Radiological, Endoscopic, and Functional Disorders in Children with Respiratory Diseases Complicated by Respiratory Failure
Purpose: The aim of this study was to reveal the correlation between clinical, radiological, functional patterns in comparison with bronchofibroscopy and morphocytological studies of children with respiratory diseases complicated by respiratory failure (RF). Materials and Methods: The prospective study, conducted from 2000 to 2020, included 305 children aged from 1 day to 18 years with respiratory diseases complicated by RF (acute and chronic) of varying severity. After the initial ICU examination and hospital examinations, children of the examined group underwent the definition of the degree of RF and radiological examination. All the children underwent bronchofibroscopy, during the stabilization of the process or convalescence acute RF and with chronic RF during the remission of the disease underwent evaluation of the mucociliary apparatus by means of a bronchial biopsy of the bronchial mucosa. 68 сhildren and adolescents performed a comprehensive function of external respiration study. Results: Acute RF of II-III degree was noted for 228 children (75% of the total number): all of them were newborn babies (89), for 70% of children in early childhood (96) and older children (43). Chronic RF (CRF) was noted for 77 children (25%). 6 to 20 years after the initiation of the disease 45% of them were still under observation and had CRF. X-ray abnormalities revealed in 239 children (79%). For neonates there was a significantly bigger (76.4%, p <0.001) increased interstitial markings. CT result’s evaluation of children with CRF showed that reliably often, in 59% of cases, there were overinflation with areas of consolidation and air traps (p <0.001). Catarrhal changes in the mucous membrane of bronchi were revealed endoscopically in 94% of the patients, with predominantly mucosal hypersecretion in 74%. Obstructive disorders were detected during complex research of external respiration in 2/3 of examined patients. Conclusion: Clinical and radiologic features of pulmonary diseases complicated by RF in different periods of childhood are of the same type. Exception is increased airiness of the pulmonary tissue with upper respiratory defects and an overinflation with areas of consolidation in children of the older age group with CRF. The main causes of RF in newborns are functional and anatomical narrowing of the respiratory tract. Diagnostic bronchofibroscopic should be performed at the earliest possible time for children with stridor breathing and hyperinflation and children on artificial lung ventilation to identify congenital malformations as a cause of RF
Introduction
Diseases of the respiratory organs take a leading position in the structure of children diseases and they are the main and/or competing cause of children deaths in the first years of life [1, 2, 3, 4]. Diseases of the respiratory tract represent significant diagnostic difficulties, due to nonspecificity and symptoms duplications for different diseases, which demonstrates the importance of the problem and a vital necessity of improved diagnostic methods, prevention and treatment of bronchopulmonary diseases [2, 3, 5, 6, 7].
Respiratory failure (RF) is a serious complication of respiratory diseases, which develops due to ineffective gas exchange, impaired ventilation function of the lungs or a combination of these processes [8, 9, 10, 11]. Early diagnosis of the form of RF with the aim of effective correction of gas exchange remains an important problem in the treatment of children respiratory tract diseases. The solution of this problem is more relevant for young children in connection with the anatomical features of the respiratory tract, which largely determine the severity of RF [4, 12].
Comparative evaluation of endoscopic, radiologic and functional children disorders with respiratory disease complicated by RF remains insufficiently studied, which delays the process of establishing the correct diagnosis, the appointment of pathogenetic treatment, and increases the percentage of chronic diseases and mortality of patients [8, 12].
The aim of this study was to reveal the correlation between clinical, radiological, functional patterns in comparison with bronchofibroscopy and morphocytological studies of children with respiratory diseases complicated by RF.
Materials and Methods
The prospective study, conducted from 2000 to 2020, included 305 children aged from 1 day to 18 years with respiratory diseases complicated by RF (acute and chronic) of varying severity. The main part of the analyzed group was made up of young children: newborns, infants and toddlers (45%). In the present study, the absolute number of boys (170 children, 57%) exceeds the number of girls (135 children, 43%).
Clinical and Instrumental Studies
After the initial ICU examination and hospital examinations, all the children of the examined group underwent the definition of the degree of RF (acid-base state, transcutaneously saturation with O2-SaO2) and chest X-ray and computer tomography (CT) with the Swissray ddRFormula Plus, Siemens Polymobil Plus, Siemens Somatom 16. X-rays and CT scans were performed using pediatric protocols and ALARA-principle. All chest X-ray and CT images were reviewed with the consensus of pediatric radiologists (with more than ten years of pediatric radiology and chest radiology experience and with more than twenty years of pediatric radiology and chest radiology experience).
Childhood and adolescents performed a comprehensive function of external respiration (FER) study (pulse oscillometry, spirometry, general body plethysmography (GBP), diffusion capacity of the lungs (DCL)) on the equipment of the company JAEGER (Germany): Master Screen IOS (MS- IOS) digital, MS-PFT (analyzer unit), MS-Body.
All the children of the examined group underwent bronchofibroscopy. Modern flexible fibro- and video endoscopes were used, the choice of the bronchoscope’s diameter depended on age. In case of necessity of conducting studies with controlled lung ventilation, a children’s rigid bronchoscope was used. The presence of a mobile endoscopic rack with a full set of instruments and apparatus allowed performing manipulations in the resuscitation department, operating rooms (during surgery), bandaging rooms. Material sampling (bronchial flushing) was manufactured into standard sterile safes. Also, the material was sampled using the method of bronchoalveolar lavage.
228 children with acute RF during the stabilization of the process or convalescence and 77 with CRF during the remission of the disease underwent evaluation of the mucociliary apparatus by means of a bronchial biopsy of the bronchial mucosa and / or the nasal mucosa in the first 5-15 min after the removal of the material in smears. Single-use cytological brushes were used to conduct endobronchial brush biopsy.
Brush biopsy specimens of bronchial and nasal mucosa were examined with the method of intravital telescopic microscopy (color digital camera RGB MMC-31C12-M-MM, ½ proscan, 2048x1536 with cated by acute and CRF, were examined PC and ММС ММ software) and morphometry with the help of high-resolution microscope and specially created computer program.
In the native material was carried out in smears prepared after centrifugation by liquid cytology and stained with Harris’s hematoxylin according to Papanikolaou, eosin- methylene blue in May-Grunwald, Gram and Ziehl–Neelsen. The metaplasia of the bronchial epithelium, the dystrophic changes and the nature of the inflammation were evaluated, in comparison with the average cytological parameters of the bronchocytogram norm (alveolar macrophages 87.5%, eosinophils 1.6%, lymphocytes 3.5%; neutrophils 4%). With pronounced morphometric changes and motor disturbances, electron microscopy of the material was carried out in the laboratory of structural and functional proteomics.
Statistical Analysis
Chi-square test was used to analyse differences between proportions with a 0.05 level of significance. The prevalence of different agents was analysed as a function of radiographic finding sand age by fitting a logistic regression model.
Results
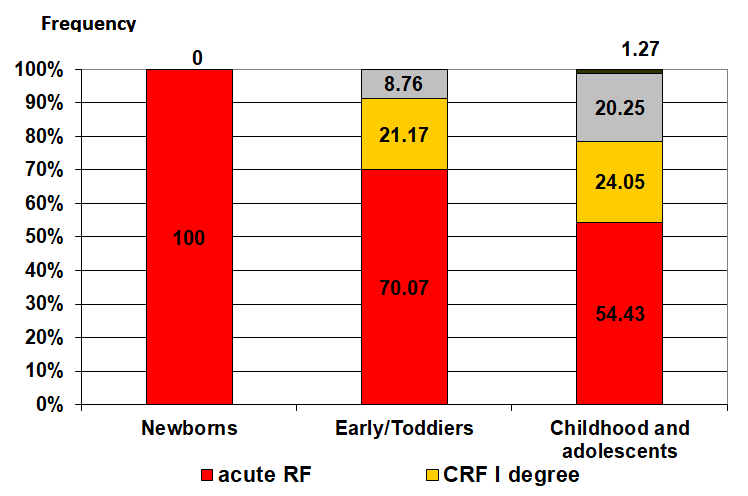
Nosological forms of respiratory diseases complicated by RF at different ages are given in Table 1. RF degrees differed at different age groups (Figure 1). Acute RF of II- III degree was noted for 228 children (75% of the total number): all newborn of current study (89), for 70% of children in early childhood (96) and 54.4 % older children (43). CRF was noted for 77 children (25%): I degree - for 48 children (15.7%), among them 29 young children (21%) and 19 older children (24%); II degree - for 28 children (9%), among them 12 children of an early age (9%) and 16 older children (20%); III degree – only one infant (0.33%) and older children (1.27%). The degree of RF in all age groups determined by obstructive syndrome, which was noted for 260 children (85%) and was absent only for 45 examined children (15%) (Table 2).
| Nosological forms | Children, qty | |||
|---|---|---|---|---|
| Newborns (0–28 days) 89 children | Infants and toddlers (29 days–3 years) 137 children | Childhood and adolescents (3–18 years) 79 children | ||
| ARDS | 8 | 0 | 0 | |
| Tracheobronchitis, obstructive bronchitis, bronchiolitis | 14 | 29 | 7 | |
| Pneumonia with atelectasis | 8 | 18 | 17 | |
| Foreign bodies of the respiratory tract | 0 | 9 | 2 | |
| Burn injuries of the respiratory system | 0 | 1 | 9 | |
| Pneumothorax | 0 | 0 | 3 | |
| Bronchopulmonary dysplasia | 12 | 32 | 0 | |
| Obliterating bronchiolitis | 0 | 8 | 29 | |
| Respiratory diseases with inherited pattern* | 4 | 4 | 3 | |
| Bronchial asthma of severe course | 0 | 0 | 2 | |
| Interstitial lung diseases ** | 0 | 0 | 3 | |
| Malformations of the upper respiratory tract | 19 | 29 | 0 | |
| Malformations of the lower respiratory tract | 24 | 25 | 4 | |
| Obstructive Syndrome | Qty of children examined | |||
| newborns (0–28 days) 89 children | Infants and toddlers (29 days–3 years) 137 children | Childhood and adolescents (3–18 years) 79 children | TTL | |
| 16 | 19 | 10 | 45 | |
| Inspiratory | 5 | 21 | 0 | 26 |
| Expiratory | 17 | 62 | 36 | 115 |
| Mixed type | 51 | 35 | 33 | 119 |
| Children in group, qty | 89 | 137 | 79 | 305 |
Table 1: Nosological forms of respiratory diseases complicated by RF for examined children. * Sievert-Cartagener syndrome, Cystic
In assessing the radiological changes in children of different age groups, there were no significant differences. Normal airiness of the pulmonary tissue was noted only for 7 newborn (2.3%). Increased airiness was detected for 191 children (63%) and prevailed in all age groups (more often in the early period - 75%), but the reliability of the difference was not revealed. Decreased airiness (atelectasis, dystelectasis, consolidation) was noted for 102 children (33%), more often for adolescents with acute respiratory pathology (43%). Asymmetric airiness of the pulmonary tissue was noted for 4 children with pneumothorax (1.3%): for 2 - with posttraumatic and for 2 - with spontaneous. Increased airiness was reliably more frequent for children with upper respiratory tract defects, decreased airiness in groups of infancy and adolescents with acute RF.
X-ray abnormality were detected in 198 children. Most often, increased interstitial markings appeared to be reinforced for 239 children (79%). For neonates there was a significantly bigger (76.4%, p <0.001) increased interstitial markings due peribronchial and perivascular thickening (Table 3). In 23.4% of infants revealed interstitial edema. In 29% of childhood and adolescents, compared with other age groups, emphysematous areas and overinflation were more pronounced.
| Chest X-ray abnormalities | Qty of newborns examined | |
|---|---|---|
| Number | %in a group | |
| Absence | 7 | 8% |
| Abnormal densities/lucencies | 82 | 92% |
| Hyperinflation, including | 46 | 52% |
| Patches of peripheral atelectasis | 33 | 37% |
| Hypoinflation, including | 36 | 41% |
| Patchy opacity | 53 | 60% |
| Infiltrates | 4 | 4.50% |
| Atelectasis | 13 | 14.60% |
| Distelectasis | 15 | 17% |
| Infiltrates + atelectasis | 4 | 4.50% |
| Normal interstitial markings | 18 | 20% |
| Increased interstitial markings, including | 68 | 76% |
| Peribronchial thickening | 54 | 60.70% |
| Perivascular thickening | 17 | 19.10% |
| Decreased interstitial markings | 3 | 3.40% |
| Interstitial edema | 33 | 37% |
6 newborns and 20 infants with acute RF, 44 with chronic lung diseases of older age group complicated by RF had chest CT. Analysis chest CT results of newborns showed that non- homogeneity of ventilation with overinflation was reliably more frequent (p<0.001). CT detection of overinflation and air traps in 12 infants was also more frequent (p<0.001). Also, overinflation with multifocal consolidation and bronchiectasis was detected in 1 infant, with the preservation of these CT patterns during further observation.
CT result’s evaluation of children with chronic RF showed that reliably often, in 59% of cases, there were overinflation with areas of consolidation and air traps (p <0.001), which were detected on expiratory CT in children over 3 years of age (Figure 2). Rare interstitial lung diseases were diagnosed in 3,8% in the group of children and adolescents (Figure 3).
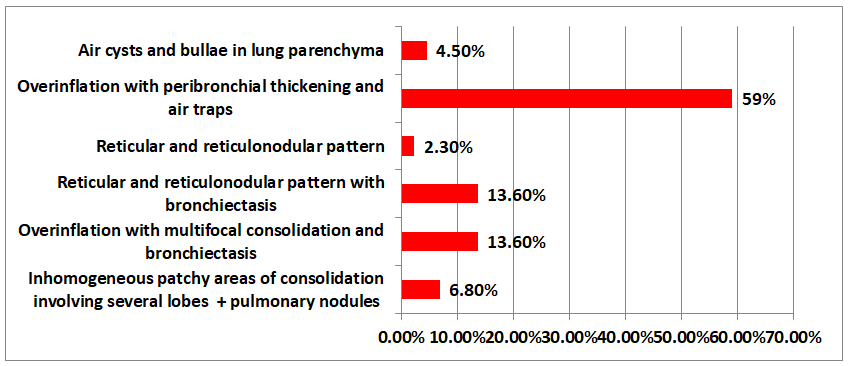
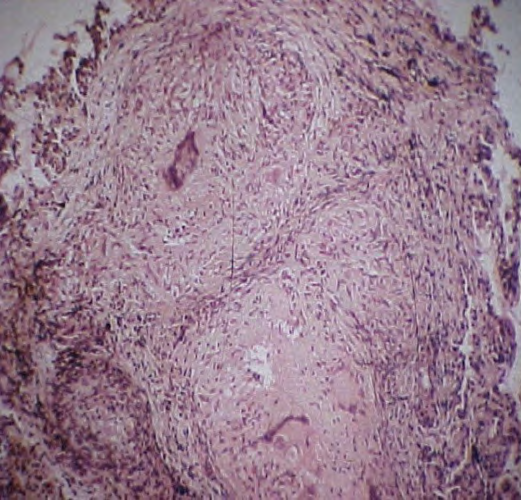
Figure 3b: Chest CT: bilateral perilymphatic nodules in the pulmonary parenchyma, typically - along the oblique interlobar pleura (white arrow).
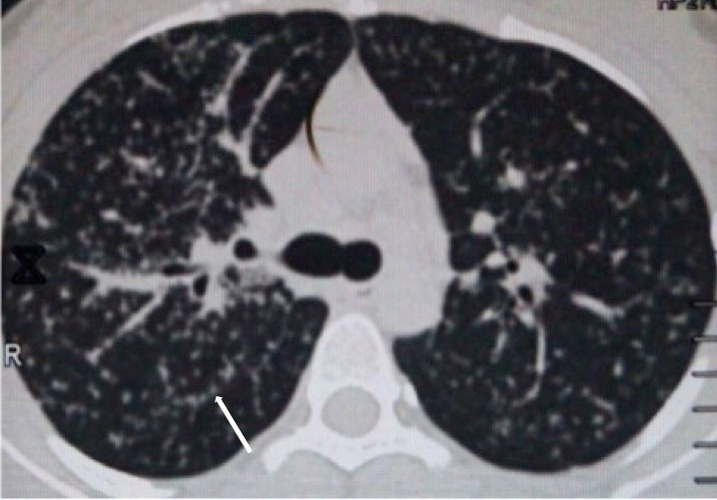
Figure 3c: Bronchofibroscopy: pronounced vascular pattern (black arrow) and tubercles under the mucous membrane of the tracheobronchial tree (white arrow). Taken biopsy and brush biopsy of the tubercle.

Figure 3d: Histologically: epithelioid cell granuloma of the sarcoid type.
All 305 children underwent a bronchofibroscopic examination. During bronchoscopic, the diffuse catarrhal changes in the mucous membrane of the trachea and bronchi (94%) with predominantly mucosal hypersecretion (74%) were most often detected. These inflammatory changes are due to the anatomical and physiological features of the respiratory tract of young children (Figure 4). The exception was children with burn injury, where deeper lesions of the mucous membrane with purulent-necrotic secretion in the respiratory tract were noted, and children with cystic fibrosis, which are characterized by the presence of viscous purulent sputum. It should be noted that in 32 infants with severe bronchopulmonary dysplasia (BPD), bronchoscopy revealed early signs of atrophic changes in the mucous membrane.

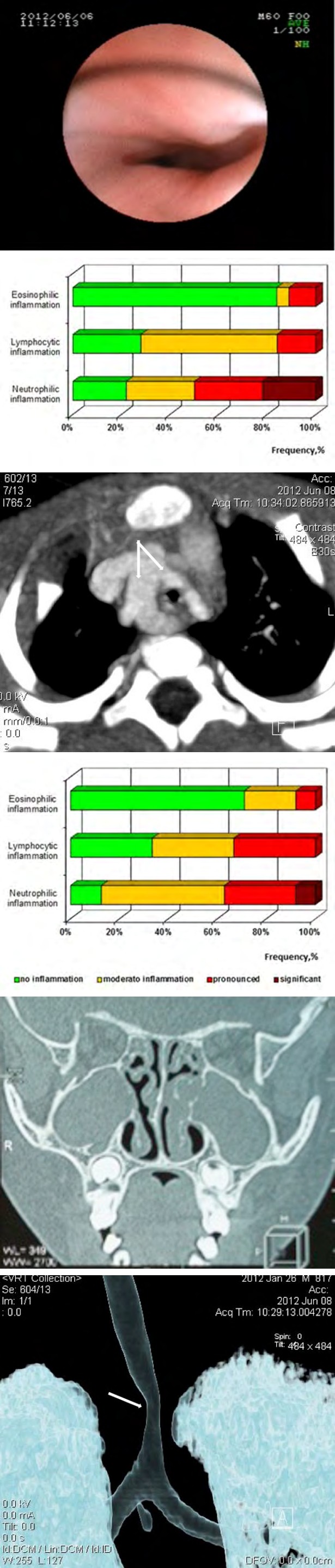
Figure 4b: Esophagogastroendoscopy: Compression deformation of the esophagus in the middle third. Vascular ring?
Figure 4c: Chest CT angiography: vascular ring - double aortic arch (white arrows).
Figure 4d: VRT reconstruction: tracheal stenosis is determined distinctly (white arrow).
All patients had a brush-biopsy of the bronchial mucosa was performed, with further study of the nature of the inflammatory changes and the state of the mucociliary system (Figure 5a, 5b). 5 children were first diagnosed with “primary ciliary dyskinesia” which was subsequently confirmed by the results of electron microscopy and genetic examination (Figure 6).
Figure 5a: The nature of inflammatory changes in the bronchial mucosa and the degree of their manifestation in acute RF.
Figure 5b: The nature of inflammatory changes in the bronchial mucosa and the degree of their manifestation in chronic lung diseases complicated by RF.
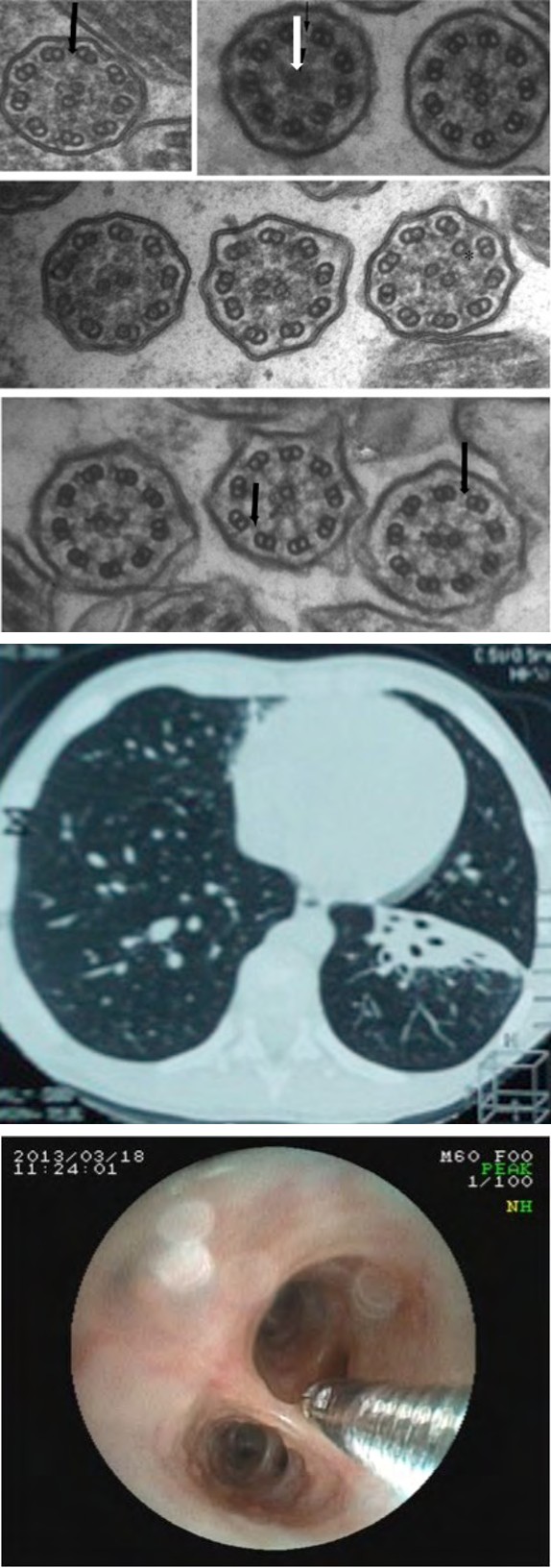
Figure 6b: Chest CT: atelectasis and bronchiectasis S8 left lower lobe. Inhomogeneous patchy area of consolidation S5 right middle lobe.
Figure 6c: Bronchofibroscopy: сatarrhal endobronchitis with mucous hypersecretion. Taking a biopsy.
Figure 6d: Transmission electron microscopy: ciliary ultrastructure abnormality - absence of the central axoneme (white arrow), microtubule disorganization, dynein arms are reduced (black arrows).
During the study, 68 children aged 7 to 17 years (86% of the total number of patients in the group, mean age 13.3 ± 2.5 years) underwent a comprehensive FER study. The normal speed indices for spirometry were recorded for 25 children (37%) of the study group. Violations of the patency of the airways were detected for 37 children (54.4%), and a decrease in the vital capacity of the lungs was observed for 9 children (13%). In the course of GBP, normal values were for 1/4 of the children (17 children, 25%), obstructive disorders for 45 children (66%), restrictive disorders - for 6 children (9%), for 5 of them, a decrease in DCL was noted (Table 4).
| Age | Children, qty | Normal GBP | Obstructive GBP | Restrictive GBP | |||
|---|---|---|---|---|---|---|---|
| Children, qty | % | Children, qty | % | Children, qty | % | ||
| 7 | 2 | 0 | 0 | 2 | 100 | 0 | 0 |
| 8 | 4 | 1 | 25 | 3 | 75 | 0 | 0 |
| 9 | 2 | 2 | 100 | 0 | 0 | 0 | 0 |
| 10 | 6 | 3 | 50 | 2 | 33.3 | 1 | 16.7 |
| 11 | 4 | 0 | 0 | 4 | 100 | 0 | 0 |
| 12 | 8 | 1 | 12.5 | 7 | 87.5 | 0 | 0 |
| 13 | 6 | 1 | 16.7 | 5 | 83.3 | 0 | 0 |
| 14 | 6 | 2 | 33.3 | 3 | 50 | 1 | 16.7 |
| 15 | 13 | 4 | 30.8 | 6 | 46.2 | 3 | 23.1 |
| 16 | 6 | 0 | 0 | 5 | 83.3 | 1 | 16.7 |
| 17 | 11 | 3 | 27.3 | 8 | 72.77 | 0 | 0 |
| TTL | 68 | 17 | 25 | 45 | 66.2 | 6 | 8.8 |
Table 3: Results of GBP in the group of childhood and adolescents.
The analysis of the conducted research shows that only for 1/3 of children the indices were close to the norm. The rest had different FER characteristic defects, the main changes were obstructive defects (66%), indirect signs of hyperinflation (65%), and an increase in RVL (49%). Restrictive changes were detected for 6 adolescents.
The Results of Observations of Children with Respiratory Disease Complicated By RF in the Dynamics
After the initial examination, the group of children was being observed and examined during 6-17 years. During the follow-up, the dependence of the outcome of the disease on the type of obstructive syndrome determining RF was studied. 163 children (53.4%) who did not form further chronic pulmonary diseases and were not examined by pulmonologists, in 35% of cases had an obstructive syndrome of the expiratory type, in 27% of cases - of a mixed type and in 25% - did not have obstructive syndrome. There were 136 children with CRF in the future (45.6%): 77 already had it at the time of the primary examination of CRF, and 59 children had formed CRF. In the group of children who developed RF, mild dyspnea was more common (51.5%), but the differences were unreliable.
Out of the entire group of observed patients, 5 children (1.97%) died in the early stages of the disease: 2 children with severe BPD and combined congenital malformations, 2 children with burn disease, and one child after autotrauma.
The group of infants and toddlers turned out to be the most prosperous, where more than a half of the children recovered (51%, p <0.01).
Discussion
Infection and anatomic malformations of the airways are the major causes of obstructive syndrome and RF in the infant population [6, 9, 11, 12]. Most cases of acute RF in children under 3 years of age are transient and secondary to an infectious etiology, usually a viral respiratory infection such as respiratory syncytial virus bronchiolitis. Anatomic malformations should be considered in young infants presenting with RF: congenital cardiac conditions resulting in pulmonary venous congestion can initially present as obstructive syndrome [11, 12, 13, 14]. Vascular rings/slings can obstruct airways causing obstructive syndrome, stridor, or respiratory distress [12]. “Noisy breathing” associated with tracheobronchomalacia is often interpreted by caretakers as obstruction [12, 15]. CRF necessitates consideration of diseases such as cystic fibrosis, primary ciliary dyskinesia, and gastroesophageal reflux [12, 14, 15]. Therefore, many different processes besides asthma may initially present with obstructive syndrome and it is important to create a broad differential during initial workup [5, 8, 9, 12, 16].
In the present study 305 children (135 girls, 170 boys) with respiratory diseases, complicated of RF, were examined. All newborns had acute RF due to upper airway obstruction (91%). In the neonatal period, obstructive syndrome of mixed type was significantly more frequent (57.3%, p <0.05), the expiratory type of obstructive syndrome (lower airway obstruction) prevailed for children of early (45%) and the older age group (46%), but the differences between the groups turned out to be unreliable. 45% of the examined newborns with acute RF developed CRF at an older age. In infants and children under 3 years of age, mixed type of RF was more often observed (67%), associated with age-related anatomical features of the respiratory tract.
In the group of childhood and adolescents, RF was also observed as a result of obstruction of the lower respiratory tract (98%), except for a group of children (of them 3 adolescents) with disseminated lung diseases (sarcoidosis, l_ymphangioleiomyomatosis_, histiocytosis X), where predominant restrictive type of RF (3.8%). In children with burn injury, RF was mixed.
Obstructive type of RF X-ray revealed as abnormal densities/lucencies in the form of overinflation with peribronchial thickening and air traps, inhomogeneous patchy areas of consolidation involving several lobes (Figure 2). Restrictive type of RF was predominantly presented as patchy opacity, ground glass opacities, multifocal consolidation with bronchiectasis, reticular and reticulonodular pattern, edema and cellular infiltrates. Mixed type of RF included a combination of both obstructive and restrictive patterns.
It is known that in infants and toddlers, bronchoscopy is indicated with an increased clinical suspicion of foreign body aspiration [2, 9, 17, 18, 19, 20]. Among the characteristics of indications for bronchoscopy for newborns and children of the first year of life, we also identified: asphyxia attacks associated with feeding, puffing during meals with coughing attacks, regurgitation with a full mouth, “draining” the food through the nasal passages, inability to breathe independently without an endotracheal tube with sufficient oxygenation of the arterial blood.
Diagnostic bronchoscopy for lungs diseases complicated by RF has proven itself to be an informative research method that provides an opportunity to assess the state of the tracheobronchial tree, reveal obstructive disorders in the trachea and bronchi, assess the nature of the inflammatory changes in the bronchial mucosa and the mucociliary system by additional methods of studying biological material, the degree of expression of mucostasis and other pathological states [21, 22, 23, 24, 25]. All 305 children of this study underwent a bronchofibroscopic examination. During bronchoscopic, the diffuse catarrhal endobronchitis (94%) with mucous hypersecretion of the trachea and bronchi (74%) were most often detected.
Analyzing the results of the study, it should be noted that for children with acute respiratory diseases, neutrophilic inflammation of the bronchial mucosa (Figure 5), while metaplasia of the ciliated epithelium and morphological changes in the ciliary apparatus are untypical, unlike dystrophic changes, which are found in all patients. Secondary motor disorders and a decrease in the number of cilia were observed in 50% of patients with acute respiratory diseases complicated by RF. For children with chronic lung diseases, lymphocytic-eosinophilic inflammation of the bronchial mucosa was more common, and marked metaplasia and dystrophy of the ciliated epithelium are characteristic (Figure 5). The pathology of the ciliary apparatus in the general group is not very acute, but a group of children (10%) with primary motor impairments was identified (Figure 6). In the native material, the cilia morphometry (length of the cilium, its shape) was carried out and the motor disturbances (synchronization of motion, mean frequency and duration of motor activity) were studied.
When comparing results for children of early and the older age group, endoscopic and radiographic changes were identical except for the increase airiness and overinflation in CRF for children of the older age group. When evaluating endoscopic changes in the group of children of early and the older age group, acute endobronchitis with mucous hypersecretion was significantly more frequent in acute RF.
Chest X-ray and CT made it possible to diagnose rare interstitial lung diseases in 3,8%, what changed the treatment of these patients.
Obstructive syndrome, which determined the severity of RF, was observed in the majority of children (more than 85%). Significantly more often, inspiratory obstruction was detected for young children.
45% of children formed CRF, when obstructive violations of bronchial patency and an increase in RVL were functionally noted. 54% of the examined children with acute RF in dynamics had no signs of hypoxemia, but retained bronchial hyperactivity.
Signs of hyperinflation and an increase in RVL in the study of GBR in 45 children over 7 years of age correlated with chest X-ray/CT patterns: increase airiness, overinflation and air traps. It should be noted that GBP is the most sensitive method of examining FER for children.
Conclusion
Clinical and radiologic features of pulmonary diseases complicated by RF in different periods of childhood are of the same type, there were no significant differences between age groups. Exception is increased airiness of the pulmonary tissue with upper respiratory defects and overinflation with areas of consolidation in children of the older age group with CRF.
Diagnostic bronchofibroscopic should be performed at the earliest possible time for children with stridor breathing and hyperinflation and children on artificial lung ventilation to identify congenital malformations as a cause of RF. The main causes of RF in newborns are functional and anatomical narrowing of the respiratory tract.
Endoscopically, diffuse catarrhal endobronchitis with mucosal hypersecretion predominated in all groups. For children with acute RF neutrophilic inflammation and secondary disorders of mucociliary clearance are characteristic. Children with CRF are characterized by pronounced metaplasia and dystrophy of the ciliated epithelium and lymphocytic-eosinophilic inflammation.
Author’s Contributions: All the authors were involved in the study design, date collection and writing of the manuscript.
Funding: The study received no funding.
Disclosure of Interest: The authors declare that they have no competing interest.
References
-
Rassiwala M, Lahoti BK, Mathur R, Laddha A, Sharma SS (2014) Failure of bronchoscopy in airway obstruction: A case series. J Assoc Chest Physicians 2(2): 90-93.
-
Black RE, Johnson DG, Matlak ME (1994) Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg 29(5): 682-684.
-
Bush A, Abel RM, Chitty LS, Harcourt J, Hewitt R, et al. (2019) Congenital lung disease. In: Wilmott RW, Deterding RR, Li A, Ratjen F, Sly P, et al. (Eds.), Kendig’s Disorders of the Respiratory Tract in Children, Philadelphia, PA: Elsevier, pp: 289-337.
-
Montella S, Corcione A, Santamaria F (2017) Recurrent pneumonia in children: a reasoned diagnostic approach and a single centre experience. Int J Mol Sci 18(2): 296.
-
Jung SY, Pae SY, Chung SM (2012) Three-dimensional CT with virtual bronchoscopy: a useful modality for bronchial foreign bodies in pediatric patients. Eur Arch Otorhinolaryngol 269(1): 223-228.
-
Kwok MM, Wong A, Paddle P, Goergen S, Rimmer J (2018) Clinico-radiological predictors of positive rigid bronchoscopy findings in children with suspected tracheobronchial foreign body aspiration. Aust J Otolaryngol 1(2): 11.
-
Annunziata F, Bush A, Borgia F (2019) Congenital lung malformations: unresolved issues and unanswered questions. Front Pediatr 7: 239.
-
Friedman ML, Nitu ME (2018) Acute Respiratory Failure in Children. Pediatr Ann 47(7): e268–e273.
-
Wong M, Bhatia R (2019) A 9‐month‐old with wheezing and acute hypoxic respiratory failure. Clin Case Rep 7(5): 976-980.
-
Faffe DS, Zin WA (2009) Lung parenchymal mechanics in health and disease. Physiol Rev 89(3): 759-775.
-
Brucknerova J, Babala J, Ujhazy E (2020) Rare Causes of Respiratory Insufficiency in Newborns Physiol Res 69(Suppl 4): S637-S647.
-
Fakhoury K (2018) Evaluation of wheezing in infants and children. In: Gregory R, Tepas E (Ed.), Waltham, MA: UpToDate.
-
Chon AH, Stein JE, Gerstenfeld T (2018) The use of fetal bronchoscopy in the diagnosis and management of a suspected obstructive lung mass. AJP Rep 8(3): e195-e200.
-
Shankar G, Kothari P, Sarda D, Kulkarni B, Kalgutkar A (2006) Pneumonectomyina child with congenital bronchiectasis: A case report and review of literature. Annals of Thoracic Medicine 1(2): 81-83.
-
Gaude GS (2009) Pulmonary manifestations of gastroesophageal reflux disease. Ann Thorac Med 4(3): 115-123.
-
Kann K, Long B, Koyfman A (2017) Clinical mimics: an emergency medicine‐focused review of asthma mimics. J Emerg Med 53(2): 195‐201.
-
DÉufemia MD, Clanci S, Meglio DF, Letizia DM, Lavinia DM, et al. (2016) Congenital high airway obstruction syndrome (CHAOS): discussing the role and limits of prenatal diagnosis starting from a single-center case series. J Prenat Med 10(1-2): 4-7.
-
Hegde SV, Hui P, Lee EY (2015) Tracheobronchial foreign bodies in children: imaging assessment. Semin Ultrasound CT MR 36(1): 8-20.
-
Pugmire BS, Lim R, Avery LL (2015) Review of ingested and aspirated foreign bodies in children and their clinical significance for radiologists. Radiographics 35(5): 1528- 1538.
-
Boufersaoui A, Smati L, Benhalla KN (2013) Foreign body aspiration in children: experience from 2624 patients. Int J Pediatr Otorhinolaryngol 77(10): 1683-1688.
-
Facciolongo N, Patelli M, Gasparini S (2009) Incidence of complications in bronchoscopy. Multicentre prospective study of 20,986 bronchoscopies. Monaldi Arch Chest Dis 71(1): 8-14.
-
Fidkowski CW, Zheng H, Firth PG (2010) The anesthetic considerations of tracheobronchial foreign bodies in children: a literature review of 12,979 cases. Anesth Analg 111(4): 1016-1025.
-
De Blic J, Marchac V, Scheinmann P (2002) Complications of flexible bronchoscopy in children; prospective study of 1,328 procedures. Eur Respir J 20(5): 1271-1276.
-
Petrella F, Borri A, Casiraghi M, (2014) Operative rigid bronchoscopy: indications, basic techniques and results. Multimed Man Cardiothorac Surg 2014: mmu006.
-
Najada AS, Dahabreh MM (2011) Bronchoskopy findings in children with recurrent and chronik stridor. J Bronchol Intervent Pulmonol 18(1): 42-47.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage