A Rare Combination of Multisystem Congenital Anomalies; Interrupted Aortic Arch, Congenital Cystic Adenomatoid Malformation of the Lungs and Horseshoe Kidneys, A Case Report
Combinations of multisystem congenital anomalies have been frequently reported. However, this article presents a rare combination of congenital anomalies affecting the cardiovascular system, lungs, and kidneys in a neonate, which was detected through a computed tomography exam. The authors conducted a comprehensive search of the English literature and found no previous reports of such a combination in online literature.
Introduction
Congenital anomalies (CAs) are defined as structural or functional abnormalities present at birth [1]. These anomalies can affect a single organ or system, or they may involve multiple organs or systems. One well-known combination of multisystem congenital anomalies is the VATER Association, which includes a combination of three or more defects involving the vertebrae, anorectal area, tracheoesophageal fistula, and renal system [2]. In this article, the authors present a rare combination of congenital anomalies that does not fall under the VATER Association and has not been previously reported in English online literature.
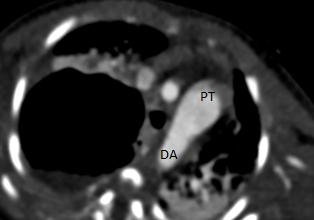
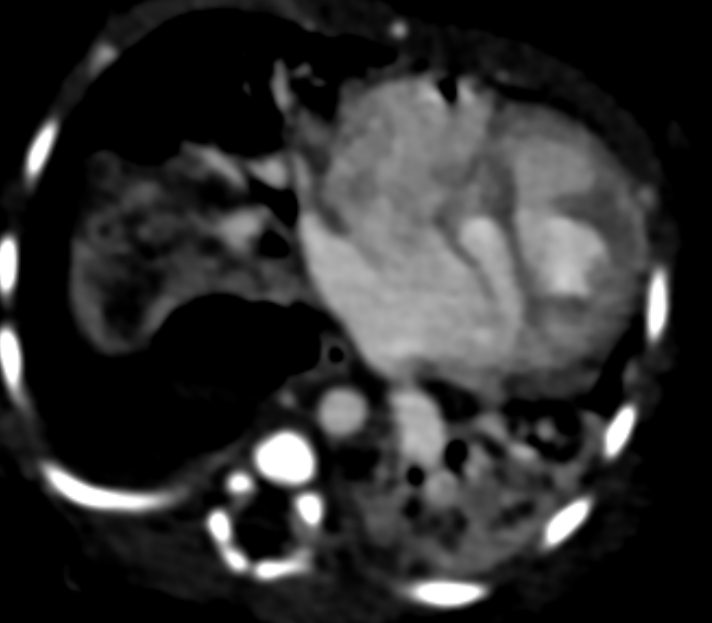
A 7-day-old neonate presenting symptoms of congestive heart failure was referred to the radiology department for a chest computed tomography (CT) scan to assess potential congenital cardiovascular anomalies. The patient underwent a contrast-enhanced computed tomography (CECT) scan using a 128-slice Siemens CT scanner. The obtained images revealed an interrupted aortic arch (IAA) located distal to the origin of the left subclavian artery, classified as type A (Figure 1). The descending aorta was visualized continued to a large patent ductus arteriosus (PDA) originating from the dilated pulmonary trunk (Figure 2). Additionally, a ventricular septal defect was identified (Figure 3).
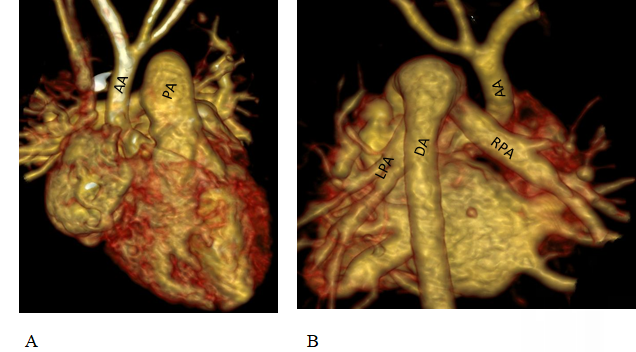
Figure 1: Cardiac CT, VRT reconstructed images; (A-anterior view): Aorta (AA) arising from left ventricle with normal branching of aortic arch. Interruption of aorta is noted distal to the origin of left subclavian artery. Pulmonary artery (PA) appears dilated. (B-posterior view): Descending aorta (DA) is opacified via large patent ductus arteriosus (PDA) from the pulmonary trunk. Right and left pulmonary arteries are also seen in this view (RPA and LPA).

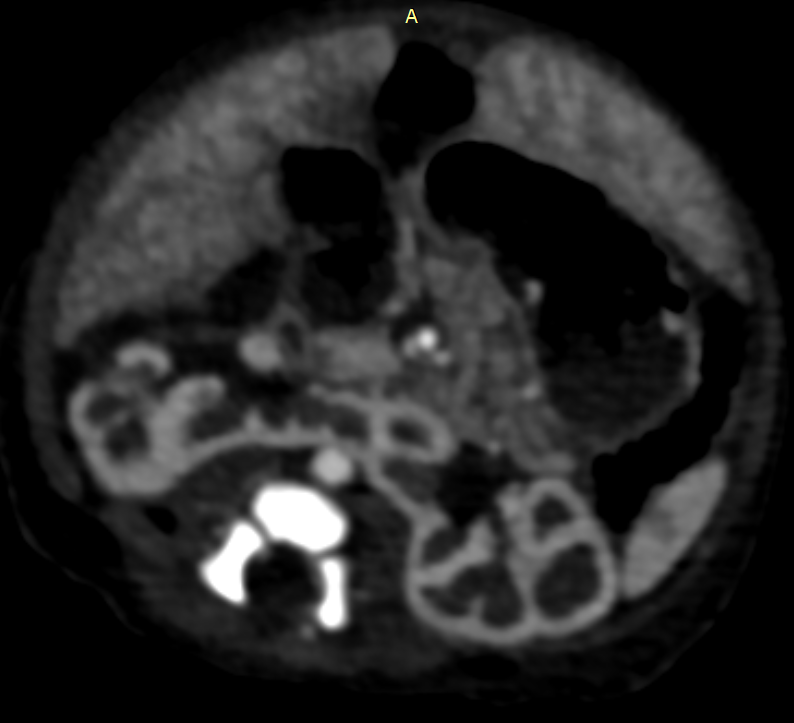
In the lung window, a sizable multi-loculated cystic lesion was observed in the upper lobe of the right lung. The cysts predominantly measured less than 2 cm in size, with no dominant cyst evident. The imaging also revealed a mediastinal shift toward the left side. This condition was diagnosed as congenital cystic adenomatoid malformation (CCAM) type 2 (Figure 4). Sections obtained from the upper abdomen displayed the fusion of the lower poles of the kidneys anterior to the abdominal aorta, consistent with a horseshoe kidney (Figure 5).
Discussion
Interrupted aortic arch (IAA) is a rare congenital anomaly that occurs in approximately 2 cases per 100,000 live births and is often associated with other intracardiac and/or extracardiac anomalies [3, 4]. IAA is classified into three types (A, B, and C) based on the location of the interruption [5]. This classification was originally described by Celoria GC, et al. [6] in 1959. Type A refers to interruption distal to the left subclavian artery, type B (the most common) refers to interruption between the left common carotid and left subclavian artery, and type C (the rarest) refers to interruption between the innominate and left carotid arteries. In a multi-institutional study of 472 patients with IAA conducted by the Congenital Heart Surgeons’ Society (CHSS) and reported by Mccrindle BW, et al. [7] type A was observed in 28% of patients, type B in 70%, and type C in 1%. In our case, the aortic arch is interrupted distal to the origin of the left subclavian artery, which is consistent with type A aortic arch.
Congenital cystic adenomatoid malformation (CCAM) is a rare congenital anomaly that affects the terminal respiratory structures [8]. Patients with CCAM can present as neonates with severe, progressive respiratory distress due to cyst expansions [9]. Stocker and colleagues described three types of CCAM based on gross and microscopic features. Type I, known as the large-cyst type, is characterized by one or more cysts ranging from 2 to 10 cm in diameter. These cysts are surrounded by multiple smaller cysts. The affected area appears as an enlarged lobe or portion of a lobe, which may be distorted due to the varying sizes of the cysts at different stages of expansion. The walls of the cysts may appear thick due to adjacent collapsed lung tissue or collapsed cysts. The cysts themselves can contain air, fluid, or a combination of both.
Type II corresponds to the intermediate cyst type, which consists of simpler cysts that rarely exceed 2 cm in diameter. These lesions comprise multiple uniform cysts that do not exceed 2 cm in size. The cyst-containing areas of the lesion merge with the surrounding normal lung tissue.
Type III, known as the small-cyst type, is a large and bulky lesion primarily observed in newborn or stillborn male infants associated with significant polyhydramnios during gestation. This lesion typically affects an entire lobe or occasionally the entire lung. The cysts in type III lesions are infrequent and do not exceed 0.3-0.5 cm in diameter. They are randomly distributed throughout the lesion and have a solid appearance, representing epithelial-lined alveolar-like structures separated by dilated bronchiole-like structures [10]. In our reported case, there is a large multicystic lesion replacing a portion of a lobe, which represents a type I CCAM.
Horseshoe kidney is the most common renal fusion anomaly and is characterized by a combination of three anatomical abnormalities: ectopia, malrotation, and vascular changes. According to the authors’ search of the English literature on Google Scholar, no such combination has been reported in English literature until February 2024.
Take Home Message
When investigating a congenital anomaly within a specific system, it is important to exercise caution and consider the possibility of anomalies in other organs and systems as well.
Declarations
Ethics Approval and Consent to Participate: The manuscript has received ethical review exemption from the ethical review committee of the authors’ institution, as case reports are exempted from review according to the institutional ethical review committee’s policy. Written consent has been obtained from the participants for publishing the case. Consent to Publish: Written consent has been obtained from the participants for publishing the case. Availability of Data and Materials: The data will be made available to the journal editor upon request. Competing Interests: None of the authors have any competing interests. Funding: This study did not receive any funding in any form. Authors Contributions: The authors have contributed equally to the submission and take public responsibility for its content. HH: Selecting the case and radiologic images, supervising the writing process of the manuscript. AZ: Writing the manuscript.
References
-
Rosano A, Botto L, Botting B, Mastroiacovo P (2000) Infant mortality and congenital anomalies from 1950 to 1994: an international perspective. J Epidemiol Community Health 54(9): 660-666.
-
Botto LD, Khoury MJ, Mastroiacovo P, Castilla EE, Moore CA, et al. (1997) The spectrum of congenital anomalies of the VATER association: an international study. Am J Med Genet 71(1): 8-15.
-
Lapar DJ, Baird CW (2018) Surgical considerations in interrupted aortic arch. Semin Cardiothorac Vasc Anesth 22(3): 278-284.
-
Alcantara JR, Mendez MD (2023) Interrupted Aortic Arch. StatPearls, Treasure Island, Florida, United States of America.
-
Reardon MJ, Hallman GL, Cooley DA (1984) Interrupted aortic arch: brief review and summary of an eighteen- year experience. Tex Heart Inst J 11(3): 250-259.
-
Celoria GC, Patton RB (1959) Congenital absence of the aortic arch. Am Heart J 58: 407-413.
-
Mccrindle BW, Tchervenkov CI, Konstantinov IE, William GW, Rodolfo AN, et al. (2005) Risk factors associated with mortality and interventions in 472 neonates with interruption of the aortic arch: A Congenital Heart Surgeons Society study. J Thorac Cardiovasc Surg 129(2): 343-350.
-
Zeng Z, Liu C, Liu C, Pu Q, Mei J, et al. (2022) Clinical characteristics and surgical treatment of congenital cystic adenomatoid malformation in adults: the largest cohort of 46 patients. Ann Transl Med 10(10): 596.
-
Chan IC, Lee YS, Tsao PC, Jeng MJ, Soong WJ (2013) Congenital pulmonary airway malformation type 4: a case report. J Pediatr Resp Dis 9: 48-52.
-
Rosado CML, Stocker JT (1991) Congenital cystic adenomatoid malformation. Radiographics 11(5): 865- 886.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage