CT Image Quality Assessment by a Channelized Hotelling Observer: Optimization of Adaptive Statistical Iterative Reconstruction for Radiation Dose Reduction and Improving Image Quality of Pediatric Abdominal CT Scan
Background: Iterative reconstruction (IR) techniques have tried to reduce the radiation dose of computed tomography (CT) scans while maintaining the image quality. One of the IR techniques is the adaptive statistical iterative reconstruction (ASIR). Increasing the amount of ASIR in image reconstruction can lead to the emergence of artifacts and reduce the ability to detect objects with low contrast. Objective: This study aimed to optimize the ASIR technique to reduce the radiation dose and increase image quality in pediatric abdominal CT. Methods: This is a phantom study performed using variable tube current (40,100,140 and 200mA) and ASIR level (ASIR 10% to ASIR 100%). Various criteria including noise, high-contrast spatial resolution, and Channelized Hotelling observer’s model were used to compare image quality at different captured levels. In this study CHO model was used for low contrast detectability. Results: The result was quit promising in the term of CHO’s used for mentioned purposes. The noise of reconstructed images with 30% ASIR and higher levels had a significant difference compared to the reconstructed images by the Filter Back Projection (FBP) method (P < 0.05). The spatial resolution of the images with tube currents of 140, 100, and 40 mA reconstructed with 30, 50, and 80% levels of ASIR technique was equal to 0.8 ± 0.144 pairs of lines per millimeter. The amount of the spatial resolution of images obtained with standard radiation dose and reconstructed by FBP method was 1 pair of lines per mm (p> 0.05). Conclusion: Based on the results of this study, using 50% ASIR for the pediatric population can reduce the radiation dose on abdominal and pelvic CT scans by 50% while maintaining image quality. Furthermore using ASIR 50% only for the reconstruction of abdominal and pelvic images in children at standard radiation dose leads to optimal image quality.
Introduction
Although computed tomography produces high-quality and accurate images and is widely used in early medical diagnoses, it can be a relatively high radiation dose imaging test [1]. Previous studies have shown that while computed tomography accounts for only 15% of all imaging tests, it accounts for more than 75% of all radiation [2, 3, 4]. Besides, there are potential risks associated with ionizing radiation, such as cancer, especially for children. They are also more in danger of probable radiation hazards because of their long life expectancy [5]. For this reason, the radiology community has paid much attention to reducing the exposure of patients, especially children, through the optimization of scanning protocols. Companies manufacturing CT scanning systems also attempted to invent techniques to maintain or improve image quality while reducing the radiation dose. They have made it one of the main focuses of their research and development goals [6]. Low-dose CT imaging has always been difficult because reducing the dose increases the noise and reduces the image’s diagnostic quality.
Therefore, as part of image acquisition, most dose reduction techniques try to maintain image quality while reducing the amount of radiation by optimizing scan parameters such as scan time and tube current. Iterative reconstruction (IR) techniques have recently maintained or even increased the diagnostic quality of images using different strategies at low doses [6, 7]. One of the iterative reconstruction techniques is the adaptive statistical iterative reconstruction (ASIR). Despite the high processing speed and good image quality of the Filter Back Projection (FBP) reconstruction technique, it is weak in low-dose imaging. In addition, the images have lost their accuracy and diagnostic quality due to excessive noise and artifacts. However, the ASIR technique uses various complicated mathematical models to eliminate noise from low-dose images and maintain or improve image quality [6, 7, 8].
Although just using the ASIR technique in reconstruction can significantly reduce image noise, radiologists still use a hybrid reconstruction algorithm consisting of FBP and IR to reconstruct images. Radiologists decide how much ASIR to use (as a percentage) in image reconstruction in each imaging test. In many protocols that use the ASIR reconstruction technique, the value is set between 10 and 40% [7]. It means that the exposure can be reduced by 10 to 40% without jeopardizing image quality. Previous studies have also suggested a combination of 30-50% ASIR and FBP for abdominal and pelvic imaging in adults [9, 10, 11]. However, few studies have attempted to establish an appropriate reconstruction protocol in the pediatric population [12, 13, 14]. In most previous studies [9, 10] radiation dose and image quality have been optimized using patients. Using patients to optimize radiation dose may increase the dose received by patients, so in this study, phantom and model observer were used. The use of the model observer brings the results obtained in this study closer to the clinical results. In fact, The model observer represents the conditions of an ideal observer and predicts its performance. Today, various models observer have been developed to predict human observer performance [15]. One of these models is called CHO. The CHO model has been widely used in a variety of imaging modalities including CT scan, MRI, mammography and nuclear medicine [16, 17, 18, 19]. Furthermore, previous studies have indicated that increasing the amount of ASIR in image reconstruction can lead to the emergence of artifacts and reduce the ability to detect objects with low contrast [4]. Therefore, this study aimed to optimize the ASIR technique to reduce the radiation dose and increase image quality in pediatric abdominal CT.
Methods
CT scanner and phantom
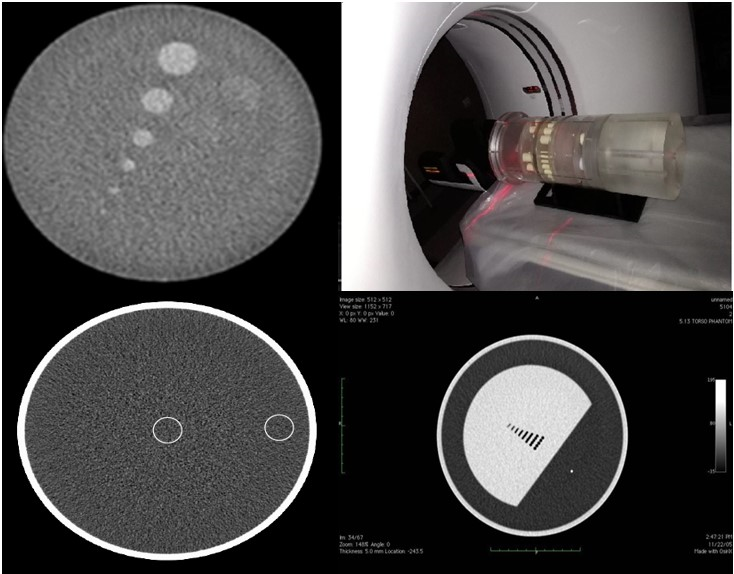
All experiments in this study were performed on a 64-slice scanner (GE Healthcare. Light Speed VCT). The BMMD-7 phantom made in the USA (Figure 1) was used to evaluate the image quality. This phantom consists of four sections to assess the parameters of low contrast resolution, spatial resolution, noise, and CT number accuracy. The diameter of the phantom was 16cm. It should be noted that despite significant changes in dimensions in the age group studied, the average standard diameter defined for children is 16 cm, so in this study, a phantom with a diameter of 16 cm was used.
Imaging of phantom was performed based on the scan parameters shown in Table 1. These parameters were selected according to the recommended scan conditions for imaging children’s abdomen and pelvis. To evaluate the impact of ASIR on the radiation dose, the scan was repeated with various mAs (140, 100, and 40 mA).
| Scanning parameters | |
|---|---|
| Tube voltage | 100 |
| Tube current | 200 |
| Rotation time | 0.5 |
| Slice thickness | 5 |
| Matrix | 512 ×512 |
| Pitch ratio | 1 |
Table 1: The scan parameters for a patient with an ideal weight.
Image reconstruction
All raw imaging phantom data obtained with tube currents of 200, 140, 100, and 40 mA were reconstructed by FBP and ASIR (ASIR 10% to ASIR 100%). A total of 396 image (FBP: four mAs setting * nine times repeating the scan; ASIR: four mAs setting * nine times repeating the scan* ten levels of ASIR) of the phantom were obtained according to different imaging parameters and different reconstructions.
Numerical measurement
Noise
The noise was determined on images of the uniform BMMD-7 CT module as the standard deviation of the pixel values in a square region-of-interest (ROI) situated at the center of the phantom module. To measure the noise of the obtained images, a central ROI of 500 pixels was immersed in the center of the water phantom image, and four other ROIs of the same size were located at a distance of one centimeter from the edges of the phantom, and finally, the standard deviation of CT numbers was reported as the image noise. To reduce error and get the right results, each of the noise values shown in this study was obtained based on five repetitions of the image, and its average was reported as noise.
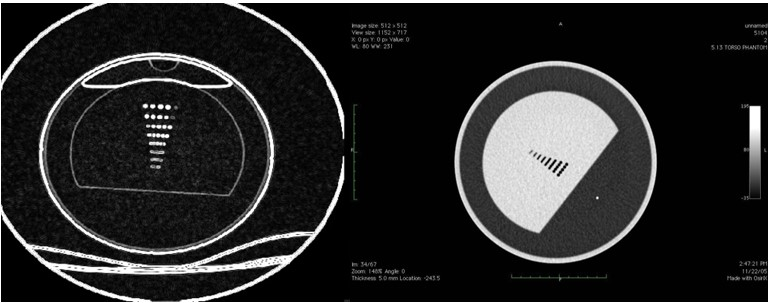
High-Contrast Spatial Resolution
The phantom spatial resolution model (Figure 2) consists of seven rows of cavities with a maximum density difference relative to the background, which reduces the diameter and distance between the holes from top to bottom. The lowest row in which two adjacent holes are observed separately is considered as the spatial resolution. In other words, if a linear array is considered for each row of cavities, and if the signal between two cavities varies a lot, two adjacent cavities can be distinguished separately. Therefore, to find the maximum changes, it is necessary to take a derivative or gradient in the cavities’ direction. Then, for each array, the differential value was calculated, and its standard deviation was obtained. If number achieved for each row is greater than the noise threshold, that row is separable. It is repeated for each row to obtain spatial resolution based on a pair of lines per millimeter.
Channelized Hotelling observers (CHO) model
In this study CHO model was used for low contrast detectability. The observer model used in this study was implemented in the MATLAB program (MATLAB R2015a). In the CHO model, detection is considered as confirmation of one of these two unique hypotheses: H0 (no signal) and H1 (signal). For this purpose, the information of the observed image (g) is given to Equation 1.
Hh:g=hx+ b, h=0,1 (1)
Which, the known signal and background is denoted by x and b, respectively. In addition, the presence or absence of the signal is controlled by the binary variable “h”. Then, a two-dimensional image (test image, signal, or background) is displayed by a vector using vertical concatenation. If the observed image has a M M pixel, its vector version (g) is a M × 1 [20]. It has been proposed to add a channel mechanism to predict human performance by embedding channels in the frequency domain thought to exist in human visual systems [21]. The use of channels involves multiplying images by a series of channel pattern images. In other words, if it is assumed that we have a channel image in total “L , and each channel image is in the form of an M × 1 vector, by applying each channel vector on the image vector, a numerical answer is obtained for example:
$$ V _ {i} = u _ {i} ^ {t} g $$
Which “uii” is the trusted channel and “vi” is the answer “I” the trustworthy channel. Adding channel responses together results in a channel data vector:
V= (v1, v2, v3,…., vL)
The CHO statistical criterion is given by the following equation 2:
$$ \lambda = w _ {C H O} ^ {T} v \tag {2} $$
Which:
$$ w _ {C H O} ^ {T} = S ^ {- 1} \left(\bar {v} _ {1} - \bar {v} _ {0}\right) \tag {3} $$ $$ \text {A n d} \bar {v} _ {1} = U ^ {T} \bar {g} _ {1}, \text {a n d} \bar {v} _ {0} = U ^ {T} \bar {g} _ {0} $$
are the total average of the
channeled vectors are the images of the existing signal and
the missing signal, respectively.
Also, $$ S = \frac {1}{2} \left[ K _ {1} + K _ {0} \right] (4) $$ Which _K_1 and _K_0 are the covariance for the channel images of the existing signal and the missing signal, respectively.
In addition, a figure of merit (fom) can be calculated to describe the CHO detection function. Area under the curve (AUC) is a type of FOM that can be calculated with the sum of the area under the receiver operating characteristic (ROC) diagram. In cases where the AUC is not close to one, the AUC is estimated and then converted to detectability (SNRAUC), which is defined by the following equation 5 [22]:
$$ S N R _ {A U C} = e r f ^ {- 1} (2 A U C - 1) (5) $$
Alternative Forced Choice (2AFC) Study
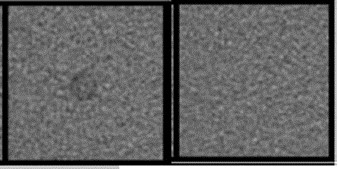
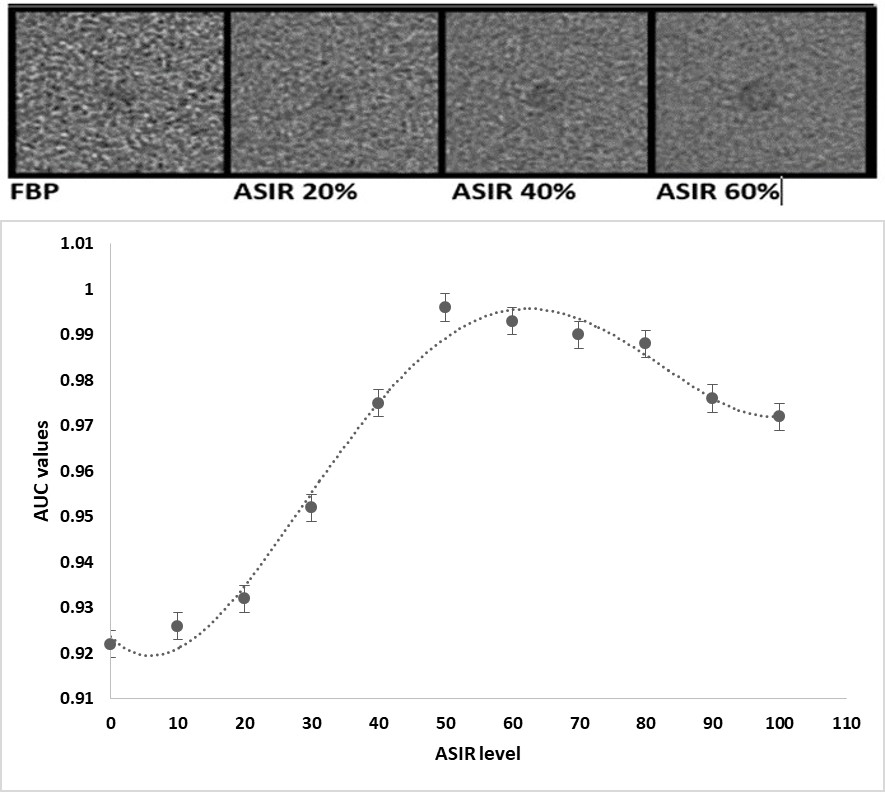
On the images obtained from the phantom, ROIs with a size of 128 x 128 pixels and a FOV size of 6.2 * 2.2 square centimeters were considered. Some of these ROIs were around contrast bars and some were on signalless images. After extracting the ROIs, the obtained images were provided to human observers and the observer model for 2AFC studies. A total of 17 2AFC studies were performed, including 4 studies on FBP (4 mA configuration) and 13 studies on ASIR (4 mA configuration and 10 ASIR reconstruction levels). Each 2AFC study consisted of 80 trials in which one signalless image and one signal image were placed side by side (Figure 3). Human observers and the observer model decided which image had the signal.
In order to evaluate the performance of the CHO model in the 2AFC experiment, we obtain the AUC values in the signal with and without signal by calculating the signal-to-noise ratio or the area under the ROC curve. This value represents the percentage of correct decisions made by the CHO model in the 2AFC experiment.
Human Observer
Three experienced radiologists analyzed all images obtained in this study in a workstation with constant ambient light and image display contrast. The images were randomly provided to observers, and they had no information about the scan parameters associated with each image. Observers could only change the magnification of the images. The images were displayed with a window surface of 40 and a width of 400. Also, observers were asked to rate their confidence in the analysis results for each image using a 6-part scale ( i.e., ranging from 0 to 5; 5 means the highest confidence in the presence of the signal ).
Radiation dose
To demonstrate the average radiation dose that is delivered to the scan volume, the volume CT dose index (CTDIvol) can be utilized express for a particular examination, which a derivative of the CT dose index (mGy). It may be employed as a measure to compare protocols throughout various scanners and practices when associated variables, including the resulting image quality, are taken into consideration as well. CTDIvol has a direct and linear relationship with the tube current, and in many scanners, its value is estimated before the scan begins by specifying the imaging parameters. After each scan, CTDIvol values were extracted from the CT scan machine screen.
Statistical analysis
In this study, SPSS software version 20 was used for statistical analysis. two-way ANOVA was used to investigate the relationship between dose and image quality. To evaluate the relationship between observers, intra class correlation (ICC) was computed. The correlation of the observers’ results and the software was also calculated using the Pearson correlation coefficient.
Results
Radiation dose
CTDI (vol) in low-dose CT imaging for tube currents of 140, 100, and 40 mA was 9.42, 6.28, and 3.14 mGy, respectively. Besides, the CTDI (vol) value in standard dose imaging (200 mA tube current and FBP reconstruction) was 12.56 mGy.
Noise
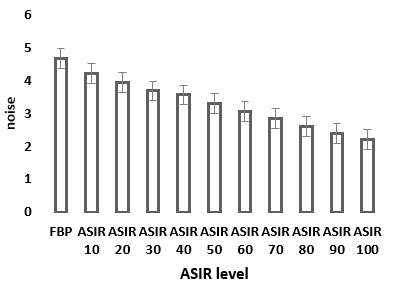
As shown in Figure 4, with increasing ASIR reconstruction level from 0 to 100% under constant radiation conditions (200mA, 100KVp), the amount of continuous image noise is reduced. The noise of reconstructed images with 30% ASIR and higher levels had a significant difference compared to the noise of reconstructed images by the FBP method (P < 0.05). Besides, the mean amount of noise in the images obtained from the phantom with tube currents of 140, 100, and 40 mA reconstructed with 30, 50, and 80% levels of ASIR technique were equal to 4.33 +_ 0.31, which did not have a significant difference with the amount of noise in the images obtained with standard radiation dose and reconstructed by FBP method (4.6) (P > 0.05).
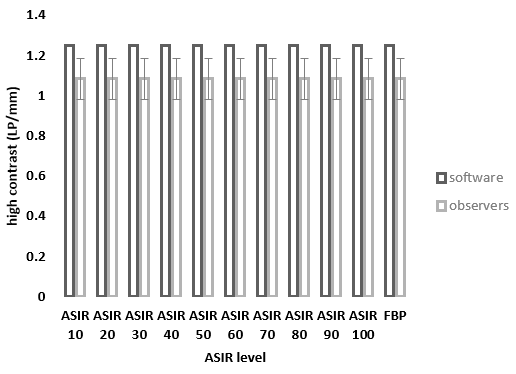
High-Contrast Spatial Resolution
Evaluation of the results reported by observers and ones obtained by the software (Figure 5) showed that with increasing the level of ASIR reconstruction in images obtained with a tube current of 200 mA, the spatial resolution of the images did not change significantly (p> 0.05). Besides, the spatial resolution of the images obtained from the phantom by human observers with tube currents of 140, 100, and 40 mA reconstructed with 30, 50, and 80% levels of ASIR technique was equal to 0.8 ± 0.144 pairs of lines per millimeter, which did not have a significant difference with the amount of the spatial resolution of images obtained with standard radiation dose and reconstructed by FBP method (1 pair of lines per mm) (p> 0.05). The ICC coefficient, which indicates the degree of agreement between the results reported by observers, was 0.801. Also, there was a statistically significant relationship (p = 0.004) and moderate (Pearson correlation coefficient = -0.468) between the values reported by observers and the values obtained by the software.
Evaluation of correlation between model observer and human observer
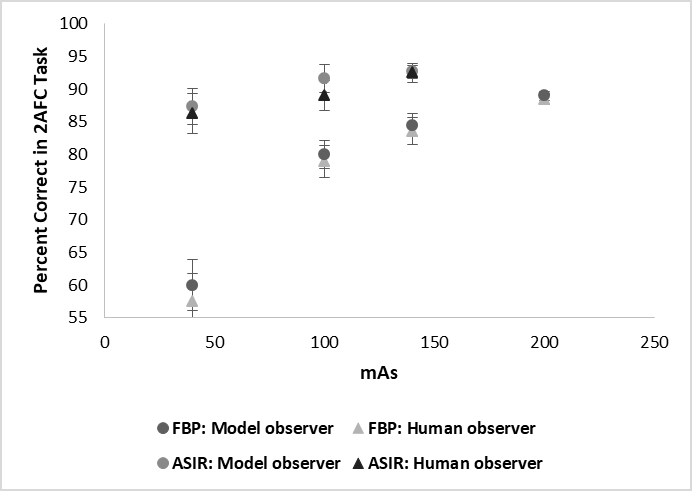
Figure 6 shows a comparison of PC values in the 2AFC test for the human observer and the model observer in the abdomen-pelvic examinations. The results indicate that human and model observations had a high correlation for 4 levels of tube current in pediatric abdomen-pelvic examinations and reconstructed with 30,50, 80% level of ASIR technique. Pearson correlation coefficient for FBP reconstruction in abdomen-pelvic examinations was 0.973, respectively. In addition, PC values obtained from human and models observations at different levels of ASIR reconstruction were highly correlated. Pearson correlation coefficient for ASIR reconstruction in abdomen-pelvic examinations was 0.980, respectively.
Impact of iterative reconstruction on 2AFC Task
From the point of view of human observers, the use of ASIR reconstruction during low-dose imaging of the pediatric abdomen-pelvic improves the amount of percent correct (PC). The amount of PC in 30% reduction of radiation dose (140 mA) from 85.6± 1.7% to 94.65± 1.5% (P = 0.001) and in 50% reduction of radiation dose (100 mA) from 80.94 ±2.5% to 91.15_ + 2.3% (P = 0.021) increased. In fact, using the ASIR technique can increase the ability to detect low-contrast objects at low dose radiation. As in human observers, the PC values improved by the control model from 86.1 ±1.4% to 94.8 ±1% (P = 0.012) in a 30% reduction in radiation dose and 81.96 ±2.8% to 91.66 ±2.1% (P = 0.001) in 50% reduction of radiation dose was reported. In addition, from the point of view of human observers and observer model the amount of PC in 80% reduction of radiation dose (40 mA) was equal to 82.8%±3.4%, which was significantly different with the amount of PC in standard radiation dose (200 mA, FBP) (P>0.05).
Optimization of ASIR technique
Figure 7 shows the AUC values for objects with a contrast of 5HU and a diameter of 3 mm in the FBP reconstruction method and different levels of ASIR reconstruction (from 10% to 100%) for abdomen-pelvic imaging (200mA,100 KVp). Based on curve in abdominal-pelvic imaging, with increasing ASIR reconstruction level from 0 to 50%, the AUC value reaches its maximum (P = 0.003).
Discussion
Previously, CT scanners only used the FBP method to reconstruct images. FBP is a fast reconstruction technique that uses simple mathematical models and limited calculations to reconstruct the image. Although this method is very simple to use and leads to an increase in image reconstruction speed, this simplicity in the reconstruction process causes an excessive increase in image noise at low doses [6]. Unlike the FBP reconstruction method, iterative reconstruction techniques use extensive and complex mathematical models to reconstruct the image and reduce noise. The complexity of the calculations in iterative reconstruction methods has led to a longer reconstruction time than the FBP method [12]. ASIR is one of the iterative reconstruction methods. The ASIR reconstruction method does not assume that the measured signal is noise-free, but more accurate statistical modeling is used to reduce or eliminate noise in the reconstruction process [8]. The present study demonstrated that using the ASIR reconstruction method and combining it with the FBP method can reduce the radiation dose by 50% while maintaining effective quality parameters such as noise, spatial resolution, and contrast resolution. In fact, using the ASIR technique can increase the ability to detect low- contrast objects in the 2afc test by compensating for the noise of images obtained at low radiation doses. Besides, the ASIR technique can be used to reduce noise and optimize image quality.
Extensive studies have been performed on applying the ASIR technique in adult abdominal CT scans [10, 11, 15]. Their results showed that using the ASIR technique could reduce the radiation dose by 31-41% while maintaining image quality. However, although children are more sensitive to radiation than adults, few studies have been conducted on applying the ASIR technique in imaging children [13, 14]. In this study, the ASIR reconstruction technique’s effect on reducing radiation dose and improving image quality in pediatric abdominal and pelvic CT scans was investigated. The present study results showed that the amount of radiation dose in abdominal and pelvic imaging could be reduced by 50% using the ASIR technique. Simultaneously, the parameters affecting the image quality, such as noise, spatial resolution, and contrast resolution, can be maintained as standard. Reducing the radiation dose by 80% and using a 40-mA tube current significantly reduces the quality of the image reconstructed with the ASIR technique. Overall, the results reported in this study were consistent with previous studies on the phantom [22, 23, 24]. In most of these studies, using ASIR 40-50% is recommended. Also, limited clinical studies have been performed by Vorona, et al. [12], Brady, et al. [25], and Sing, et al. [15], who has reported dose reductions of 30-48%. The rate of radiation dose reduction in the present study was greater than in the previous clinical study. In most clinical studies, the use of ASIR 40% and radiation dose reduction of 30-40% is recommended [25, 26]. Differences in the results reported in previous clinical studies with the present study results may be due to differences in study design.
Most studies that have examined the application of the ASIR technique in radiation dose reduction were clinical investigations [25, 26]. These studies were designed in two forms, prospective and retrospective. Prospective studies require additional CT examinations on a patient, and because it is attempted to minimize radiation for children, this will not be ideal. In retrospective clinical studies, two groups with almost the same weight are compared, the ASIR technique will be used for one group, and the FBP method will be used for the other group. Although this type of study increases the sample size, it is assumed that two patients of the same weight have the same body shape and composition. However, there are large differences in body size and shape in growing children at a certain weight [12]. Thus, the present study was performed on a standard phantom with a diameter of 16 cm, which is equivalent to children’s bodies. Although the results of studies on the phantom may be slightly different from the actual effects of the ASIR technique on image quality, it prevents unnecessary radiation to children and, due to the constant dimensions of the phantom, more accurate comparisons can be made.
The present study’s findings showed that although the lowest amount of noise in the image is obtained using the 100% ASIR reconstruction method, but according to the results obtained from the CHO model, it can be said that the use of 50% ASIR in abdomen-pelvic tests improves optimal image quality. In other words, using more than 60% of the ASIR technique leads to smoother borders and reduced visibility of small structures with low contrast. In abdominal and pelvic imaging, optimization of reconstruction methods is of great importance due to the lack of appropriate intrinsic contrast between the lesions and soft tissue.
Clinical evaluations by physicians are the most common method to determine image quality. The use of clinical methods to achieve a reasonable radiation dose and determine image quality is very laborious and requires high accuracy in the design and implementation of the study. The results obtained from clinical evaluations have little capability to compare different imaging and reconstruction protocols in different scanners [27, 28]. Therefore, we need quantitative methods to evaluate the quality of images in CT scan. Modulation transfer function (MTF), Section sensitivity profile (SSP) and NPS are some of the physical methods used to evaluate image quality. These quantitative criteria alone cannot be used in studies because they cannot provide a complete description of the image quality [29, 30]. In addition, some of these physical metrics are not applicable to some imaging protocols. The CHO model observer is one of the image quality assessment methods that has been widely welcomed in studies in recent decades [31, 32]. However, relatively few studies have examined the quality of CT scan images using the CHO model. Wunderlich and Noo used a CHO for modeling the human observer performance in the diagnosis of simulated lesions [33]. Richard et al. investigated the relationship between model observers and the performance of human observers for diagnostic tasks in multislice CT [34]. In their studies, it was assumed that the noise was constant and Gaussian, and computer simulations were used in diagnostic task. In addition, Lifeng Yu et al. investigated how the observer model CHO could predict human observer performance for a simple diagnostic task [33]. In the present study, the CHO model was used to evaluate the image quality. In this study, unlike many previous studies [35, 36], instead of using simulated signals, low-contrast phantom scans were used to produce signal- absent and signal-present images. The results of this study showed that there is a excellent agreement in performance between human observers and CHO model in different dose levels for both FBP and ASIR reconstruction methods and the CHO model has the potential to be used to optimize radiation doses and scan protocols for clinical scenarios. However, placing the signals on a uniform background may simplify the decision to determine the presence of the signal in the image and the results in clinical terms seem a bit unrealistic.
This study faced some limitations. First, in this study, only one iterative reconstruction method was evaluated on a scanner model. Therefore, the results obtained are only applicable to one type of iterative reconstruction. Second, no clinical evaluation was performed to optimize radiation dose and image quality in this study. It was just attempted to do this optimization using phantoms and evaluating physical parameters affecting image quality. However, to achieve more practical radiation dose optimization and image quality results, this study needs to be completed with a clinical evaluation.
Conclusion
Based on results of this study, using of 50% ASIR for the pediatric population can reduce the radiation dose on abdominal and pelvic CT scans by 50% while maintaining image quality. Also, using ASIR 50% only for the reconstruction of abdominal and pelvic images in children leads to optimal image quality. A CHO-based model observer can be used to predict human observer performance at different radiation dose and for both FBP and IR reconstruction methods. CHO model can provide a quantitative approach to efficiently optimizing CT protocol and radiation dose.
Acknowledgment
This study was sponsored by the Student Research Committee of the Paramedical School of Isfahan University of Medical Sciences, Isfahan, Iran, with the approved project number of 197155.
References
-
Collough CHM, Chen GH, Kalender W, Leng S, Samei E, et al. (2012) Achieving Routine Submillisievert CT Scanning a Report From the Summit on The Management of Radiation Dose in CT. Radiology 264(2): 567-580.
-
Patro SN, Chakraborty S, Sheikh A (2016) The Use of Adaptive Statistical Iterative Reconstruction (Asir) Technique in Evaluation of Patients with Cervical Spine Trauma Impact on Radiation Dose Reduction and Image Quality. Br J Radiol 89(1060).
-
Brenner DJ, Hall EJ (2007) Computed Tomography an Increasing Source of Radiation Exposure. N Engl J Med 357(22): 2277-2284.
-
Imhof H, Schibany N, Ba Ssalamah A, Czerny C, Hojreh A, et al. (2003) Spiral CT and Radiation Dose. Eur J Radiol 47(1): 29-37.
-
Lee SH, Kim MJ, Yoon CS, Lee MJ (2012) Radiation Dose Reduction with the Adaptive Statistical Iterative Reconstruction (ASIR) Technique for Chest CT in Children an Intra-Individual Comparison. Eur J Radiol 81(9): 938-943.
-
Fan J, Yue M, Melnyk R (2014) Benefits of ASiR-V reconstruction for reducing patient radiation dose and preserving diagnostic quality in CT exams. White paper GE Healthcare.
-
Maxfield MW, Schuster KM, McGillicuddy EA, Young CJ, Ghita M (2012) Impact of Adaptive Statistical Iterative Reconstruction on Radiation Dose in Evaluation of Trauma Patients. The Journal of Trauma and Acute Care Surgery 73(6): 1406-1411.
-
Shah A, Rees M, Kar E, Bolton K, Lee V, Panigrahy A (2018) Adaptive Statistical Iterative Reconstruction Use for Radiation Dose Reduction in Pediatric Lower- Extremity CT: Impact on Diagnostic Image Quality. Skeletal Radiology 47(6): 785-793.
-
Singh S, Kalra MK, Hsieh J, Licato PE, Do S, et al. (2010) Abdominal CT: Comparison of Adaptive Statistical Iterative and Filtered Back Projection Reconstruction Techniques. Radiology 257(2): 373-383.
-
Myers KJ, Barrett HH (1987) Addition of a Channel Mechanism to the Ideal-Observer Model. JOSA A 4(12): 2447-2457.
-
Park S, Badano A, Gallas BD, Myers KJ (2008) Incorporating Human Contrast Sensitivity in Model Observers for Detection Tasks. IEEE Transactions on Medical Imaging 28(3): 339-347.
-
Vorona GA, Ceschin RC, Clayton BL, Sutcavage T, Tadros SS, et al. (2011) Reducing Abdominal CT Radiation Dose with the Adaptive Statistical Iterative Reconstruction Technique in Children: A Feasibility Study. Pediatric Radiology 41(9): 1174-1182.
-
Mueck FG, Korner M, Scherr MK, Geyer LL (2012) Upgrade to Iterative Image Reconstruction (IR) in Abdominal MDCT Imaging: A Clinical Study for Detailed Parameter Optimization Beyond Vendor Recommendations Using the Adaptive Statistical Iterative Reconstruction Environment (ASIR). Inrofo-Fortschritte Auf Dem Gebiet Der Rontgenstrahlen Und Der Bildgebenden Verfahren 184(3): 299-238.
-
Yoon MA, Kim SH, Lee JM, Woo HS, Lee ES, et al. (2012) Adaptive Statistical Iterative Reconstruction and Veo: Assessment of Image Quality And Diagnostic Performance in CT Colonography at Various Radiation Doses. Journal of Computer Assisted Tomography 36(5): 596-601.
-
Barrett HH, Yao J, Rolland JP, Myers KJ (1993) Model Observers for Assessment of Image Quality. Proceedings of the National Academy of Sciences 90(21): 9758-9765.
-
International Commission on Radiation Units and Measurements “Medical imaging - The assessment of image quality,” ICRU Report 1995: No. 54.
-
Yu L, Leng S, Chen L, Kofler JM, Carter RE, et al. (2013) Prediction of Human Observer Performance in A 2‐ Alternative Forced Choice Low‐Contrast Detection Task Using Channelized Hotelling Observer: Impact of Radiation Dose and Reconstruction Algorithms. Medical Physics 40(4): 041908.
-
Gang GJ, Tward DJ, Lee J, Siewerdsen JH (2010) Anatomical Background and Generalized Detectability in Tomosynthesis and Cone‐Beam CT. Medical Physics 37(5): 1948-1965.
-
Gifford HC, King MA, de Vries DJ, Soares EJ (2000) Channelized Hotelling and Human Observer Correlation for Lesion Detection in Hepatic SPECT Imaging. Journal of Nuclear Medicine 41(3): 514-521.
-
Mieville FA, Ayestaran P, Argaud C, Rizzo E, Ou P, et al. (2010) Potential Benefit of the CT Adaptive Statistical Iterative Reconstruction Method for Pediatric Cardiac Diagnosis. In Medical Imaging 2010: Physics of Medical Imaging Vol. 7622. International Society for Optics and Photonics.
-
Mitsumori LM, Shuman WP, Busey JM, Kolokythas O, Koprowicz KM (2012) Adaptive Statistical Iterative Reconstruction Versus Filtered Back Projection in the Same Patient: 64 Channel Liver CT Image Quality and Patient Radiation Dose. European radiology 22(1): 138- 143.
-
Lee SH, Kim MJ, Yoon CS, Lee MJ (2012) Radiation Dose Reduction with the Adaptive Statistical Iterative Reconstruction (ASIR) Technique for Chest CT in Children: An Intra-Individual Comparison. European Journal of Radiology 81(9): e938-e943.
-
Singh S, Kalra MK, Shenoy Bhangle AS, Saini A, Gervais DA, et al. (2012) Radiation Dose Reduction with Hybrid Iterative Reconstruction for Pediatric CT. Radiology 263(2): 537-546.
-
Hara AK, Paden RG, Silva AC, Kujak JL, Lawder HJ, et al. (2009) Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. American Journal of Roentgenology 193(3): 764-771.
-
Zarb F, Rainford L, McEntee MF (2011) Developing Optimized CT Scan Protocols: Phantom Measurements of Image Quality. Radiography 17(2): 109-114.
-
Gay F, Pavia Y, Pierrat N, Lasalle S, Neuenschwander S, et al. (2014) Dose Reduction with Adaptive Statistical Iterative Reconstruction for Paediatric CT: Phantom Study and Clinical Experience on Chest and Abdomen CT. European radiology 24(1): 102-111.
-
Brady SL, Yee BS, Kaufman RA (2012) Characterization of Adaptive Statistical Iterative Reconstruction Algorithm for Dose Reduction in CT: A Pediatric Oncology Perspective. Medical Physics 39(9): 5520-5531.
-
Bae S, Kim MJ, Yoon CS, Kim DW, Hong JH, et al. (2014) Effects of Adaptive Statistical Iterative Reconstruction on Radiation Dose Reduction and Diagnostic Accuracy of Pediatric Abdominal CT. Pediatric radiology 44(12): 1541-1547.
-
Singh S, Kalra MK, Moore MA, Shailam R, Liu B, et al. (2009) Dose Reduction and Compliance with Pediatric CT Protocols Adapted to Patient Size, Clinical Indication and Number of Prior Studies. Radiology 252(1): 200- 208.
-
Guimaraes LS, Fletcher JG, Harmsen WS, Yu L, Siddiki H, et al. (2010) Appropriate Patient Selection at Abdominal Dual-Energy CT Using 80 kV: Relationship Between Patient Size, Image Noise and Image Quality. Radiology 257(3): 732-742.
-
Kazerooni EA, Armstrong MR, Amorosa JK, Hernandez D, Liebscher LA, et al. (2015) ACR CT Accreditation Program and the Lung Cancer Screening Program Designation. Journal of the American College of Radiology 12(1): 38- 42.
-
Siewerdsen JH, Cunningham IA, Jaffray DA (2002) A framework for noise‐power spectrum analysis of multidimensional images. Medical physics 29(11): 2655-2671.
-
Burgess AE, Jacobson FL, Judy PF (2001) Human Observer Detection Experiments with Mammograms and Power‐Law Noise. Medical Physics 28(4): 419-437.
-
Tisdall MD, Atkins MS (2006) Using Human and Model Performance to Compare MRI Reconstructions. IEEE Transactions on Medical Imaging 25(11): 1510-1517.
-
Wunderlich A, Noo F (2008) Image Covariance and Lesion Detectability in Direct Fan-Beam X-Ray Computed Tomography. Physics in Medicine & Biology 53(10): 2471-2493.
-
Richard S, Li X, Yadava G, Samei E (2011) Predictive Models for Observer Performance in CT: Applications in Protocol Optimization. Physics of Medical Imaging 7961: 79610H.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage