A Case Report of Simultaneous Bilateral Upper Limb CT Angiography
Diabetes mellitus leads to accelerated development of athermanous plaques in the arteries, which can lead to ischemia especially of the distal parts of the limbs, namely the fingers and digits. Bilateral upper limb ischemia is however an infrequently reported complication of patients with diabetes mellitus as compared to the lower limbs. However, it can have devastating consequences for the patient including ischemic necrosis and subsequent amputation of the fingers. Angiography is often required to assess the extent of the disease and to decide further management. CT angiography is a less invasive and effective method of assessment of vascular compromise. We are reporting a case where we performed bilateral upper limb CT angiography simultaneously to minimize the radiation burden to the patient and the potential for renal damage. The contrast was injected using a vein of the lower limb and bilateral athermanous plaques in the arteries visualized in a single scan.
Introduction
The second most frequent manifestation of atherosclerosis is peripheral arterial disease (PAD) [1]. PAD and consequent limb ischemia are a major cause of morbidity and mortality [2, 3, 4]. In the available literature, individuals with diabetes have between two to five fold increase in the odds of developing PAD [5, 6]. CT angiography provides three dimensional imaging of the entire vascular tree non-invasively leading to a high-diagnostic accuracy, an excellent temporal and spatial resolution and more than 90% sensitivity and specificity in detecting hemodynamically significant stenosis [7, 8, 9]. Most of the time the upper limb CT angiography is required for a single limb only, however in case of diabetes, multi-vessel vascular involvement may be present [8, 9, 10]. We are presenting a case report where we have performed the CT angiography of both the upper limbs vessels simultaneously using a single bolus that was delivered via a lower limb vein, to reduce the radiation burden and save time and cost.
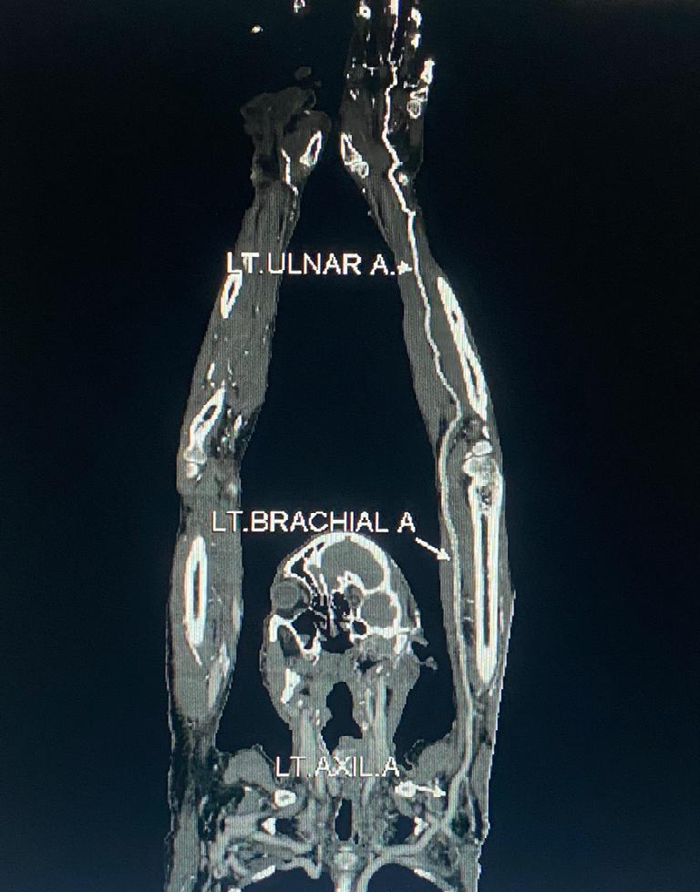
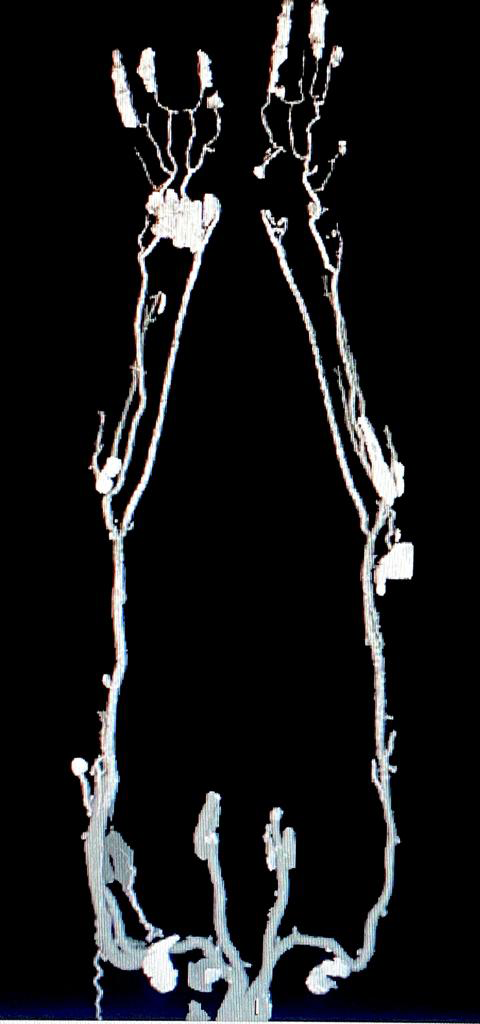
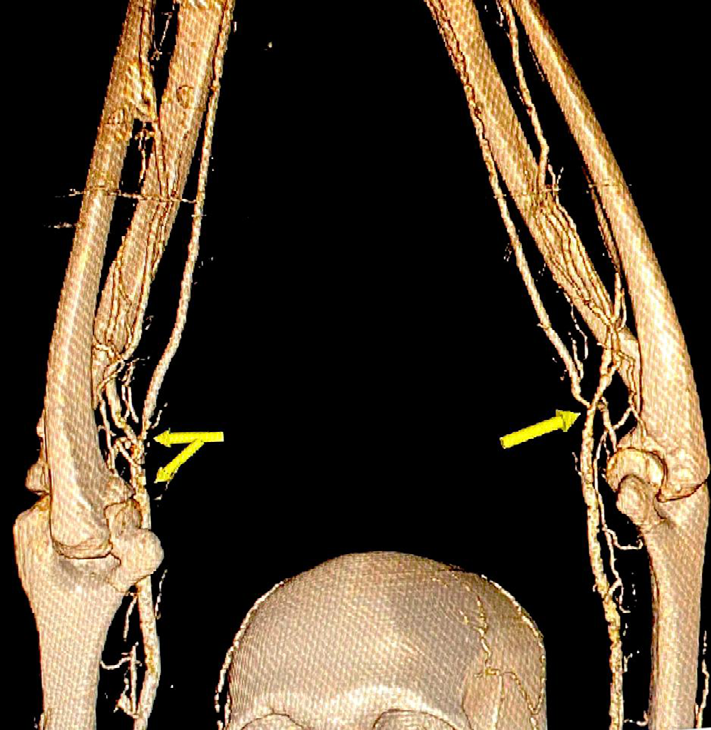
A 60-year-old male with chronic uncontrolled diabetes mellitus presented to the radiology department for CT angiography of the upper limbs. He suffered from chronic kidney disease and required dialysis every time radiography contrast was used. He had suffered from ischemia of the fingers with amputation of a finger of the right hand. A CT angiogram of the arms was required to see the cause and extent of the vascular compromise to the fingers. In order to reduce the patient’s radiation burden, and the chance of further renal damage, it was decided that both the arms would be scanned simultaneously to compare the arteries of both arms. The scan was performed with the patient in the prone position. Similarly, it was decided that the bolus would be injected in a suitable vein of the lower limb. 80 ml of a non- ionic contrast was injected at a flow rate of 4 ml/s. sure start technique was used using the manual technique once the bolus reached the arch of aorta. The scan revealed severe bilateral symmetrical athermanous calcified diffuse plaque disease extending from the level of the mid arm to the palmar branches of the radial and ulnar arteries leading to severe digital ischemia (Figures 1-4).

Discussion
Atherosclerosis is the most frequent large-vessel PAD in the upper limb [11]. Because of the rising frequency of chronic diabetes mellitus in the modern world, PAD is increasingly becoming a mounting healthcare problem [12]. As many as 16.2% of diabetics may present with PAD [12]. It
is estimated that for every 1% increase in haemoglobin A1C, there is a 26% increase in the risk of PAD [13]. Furthermore, diabetics have more aggressive PAD than non-diabetics, with early major vascular involvement and distal symmetrical disease [13]. CT angiography has the ability to accurately assess the extent of disease, delineate the vessel morphology and act as a guide for the management options. Due to its superior spatial resolution, CT angiography is optimal for assessing smaller vessels in the upper extremities [14, 15].
In our review of literature, we have not found a single of case of upper limb CT angiography where both the limbs were assessed simultaneously after injection of the contrast in the leg vein. This technique has the advantage of assessment of the vasculature of both the upper limbs with a single injection of radio-contrast thus reducing the radiation exposure and the chance of renal damage due to radiography contrast agent.
References
-
Beckman JA, Schneider PA, Conte MS (2021) Advances in Revascularization for Peripheral Artery Disease. Revascularization in PAD. Circ Res 128(12): 1885-1912.
-
Berger JS, Ladapo JA (2017) Underuse of Prevention and Lifestyle Counseling in Patients with Peripheral Artery Disease. J Am Coll Cardiol 69(18): 2293-2300.
-
Tolia J, Bhatt A (2020) Clinical experience of upper limb ischemia. A retrospective study. In Int Surg J 7(5): 1562.
-
Chidambaram PK, Swaminathan RK, Ganesan P, Mayavan M (2016) Segmental Comparison of Peripheral Arteries by Doppler Ultrasound and CT Angiography. J Clin Diagn Res 10(2): 12-16.
-
Wilcox T, Newman JD, Maldonado TS, Rockman C, Berger JS, et al. (2018) Peripheral vascular disease risk in diabetic individuals without coronary heart disease. Atherosclerosis 275: 419-425.
-
Lapeyre M, Kobeiter H, Desgranges P, Rahmouni A, Becquemin JP, et al. (2005) Assessment of critical limb ischemia in patients with diabetes. Comparison of MR angiography and digital subtraction angiography. AJR Am J Roentgenol 185(6): 1641-1650.
-
Schernthaner R, Fleischmann D, Stadler A, Schernthaner M, Lammer J, et al. (2009) Value of MDCT angiography in developing treatment strategies for critical limb ischemia. AJR Am J Roentgenol 192(5): 1416-1424.
-
Murphy DJ, Aghayev A, Steigner ML (2018) Vascular CT and MRI. A practical guide to imaging protocols. Insights Imaging 9(2): 215-236.
-
Shareghi S, Gopal A, Gul K, Matchinson JC, Wong CB, et al. (2010) Diagnostic accuracy of 64 multidetector computed tomographic angiography in peripheral vascular disease. Catheter Cardiovasc Interv 75(1): 23- 31.
-
Mohammedi K, Woodward M, Hirakawa Y, Zoungas S, Williams B, et al. (2016) Microvascular and macrovascular disease and risk for major peripheral arterial disease. Diabetes Care 39(10): 1796-1803.
-
Bae M, Chung SW, Lee CW, Choi J, Song S, et al. (2015) Upper Limb Ischemia. Clinical Experiences of Acute and Chronic Upper Limb Ischemia in a Single Center. Korean J Thorac Cardiovasc Surg 48(4): 246-251.
-
Dal Canto E, Ceriello A, Rydén L, Ferrini M, Hansen TB, et al. (2019) Diabetes as a cardiovascular risk factor. An overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol 26(2): 25-32.
-
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, et al. (2007) Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg 45: S5-67.
-
Fleischmann D, Hellinger JC, Napoli A (2005) Multidetector-Row CT Angiography of Peripheral Arteries: Imaging Upper-Extremity and Lower-Extremity Vascular Disease. Multidetector-Row CT Angiography pp: 187-198.
-
Ghouri MA, Gupta N, Bhat AP, Thimmappa ND, Saboo SS, et al. (2019) CT and MR imaging of the upper extremity vasculature. Pearls, pitfalls, and challenges. Cardiovasc Diagn Ther 9(1): S152-S173.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage