Multiphasic MDCT of Living Renal Donors, Prior to Surgery
Background: Live kidney donor evaluation mandates anatomical and functional assessment of the donor kidney. Multiphasic Multidetector computed tomography (MDCT) with advanced 3‐D techniques provides a detailed description of the vascular, parenchymal, and collecting system. Objectives: To evaluate the clinical application of Multiphasic MDCT in the pre-operative anatomic assessment of prospective donor kidneys. Methods: Multiphasic MDCT was performed in thirty-eight patients as part of a pre-operative assessment. Each study comprised three phases of imaging, including the arterial, venous, and excretory phases. Results: The predominant radiological finding amongst the cases studied was that of the presence of accessory renal arteries in 35% of the patients. Multiphasic MDT was also able to detect renal parenchymal disease in one case. Post-renal anatomical evaluation also identified renal calculi in 12.5% of the total cases. Conclusions: There is considerable scope for multiphasic MDCT in the pre-operative evaluation of donor kidneys, especially as modern-day renal transplant surgery sees a shift towards laparoscopic techniques where intraoperative anatomic evaluation can be restricted. The multiphasic MDCT is useful in pre-renal, renal, and post-renal anatomic evaluation. Advances in Knowledge: Multiphasic MDCT can provide noninvasive, detailed, and fast images to aid the preoperative evaluation of donor kidneys.
Introduction
Kidney transplantation (KT) is the treatment of choice in patients with end-stage renal disease, as it improves patient survival and recipients’ quality of life compared to chronic dialysis treatment [1]. A staggering number of more than 50,000 patients were noted to be awaiting a kidney transplant in the United States in October 2001, but only approximately 9,000 cadaver kidney transplants had been performed each year over the preceding decade [2].
An anatomic assessment of the donor’s kidney is performed before transplantation to aid in the selection of which kidney to use and to plan the surgical approach. The increasing use of laparoscopic donor nephrectomy makes preoperative diagnosis even more critical since the details of arterial and venous anatomy especially visualizing of the posterior and medial superior aspects of the kidneys and renal vessels are limited during a laparoscopic surgery [3]. A renal donor must have two kidneys of normal size and position. Renal vessels are acknowledged for presenting a wide range of variations. About 70% of people have 1 renal artery per kidney, typically arising at the level of the upper margin of the second lumbar vertebral body, 1 cm below the origin of the superior mesenteric artery. It is important to detect any perihilar branching that occurs within 2 cm of the origin of the renal artery from the aorta, as most surgeons require at least a 2 cm length of renal artery before hilar branching, to ensure adequate control and anastomosis [2].
The venous anatomy includes renal veins, adrenal veins, gonadal veins, and lumbar veins. Renal veins have a more uniform anatomic pattern than renal arteries, and 92% of people have one renal vein on each side. The left renal vein is approximately 7.5 cm long, and the right renal vein is approximately 2.5 cm long. Duplicate renal veins are more common on the right side. Duplicate collecting systems are found in approximately 1% of the general population [2]. Although criteria for the exclusion of laparoscopic donor nephrectomy have not been clearly defined, the presence of a renal anomaly such as unilateral agenesis, renal ectopia, or horseshoe kidney is a contraindication for the procedure. Other exclusionary criteria are the presence of renal arterial disease, renal neoplasm, severe hydronephrosis, cortical atrophy, sponge kidney, renal papillary necrosis, or retroperitoneal varices [2].
Nephrolithiasis may be a contraindication for living donor nephrectomy because of the risk that recurrent stones, obstruction, and infection may injure the remaining kidney. This condition also places the recipient at risk. Preoperative diagnostic imaging plays a fundamental role in the evaluation of kidneys and vasculature, initiating a minimized risk of complications in both the recipient and the donor [4]. Preoperative diagnostic imaging modalities include Doppler ultrasound, multiphase computed tomography (CT) including CT Angiography (CTA), and magnetic resonance imaging (MRI) or angiography (MRA) [4]. Ultrasound is cheap and widely available but fails to assess vessel anatomy, whereas MRA can provide a detailed evaluation of the kidneys and can be used for patients with an iodine allergy. The limitations of MRA are spatial resolution and small coverage per slab in a single acquisition, which potentially may result in missing the small accessory arteries arising from pelvic vessels. Other potential issues with MRI are motion artifacts due to breathing in longer sequences and poor coordination between the injection of the contrast material and image acquisition. Further, small stones and calcifications can easily be missed on MRI images, possibly necessitating additional imaging. Compared to Ultrasound and MR, CT exposes the patient to ionizing radiation and a potential risk of contrast-induced nephrotoxicity or allergy [4].
CT angiography is less invasive, better tolerated by patients, and provides considerably more information than other modalities, particularly concerning renal vascular anatomy and non-renal intraabdominal organs [5]. The better spatial resolution, faster speed, and greater cost- effectiveness of CT have led to a wide acceptance of CT over other modalities [6]. Previous works have shown that CT angiography has 100 % sensitivity in identifying accessory arteries and 93 % sensitivity in identifying perihilar arterial branches [7], According to a study 3.0T MRI excellent depiction of renal hilar anatomy as well as early arterial branching with a sensitivity of 96% and a PPV of 100%, and a lower sensitivity (72%) and accuracy (83%) in the detection of late venous confluence [8].
The technical parameters for the MDCT protocol depend on the speed of the scanner, the section thickness, and the number of phases—in the majority of institutions, the study comprises a multiple-phase procedure including at least two of the following phases: unenhanced, arterial, nephrographic and excretory phase [7]. The CT protocol parameters depend on the speed of the scanner, the section thickness options, the number of scanning phases (scanning timing relative to the administration of contrast medium), and the anatomic coverage of each scan [9]. The optimal delay for each imaging phase after contrast material injection depends on the volume of contrast material administered, the rate of injection, and the subject’s cardiac output. The main aim of the unenhanced phase is to locate the kidneys, rule out calculi, and provide a baseline study to compare the enhancement of eventual lesions [2].
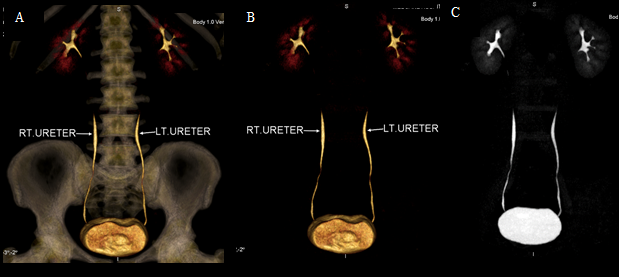
While the arterial phase is used to depict not only the arterial anatomy but also venous anatomy. The venous enhancement is different from the arterial enhancement. The nephrogenic phase depicts the veins, except for small tributaries such as gonadal, adrenal, and lumbar veins which tend to opacify to the same degree as arteries, making characterization of vascular anatomy difficult. Finally, an excretory phase 7–10 min after contrast injection is used to assess the renal collecting system and ureters [10].
Scan Protocol
MDCT was performed using 64-slice MDCT with 0.5 tube rotation time and auto mAs exposure (Aquilion Toshiba). Non-enhanced, arterial, venous, and excretory phases were acquired. Intravenous contrast protocol was 70-80 ml of Iohexol (Omnipaque 350 mg I/ml GE healthcare) injected through the antecubital vein with a 20 gauge intravenous cannula by using an automatic dual syringe power injector (Nemoto technologies) at the rate of 4ml/s followed by a saline chaser. Arterial phase scanning was initiated by bolus tracking when the threshold enhancement of 150 HU was reached at the abdominal aorta 3- 4 cm above the kidneys. Venous phase imaging was initiated 15 seconds after the completion of arterial phase scanning. The excretory phase was initiated with a delay of 8-10 minutes.
Image Analysis
All image datasets were transferred to a stand-alone workstation for post-processing (Vitrea 2.0) and evaluation. A radiologist independently evaluated all the phases.
Results
In our study of 38 cases of pre-renal donor renal angiography, there were 21 (52.5%) male donors and 17 (47.5%) female donors. Amongst the 38 patients, 14 (35.0%) donors had accessory renal artery; 9 donors (22.5%) had right accessory renal artery, 3 (7.9%) donors had left accessory renal artery, and 2 donors (5.0%) had bilateral accessory renal arteries. 4 (10.0%) donors had double right veins and 1 (2.5%) donor had double ureter. 27 donors (67.5%) had satisfactory pre-renal donor appearance. A total of 5 (12.50%) donors had renal calculi; out of which 3 (7.5%) donors had right renal calculi and 2 (5.0%) donors had bilateral multiple renal calculi. Fatty liver, liver hemangioma, and fibroids were incidentally found in 2 donors (5.0%) each. Liver cirrhosis, renal artery stenosis, and ovarian tumor were also incidentally found in 1 (2.5%) donor each. While bilateral renal patchy scaring was found in 1 (2.5%) donor suggestive of previous renal infection.
Conclusion
CT renal donor protocol is a noninvasive technique that is better tolerated by patients and provides considerably more information to demonstrate any abnormality or anomaly prior to the evaluation of living renal donors, particularly concerning renal vascular anatomy and non- renal intraabdominal organs by applying various phases of CT scan. Multiphasic CT angiography has 100 % sensitivity in identifying accessory arteries and 93 % sensitivity in identifying perihilar arterial branches, and renal calculi. Overall, Multiphasic CT angiography allows the radiologists to relay the precise preoperative anatomy of the renal structure & vasculature to the surgical team, thus reducing the risks and complications associated with the harvesting procedure and improving the chances for a successful outcome.
The sensitivity and specificity of ultrasound in detecting renal calculi is significantly lower than unenhanced CT. Unenhanced CT provides an accurate measurement of the calculi, while also differentiating between calcification and calculi as shown in Figure 1. The scan time for MRA as compared to CTA is high, and due to low spatial resolution and small coverage can result in missing the small accessory arteries arising from pelvic vessels. The better spatial resolution, faster speed and using Surestart bolus tracking minimize the chances of missing any small tributaries in CTA as depicted in Figures 2-4.
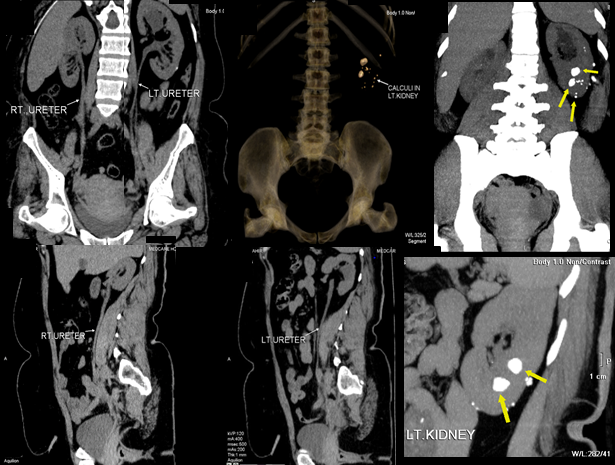
Figure 1: Unenhanced phase showing two non-obstructing calculi in the mid and lower pole of the left kidney measuring up to 13 x 10 mm in the lower pole and 14 x 8 mm in the mid pole with a mean Hounsfield value measured up to 1000.3 in the mid pole and 1360.71 in the lower pole, There are areas of further dense cortical nodular calcification in the left kidney. (A) coronal curved MPR shows right and left ureter (B) 3D semitransparent image (C) coronal MIP image shows size and location of calculi (D) sagittal curved MPR showing the right ureter (E) sagittal curved MPR shows the left ureter (F) shows sagittal MIP image (E) sagittal of the left kidney with increased MIP.
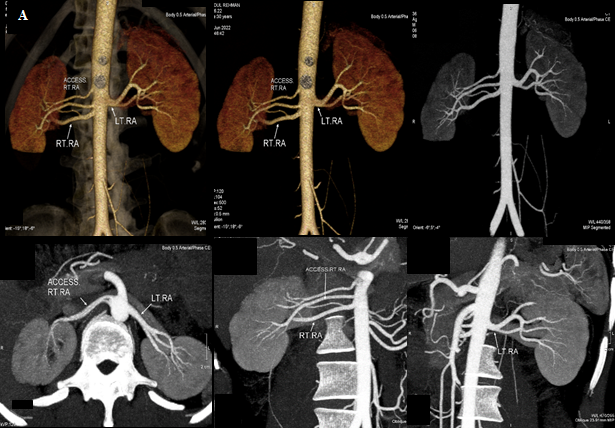
Figure 2: Arterial phase depicting the arterial anatomy; three right renal arteries, two accessory renal arteries coursing towards the right upper renal pole; the main right renal artery measuring approximately 4.5 mm, with an arterial diameter at the origin site of 12mm, and one left renal artery that measures about 5.5mm, with an arterial diameter of 10mm, from their origin till their first segmentary bifurcation. (A) 3D semi-transparent background images (B) 3D transparent background images (C) coronal MIP images (D) curved MPR showing both the right accessory artery and left renal artery on axial (E) oblique coronal showing right renal artery as well as the accessory renal artery (F) showing the left renal artery.
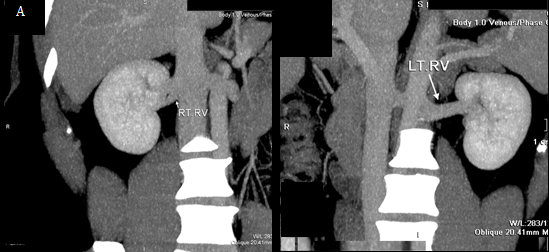
Figure 3: Venous phase depicting the veins, the main left renal vein courses anterior to the aorta measuring about 25 mm from IVC to hilum. The distance between the confluence of the left renal vein and the left margin of the aorta is 40 mm and a single right vein at the renal hilum drains into the IVC which measures 62 mm from the IVC to the hilum. The left gonadal and lumbar veins drain into the left renal vein. The right gonadal and lumbar veins drain directly into the IVC. (A) Showing an oblique of the right renal vein (B) showing the oblique of the left renal vein.
References
-
Bejic M, Deglise S, Venetz JP, Nseir G, Dubuis C, et al. (2018) Use of intraoperative duplex ultrasound and resistance index reduces complications in living renal donor transplantation. Transplant Proc 50(10): 3192- 3198.
-
Kawamoto S, Montgomery RA, Lawler LP, Horton KM, Fishman EK (2004) Multi-detector row CT evaluation of living renal donors prior to laparoscopic nephrectomy. Radiographics 24(2): 453-466.
-
Halpern EJ, Mitchell DG, Wechsler RJ, Outwater EK, Moritz MJ, et al. (2000) Preoperative evaluation of living renal donors: comparison of CT angiography and MR angiography. Radiology 216(2): 434-439.
-
Aghayev A, Gupta S, Dabiri BE, Steigner ML (2019) Vascular imaging in renal donors. Cardiovasc Diagn Ther 9(Suppl 1): S116-S130.
-
Pozniak MA, Balison DJ, Lee FT, Tambeaux RH, Uehling DT, et al. (1998) CT angiography of potential renal transplant donors. Radiographics 18(3): 565-587.
-
Singh AK, Sahani DV (2008) Imaging of the renal donor and transplant recipient. Radiol Clin North Am 46(1): 79-93.
-
Arevalo PJ, Gragera TF, Marin TA, Koren FL, Hayoun C, et al. (2013) Angio CT assessment of anatomical variants in renal vasculature: its importance in the living donor. Insights Imaging 4(2): 199-211.
-
Gulati M, Dermendjian H, Gomez AM, Tan N, Margolis DJ, et al. (2016) 3.0Tesla magnetic resonance angiography (MRA) for comprehensive renal evaluation of living renal donors: pilot study with computerized tomography angiography (CTA) comparison. Clin Imaging 40(3): 370-377.
-
Rydberg J, Kopecky KK, Tann M, Persohn SA, Leapman SB, et al. (2001) Evaluation of prospective living renal donors for laparoscopic nephrectomy with multisection CT: the marriage of minimally invasive imaging with minimally invasive surgery. Radiographics 21 Spec No: S223-S236.
-
Sebastia C, Peri L, Salvador R, Bunesch L, Revuelta I, et al. (2010) Multidetector CT of living renal donors: lessons learned from surgeons. Radiographics 30(7): 1875- 1890.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage