Localized Pachymeningitis - An Uncommon Complication of Chronic Otitis Media and Mastoiditis
We describe the case history of a 55-year-old male presenting with gradual onset of bilateral facial nerve paralysis. A radiological test of CT temporal bone revealed soft tissue thickening in bilateral mastoid air cells and middle ear cavities. Tl weighted contrast-enhanced MRI revealed thickening and early enhancement of the adjacent dura, indicating active pachymeningitis. The past middle ear infection appears to cause the above inflammatory findings in the meninges and worsening on the untreated side. Currently, he is on steroids with some improvement in facial nerve paralysis.
Introduction
Hypertrophic pachymeningitis is a neuro-inflammatory condition characterized by the thickening and fibrosis of the dura mater, leading to the compression of the neural foramen [1]. The present report describes a partially treated case of a bilateral middle ear infection presenting with hypertrophic pachymeningitis.
Case Report
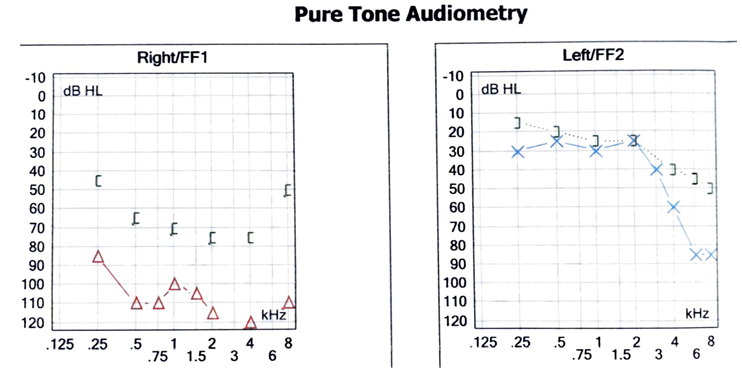
A 55-year-old patient of bilateral chronic suppurative otitis media complained of persistent ear ache, hearing loss and right ear discharge. He had a past history of mastoidectomy of the right ear. On the examination, he showed features of bilateral conductive deafness and bilateral facial nerve palsy (lower motor neuron). Computed tomography of the temporal bone and contrast-enhanced magnetic resonance imaging were advised.
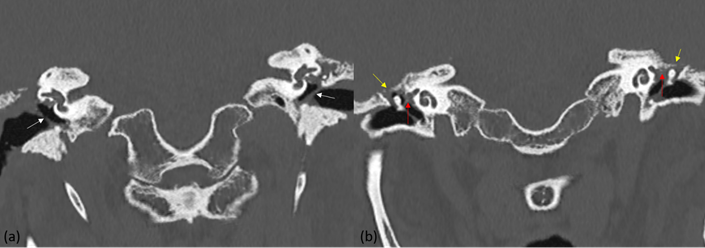
The CT scan revealed evidence of right sided mastoidectomy with opacification of the middle ear cleft and accumulation of fluid in the mastoidectomy site. There was periosteal reaction in the adjoining bony margins which was suggestive of associated osteomyelitis. Both tympanic membranes were thickened and retracted. The tegmen tympani were eroded.
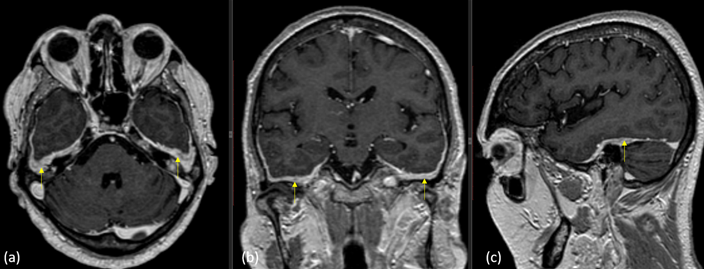
Given the associated facial nerve involvement, contrast- enhanced magnetic resonance imaging was performed which revealed symmetrical thickening and enhancement of the dura within the middle cranial fossa adjacent to the temporal lobes. This finding was consistent with hypertrophic pachymeningitis. The internal auditory canal protocol evaluated the facial and vestibulocochlear nerve, which appeared normal. At the brainstem level, the facial nerve nucleus also revealed no significant finding.
Discussion
Hypertrophic pachymeningitis (HP) is characterized by the thickening and fibrosis of the dura mater. It can result in diffuse or localized thickening in the form of dural plaques that mimic a mass lesion. Various infectious (syphilis, tuberculosis, etc.) or inflammatory (sarcoidosis, granulomatosis with polyangiitis, IgG4-related disease, idiopathic) causes are seen in its background [2]. It is classified as primary or idiopathic and secondary hypertrophic pachymeningitis. Causes of secondary hypertrophic pachymeningitis include infections, dural malignant tumors, metastasis, Wegener’s granulomatosis, rheumatoid arthritis, sarcoidosis, and masked mastoiditis (Figures 1-3).
HP exhibits a diverse clinical presentation depending on the underlying cause. Initial symptoms are commonly headache (seen in up to 92% of patients) and cranial nerve complications. Idiopathic HP is often diagnosed by excluding alternate causes of pachymeningitis, and confirmed by a negative biopsy [3]. Cranial nerves II and VII are affected, often due to nerve compression or orbital pseudotumor, with the optic nerve involved frequently, sometimes bilaterally. The involvement of cranial nerves III, IV, and VI can cause diplopia and painful eye movements. Other neurological manifestations encompass intracranial hypertension, seizures, cerebral venous thrombosis, hearing loss, and gait ataxia. HP shows a variable clinical presentation depending on the location of the lesion and dural thickness on imaging. The parenchymal manifestations of HP include seizures, hemiparesis, tremors, cognitive impairment, and localized brain edema with a “pseudo tumor” presentation [4]. HP can rarely cause spinal cord compression.
IgG4-RD is a systemic fibro inflammatory condition capable of affecting various organs, with the lacrimal and salivary glands, pancreas, biliary tree, and the retroperitoneal space being most commonly affected [5, 6, 7]. In cases of HP previously considered idiopathic, a substantial portion can be attributed to IgG4-related disease and MPO-ANCA- associated vasculitis localized to the central nervous system. The definite diagnosis, however, requires a biopsy and a histological examination. Interestingly, these cases often lack systemic involvement in their clinical presentation, but analyses reveal elevated levels of IgG4 and MPO-ANCA [8].
The meningovascular form of syphilis may also manifest as HP. To exclude this particular presentation of syphilis, serologic evaluation is crucial [2]. In complicated cases of bacterial meningitis or otitis media, the meninges can get involved, leading to HP in the dura adjacent to the infected site. A previous report also showed the development of hypertrophic pachymeningitis secondary to otitis media. It seems that the chronic inflammatory process can lead to changes in the adjacent meninges with can eventually become diffuse [9]. HP and leptomeningitis are both linked to tuberculosis, typically presenting alongside cognitive behavioral disorders and systemic symptoms. While conventional CSF analysis can aid the diagnosis, advanced techniques like PCR are much more sensitive [10]. Fungal meningitis causes dural thickening with features akin to those seen in other causes of HP, with Aspergillus Flavus being a prominently associated pathogen [11].
Anti-neutrophil cytoplasmic antibody (ANCA)- associated vasculitis (AAV) is a rare necrotizing vasculitis. It has few or no immune deposits and primarily involves small vessels associated with ANCA specific for myeloperoxidase (MPO) or proteinase 3 (PR3). AAV of the small vessels includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA). AAV has also been demonstrated to cause HP [12]. Older male diabetic or immunocompromised patients can develop skull base osteomyelitis as a consequence of malignant external otitis media. Pseudomonas Aeruginosa is typically the causative agent. Infected PNS or dental caries may also lead to the spread of infection to the skull base. In rare instances, it can be hematogenously transmitted [12]. The majorities of cases of HP are idiopathic and exhibit an excellent response to steroids. In most instances, patients undergoing steroid therapy demonstrate early improvement and a positive clinical response without the need for additional drugs. In cases where there is no response to steroids or when high doses of corticosteroids are necessary, immunomodulators, like methotrexate or azathioprine, can be used [13]. Certain authors propose that inflammatory myofibroblastic tumor (IMT), Tolosa-Hunt syndrome (THS), and idiopathic HCP could represent a wide range of manifestations within the spectrum of inflammatory disorders. These conditions can exhibit diverse locations but share comparable clinicopathological and radiological findings [14].
A review of the literature shows most pachymeningitis present diffusely, and pachymeningitis due to mastoiditis is one of the rare manifestations with few cases reported. Our patient, had undergone treatment for CSOM, was still suppurating and showed features of secondary hypertrophic pachymeningitis which we speculate resulted from the adjoining infective process. Meningeal biopsy for conventional pathological analysis and immunohistochemistry with lymphocyte markers, macrophages, and IgG4 markers are imperative to establish the exact diagnosis. However, our patient was unwilling for any further surgical intervention. Currently, he is on steroids with some improvement in facial nerve paralysis.
Conclusion
This case highlights the associated finding of localized hypertrophic pachymeningitis seen in contrast-enhanced magnetic resonance imaging in a patient having chronic suppurative otitis media with recurring facial nerve paralysis. Previous history of mastoidectomy and imaging findings of persistent inflammation, led to the diagnosis of hypertrophic pachymeningitis associated with CSOM. Learning points –
- Localised bilateral symmetrical pachymeningitis is a rare complication of chronic otitis media and mastoiditis.
- Diagnostic imaging, including CT and CE-MRI, is essential for identifying the inflammatory changes in the meninges associated with HP.
- Causes of HP include infectious and inflammatory conditions like syphilis, TB, IgG4-RD, ANCA-AV, fungal meningitis, etc.
- Steroid therapy is often effective in treating HP; however, refractory cases may require immunomodulators like methotrexate or azathioprine.
MCQs
1. Which of the following layers are involved in pachymeningitis? a. Dura matter + Pia matter b. Pia matter + Arachnoid c. Dura matter + Arachnoid d. Dura matter only Answer key - d
2. Which of the following is not a potential etiological factor for secondary pachymeningitis? a. Viral infection b. Rheumatoid arthritis c. Primary brain tumor d. Meningiomas Answer key – c
3. Which imaging modality is commonly used to diagnose pachymeningitis? a. CT b. MRI c. USG d. X-Ray Answer key – b
4. What is the characteristic radiological finding associated with pachymeningitis? a. Enlarged ventricles b. Diffuse cortical atrophy c. Thickened dura matter d. Focal white matter lesions Answer key - c
References
-
Karthik S, Bhanu K, Velayutham S, Jawahar M (2011) Hypertrophic pachymeningitis. Ann Indian Acad Neurol 14(3): 203-204.
-
Fain O, Mekinian A (2017) Pachymeningitis. Rev Med Interne 38(9): 585-591.
-
Kupersmith MJ, Martin V, Heller G, Shah A, Mitnick HJ (2004) Idiopathic hypertrophic pachymeningitis. Neurology 62(5): 686-694.
-
Kazem IA, Robinette NL, Roosen N, Schaldenbrand MF, Kim JK (2005) Idiopathic Tumefactive Hypertrophic Pachymeningitis. RadioGraphics 25(4): 1075-1080.
-
Abdelrazek MA, Venna N, Stone JH (2018) IgG4-related disease of the central and peripheral nervous systems. Lancet Neurol 17(2): 183-192.
-
Khosroshahi A, Mollie NC, John HS, Shweta S, Nisha S, et al. (2013) Rethinking Ormond’s Disease: “idiopathic” retroperitoneal fibrosis in the era of IgG4-related disease. Medicine 92(2): 82-91.
-
Yamamoto M, Hiroki T, Mikiko O, Chisako S, Yasuyoshi N, et al. (2006) A new conceptualization for Mikulicz’s disease as an IgG4-related plasmacytic disease. Mod Rheumatol 16(6): 335-340.
-
Aragones JM, Arias RM, Garcia BJM, Lucchetti G (2015) [IgG4- and MPO-ANCA-associated hypertrophic pachymeningitis]. Rev Neurol 61(10): 454-457.
-
Kanzaki S, Inoue Y, Watabe T, Ogawa K (2004) Hypertrophic chronic pachymeningitis associated with chronic otitis media and mastoiditis. Auris Nasus Larynx 31(2): 155-159.
-
Zunt JR (2018) Tuberculosis of the Central Nervous System. Continuum 24(5): 1422-1438.
-
Laurens MB, Becker RM, Johnson JK, Wolf JS, Kotloff KL (2008) MRSA with progression from otitis media and sphenoid sinusitis to clival osteomyelitis, pachymeningitis and abducens nerve palsy in an immunocompetent 10-year-old patient. Int J Pediatr Otorhinolaryngol 72(7): 945-951.
-
Caldas AR, Brandao M, Paula FS, Castro E, Farinha F, et al. (2012) Hypertrophic cranial pachymeningitis and skull base osteomyelitis by pseudomonas aeruginosa: case report and review of the literature. J Clin Med Res 4(2): 138-144.
-
Bosch J, Ortega-Aznar A, Tintore M, Rio J, Ferreira R, et al. (2000) [Hypertrophic pachymeningitis. A review of the histories of two cases and pathological relationship with the Tolosa-Hunt syndrome and the orbital pseudotumor]. Rev Neurol 31(10): 946-951.
-
Wasmeier C, Pfadenhauer K, Rosler A (2002) Idiopathic inflammatory pseudotumor of the orbit and Tolosa-Hunt syndrome--are they the same disease? J Neurol 249(9): 1237-1241.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage