simple screening tool but is often not accurate enough [7, 8].
IP has been described as the most sensitive means of diagnosing UR, is a useful tool for visualising the urinary tract. Recently, CT scanning is considered the optimal evaluation for diagnosing, because of the expected poor resolution of IP in an unprepared patient [1, 5, 11]. Intravenous contrast- enhanced CT is the most informative modality and has a higher sensitivity than other imaging modalities. The location and degree of leakage can also be readily assessed by CT. False negative results are reduced based on the results of abdominal plain radiography in the excretory phase [6, 7, 18]. In our patient, we diagnosed ureteral rupture via the extravasation of contrast medium from the perforated ureter with delayed contrast-enhanced CT. IP and CT with delayed images (obtained 5-20 min after contrast medium injection) show contrast medium extravasation in the peripelvic, perinephric, or retroperitoneal spaces [1, 5, 6, 7, 8].
In stable patients, contrast-enhanced CT should be performed to define an exact extent of the lesion and to provide detailed information about associated intra- abdominal or retroperitoneal injuries [7]. Whilst US can be helpful in identifying a perinephric or retroperitoneal fluid collection, the condition is best diagnosed with a delayed CT scan post-intravenous contrast. This modality will confirm a urinary leak and can accurately define the site of rupture. Coronal reconstructions may further help in accurately identifying the site of leak. The use of a delayed film post IV contrast is also very useful in differentiating a ureteral rupture from an infective perinephric abscess that can also arise from obstructing calculi. It can also differentiate from forniceal rupture [2, 8]. SUR can have serious consequences, including urinoma, perinephric or retroperitoneal abscess formation, and urosepsis. Consequently, spontaneous ureter rupture should be treated promptly [6].
Management of the SUR is not standardized because few systemic reports are available now. In Chen GH, et al. [3] series, primary ureteroscopy to set double ureteral stents was successfully performed in 13 patients (72.2% without complication). The average duration of double J (D-J) stents was 21 days (range, 8-45 days). All patients had good outcomes with a mean follow-up of 12.5 months (range, 0-52) [3]. Minimally invasive procedures or conservative care offer excellent results, and several case reports confirm this. Stavodimos K, et al. [10] reported on five patients managed successfully with a D-J ureteral stent insertion under fluoroscopy. Csata S, et al. [19] reported 2 patients with spontaneous ureteral rupture cured by conservative therapy. Akpinar H, et al. [8] successfully managed one patient by a D-J stent, one patient with acute urinary retention by urethral catheterization and 2 patients by conservative therapy.
Conclusion
Ureteral rupture is in itself an infrequently encountered entity and a spontaneous rupture is even rarer. The diagnosis is made by CT, the non-contrast phase shows the stone in the ureter and the excretory phase shows contrast extravasation, confirming the rupture. Conduct with minimally invasive procedures or conservative treatment yields the best results.
References
-
Choi SK, Lee S, Kim S, Kim TG, Yoo KH, et al. (2012) A Rare Case of Upper Ureter Rupture: Ureteral Perforation Caused by Urinary Retention. Korean J Urol 53(2): 131- 133.
-
Pace K, Spiteri K, German K (2016) Spontaneous proximal ureteric rupture secondary to ureterolithiasis. J Surg Case Rep 2016(11).
-
Chen GH, Chen CC, Chang YH, Chou E, Hsiao PJ, et al. (2014) Spontaneous ureteral rupture and review of the literature. Am J Emerg Med 32(7): 772-774.
-
Pampana E, Altobelli S, Morini M, Ricci A, Onofrio SD, et al. (2013) Spontaneous Ureteral Rupture Diagnosis and Treatment. Case Report Radiol 2013.
-
Aggarwal G, Adhikary SD (2016) Spontaneous ureteric rupture, a reality or a faux pas?. BMC Urol 16: 37.
-
Eken A, Akbas T, Arpaci T (2015) Spontaneous rupture of the ureter. Singapore Med J 56(2): 29-31.
-
Kulkarni PM, Mukha RP, Kekre NS (2014) Ureteropelvic Junction Rupture-An Unusual Presentation of Distal Ureteric Calculus. Urol J 10(4): 1151-1153.
-
Akpinar H, Kural AR, Tufek I, Obek C, Demirkesen O, et al. (2002) Spontaneous ureteral rupture: is immediate surgical intervention always necessary? Presentation of four cases and review of the literature. J Endourol 16(3): 179-183.
-
Koga S, Arakaki Y, Matsuoka M, Ohyama C (1992) Spontaneous peripelvic extravasation of urine. Int Urol Nephrol 24(5): 465-469.
-
Stravodimos K, Adamakis I, Koutalellis G, Koritsiadis G, Grigoriou I, et al. (2008) Spontaneous perforation of the ureter: clinical presentation and endourological management. J Endourol 22(3): 479-484.
-
Schwartz A, Caine M, Hermann G, Bittermann W (1966) Spontaneous renal extravasation during intravenous urography. Am J Roentgenol Radium Ther Nucl Med 98(1): 27-40.
-
Yoshii T, Horiguchi A, Shirotake S, Tobe M, Hayakawa M, et al. (2010) Spontaneous rupture of the ureter as the primary symptom of malignant lymphoma. Hinyokika Kiyo 56(11): 639-643.
-
Bolat D, Zumrutbas AE, Baser A, Tuncay L (2016) Spontaneous ureteral rupture in a patient with polyarteritis nodosa. Int Urol Nephrol 48(2): 223-224.
-
Sato H, Kurumisawa S, Saito T, Kawahito K (2018) Spontaneous ureteral rupture caused by iliac aneurysm: a case report. Surg Case Rep 4: 146.
-
Serra RM, Engle JE, Jones RE, Schoolwerth AC (1980) Perianeurysmal retroperitoneal fibrosis: An unusual cause of renal failure. Am J Med 68(1):149-153.
-
Gershman B, Kulkarni N, Sahani DV, Eisner BH (2011) Causes of renal forniceal rupture. BJU Int 108(11): 1909- 1911.
-
Eisner BH, Pedro R, Namasivayam S, Kambadakone A, Sahani DV, et al. (2008) Differences in stone size and ureteral dilation between obstructing proximal and distal ureteral calculi. Urology 72(3): 517-520.
-
Searvance K, Jackson J, Schenkman N (2016) Spontaneous Perforation of the UPJ: A Case Report and Review of the Literature. Urol Case Rep 10: 30-32.
-
Csata S, Repassy D, Weninger T, Tamas G (1998) Spontaneous (renal) pelvic rupture. Two cases cured by conservative therapy. Int Urol Nephrol 30(1): 19-24.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage