Imaging Modalities for Breast Cancer: Role of the Radiologist
Breast cancer is the third most common cancer in the world after lung and colon , and overall the commonest cancer among women in India. Early detection and diagnosis help in providing early treatment to the patients thereby significantly impacting overall survival rate. The different imaging modalities at our disposal include ultrasonography, mammography and magnetic resonance imaging and computed tomography. Over and above, nowadays with emergence of breast conservative surgery for early stage cancers the role of the radiologist in performing various imaging guided breast interventions is also evolving. Imaging guided breast biopsies, marker placement, stereotactic biopsy, wire localization are some of the commonly performed procedures by breast radiologists in addition to other pain and palliation measures as described later in the article. In this review / perspective article, therefore, we try to discuss the salient features of the common imaging modalities available for breast cancer detection and staging as well as explore the emerging role of imaging guided interventions for breast cancer in this era of multidisciplinary approach.
Introduction
After lung and colon cancer, breast cancer ranks third among all cancers that affect women globally. Approximately 1.7 million new cases of cancer were reported globally in 2012, with a mortality rate of approximately 31%. In developing nations, there is a trend toward an increase in the overall prevalence and death rate of breast cancer. The most common cancer among Indian women is breast cancer. It is responsible for 26.3 percent of newly diagnosed cancer cases and 23.5 percent of cancer-related deaths in India’s female population [1]. Early detection techniques can raise survival rates to roughly five years, according to clinical research. Breast lumps, fixed masses with irregular or poorly defined borders, retraction, thickening, discoloration, dimpling, nipple discharge, and pain in the breast or nipples are important indicators of this cancer [2]. Utilizing low energy 20–30 keV X-rays, mammography imaging is currently the accepted standard method for both screening and diagnosis. The most effective technique for identifying breast cancers is post contrast enhanced dynamic MRI (DCE MRI), which employs injectable intravenous gadolinium. Sonography is the third modality. In this article, we’ll go over the key characteristics, benefits, interpretations, and clinical implications of the various imaging modalities. According to a study, the sensitivity of diagnosis for mammography with manual examination was as low as 74%, whereas the sensitivity for mammography and ultrasound used concurrently was 97% [1].
Mammography
The most recent NCCN guidelines for the workup of breast cancer suggest bilateral diagnostic mammograms following a history and physical examination. Regular mammography screening is also carried out in women who are asymptomatic. Furthermore, physical examination findings such as lumps and palpable masses are suggestive of a mammogram. The purpose of mammography, a unique kind of x-ray imaging, is to get precise pictures of the breast. Low atomic weight alloy targets (such as molybdenum and rhodium) are used in mammography to produce low KVp x-rays. The patient’s radiation exposure is reduced by using filters composed of aluminum, molybdenum, rhodium, beryllium, or palladium to remove photons that don’t contribute to the image. In order to image and examine as much tissue as possible, breast compression techniques are used to flatten the breast. Moreover, it permits the immobilization of the breast to lessen motion blur. Additionally, it guarantees that the breast tissue receives a lower dose of x-rays. In addition to lowering scatter radiation, compression results in sharper images. Every year, patients receive a lower radiation dose from mammograms than from background environmental or terrestrial sources. It is therefore regularly advised because the substantial decrease in breast cancer mortality considerably outweighs the dangers and discomfort of the test [1, 3].
Screening X-Ray Mammography
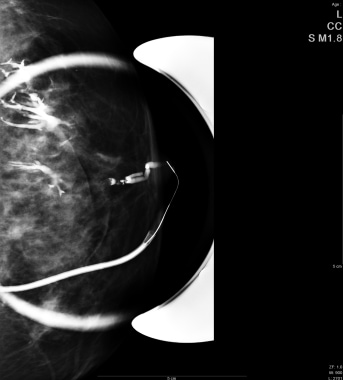
Screening and diagnostic mammograms are the two types of exams. The majority of women who have no symptoms have screening mammography. The cranial- caudal (CC) and medio-lateral-oblique (MLO) projections typically yield two images of each breast during a screening mammography [2].
Diagnostic X-Ray Mammography
Women who exhibit symptoms such as breast lumps or discharge from their nipples are referred for diagnostic mammography. To image the surrounding tissue and lymph nodes or to ascertain the size and location of breast abnormalities, diagnostic mammography may employ additional views. Among these additional views are medio- lateral (ML) and latero-medial (LM), spot compression, magnified CC, and magnification. To identify specific lesions, skin abnormalities, the nipple, and other areas, special skin markers may occasionally be used [2].
American College of Radiology Breast Imaging Reporting and Data System
In order to direct the routine diagnostic and screening process for breast cancer, the American College of Radiology (ACR) created the Breast Imaging Reporting and Data System (BI-RADS). In order to perform adequate breast mammography examinations, interpret the results, report the results, and communicate recommendations to patients and other medical colleagues, a standardized system was developed by the BI-RADS Atlas. Magnification, ultrasound, and magnetic resonance imaging (MRI) have their own guidance chapters in the ACR BIRADS atlas. For this reason, the BI-RADS system is designed to help radiologists and referring doctors standardize and streamline patient care during the breast cancer decision-making process [3, 4] (Figures 1 & 2).
Interpretation of Mammograms
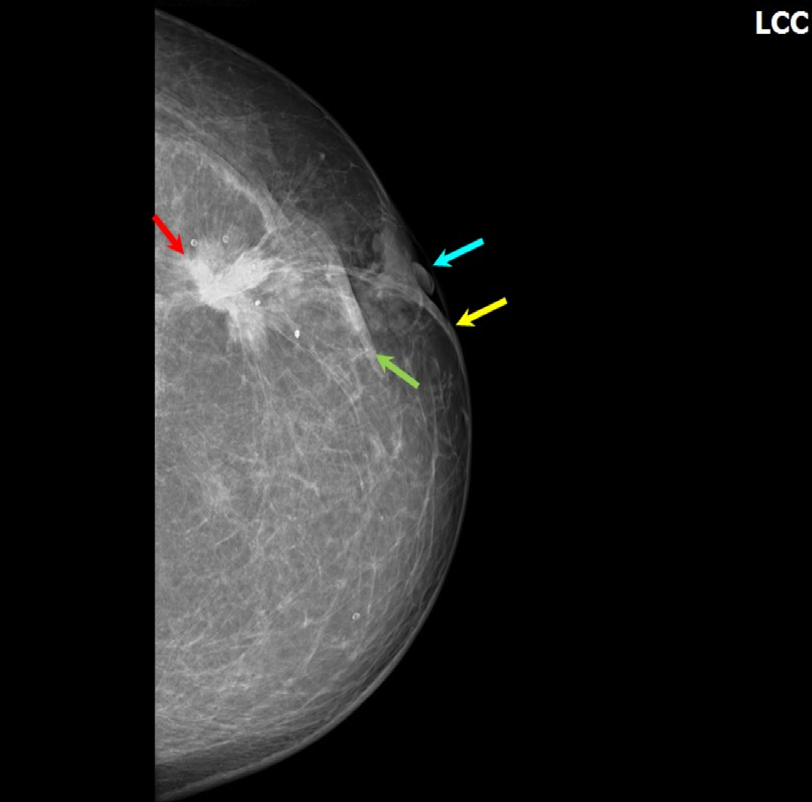
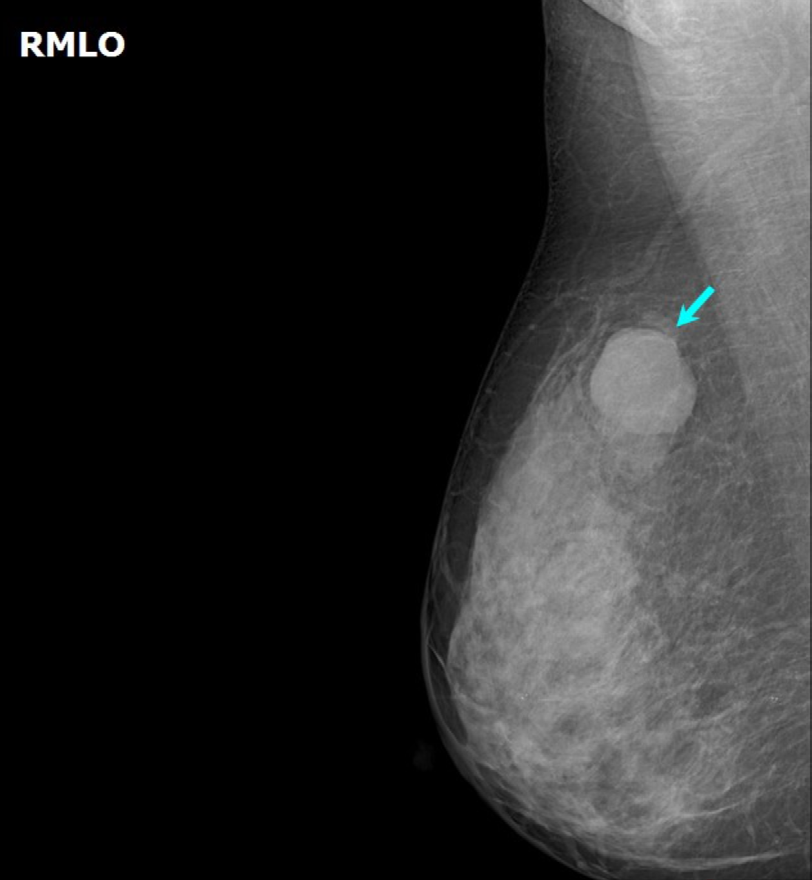
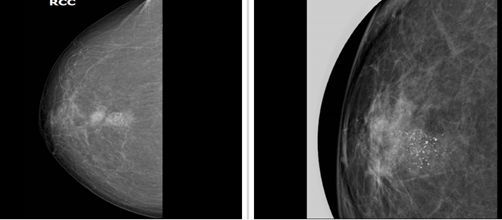
Repeat imaging may be considered in the event of sub optimally acquired mammographic views. The mammograms are closely examined. Targeting comparable or corresponding areas in both breasts, the search is conducted methodically. The radiologist’s job is to determine if the results are benign, normal, or suspicious enough to require tissue biopsy or sampling. Initially, the symmetry, size, overall density, and glandular distribution of the breasts are noted. After that, an investigation is carried out to look for masses, densities, calcifications, architectural distortions, and related discoveries. The density, shape, and margins of masses are examined. It is possible for benign and malignant masses to share characteristics. Benign masses frequently have an oval or round shape with bounded edges. Usually, the margins of malignant lesions are spiculated, uneven, or unclear [1, 4] (Figures 3 & 4).
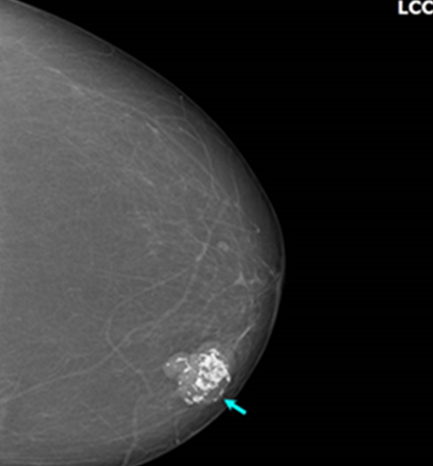
Compared to healthy breast tissue, malignancies typically have densities that are larger. When very low density fat is present in a lesion, benign findings like oil cysts, hamartomas, lipomas, and galactoceles are frequently suggested. A benign breast process or cancer could be indicated by calcifications. The majority of benign calcifications are larger, coarser- looking, round, and easily noticeable. Eggshell calcifications in cyst walls, tramlike calcifications in arterial walls, popcorn-type calcifications in fibroadenomas, large, rod-like calcifications with potential branching in ectatic ducts, and tiny calcifications in the skin with a lucent centre are several examples of the distinct shapes that benign calcifications typically take [1, 4] (Figure 5).
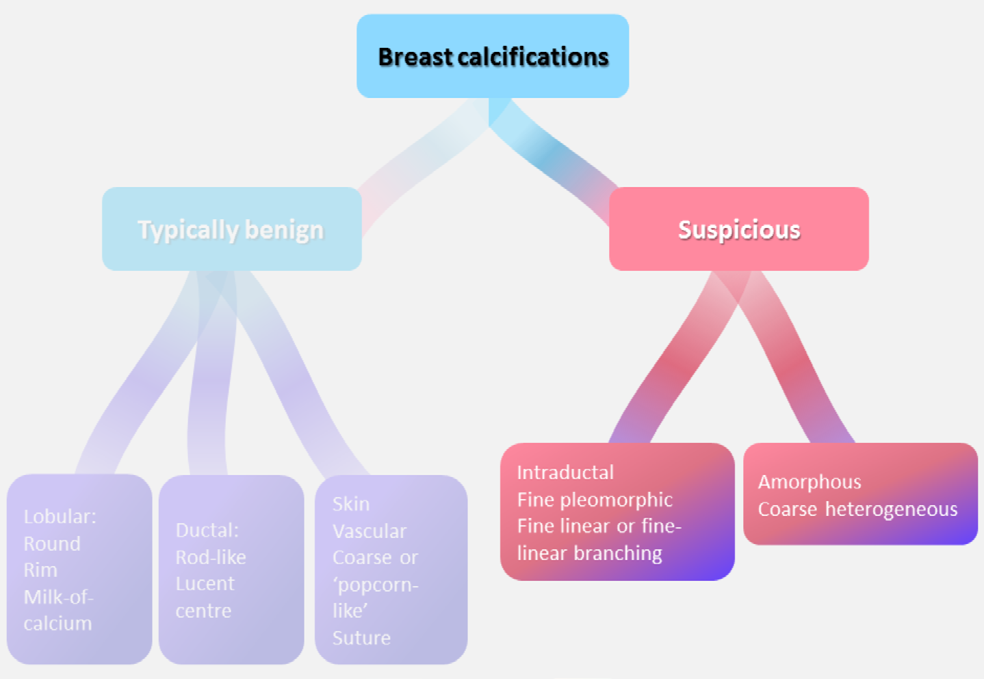
Malignant calculi are typically small (< 0 point 5 mm), and in order to make an accurate assessment, they frequently require spot magnified views or digital zooming. With fine granular, fine linear, or branching (casting) shapes and forms, they typically have a pleomorphic or heterogeneous shape. Grouping, clustering, linear, segmental, regional, and diffuse are some possible descriptions for the calcifications’ distribution. An intramammary lymph node-typical reniform- shaped mass with a radiolucent center or a linear density that could indicate a duct full of secretions are examples of unusual findings. These typically indicate benign findings more strongly [3, 4] (Figures 6 & 7).
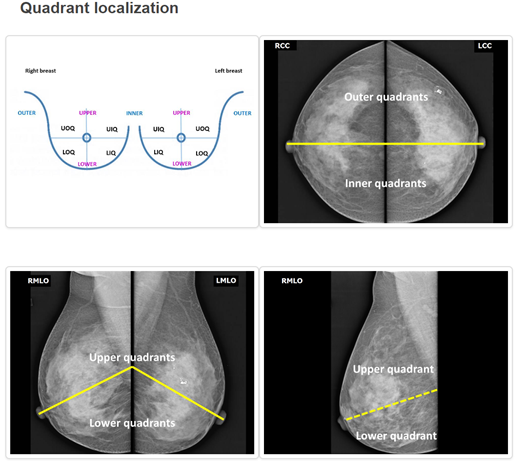
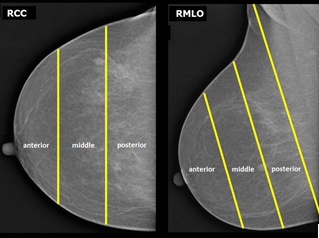
The following are associated findings: axillary adenopathy, skin or nipple retraction, trabecular thickening, focal or diffuse skin thickening, skin lesions, and architectural distortion. Lesions classified according to their location can be found in a quadrant, central, retroareolar, or, more accurately, at a clock position. Positioned with the patient facing the observer, the breast is perceived as the face of a clock. The anterior, middle, or posterior third of the breast may be identified as the location of the lesion depending on extent. For evaluating the course of the disease, a comparative analysis is helpful if prior exam pictures are available. Once a final assessment is made and a BI-RADS category is assigned, all of these findings are combined [1, 2].
Breast Density
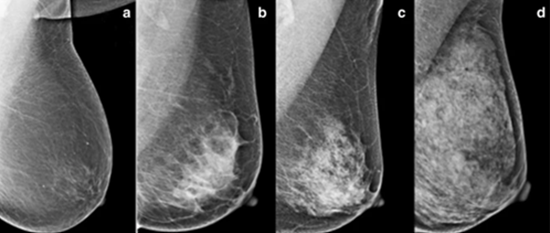
Breast density can only be determined by mammography. It shows the proportion of fat, which appears dark on a mammography, to glandular tissue, which appears white. A breast that is almost entirely composed of fat is classified as category A, and a breast that is almost entirely composed of glandular tissue is classified as category D. These are the four categories into which it can be placed in the BI-RADS atlas. Breast density affects both the risk of breast cancer development and the interpretation of mammograms. Research has demonstrated an inverse relationship between density and the sensitivity of breast cancer detection. It is between 50 and 65 percent in dense breasts (category D) and up to 98 percent in fatty breasts (category A). Furthermore, breast density is positively correlated with the risk of developing breast cancer. Compared to women with fatty category A breasts, those with very dense category D breasts have a four-fold higher relative risk of developing breast cancer [3] (Figure 8).
BI-RADS assessment categories can be summarized as follows: Category 0 - Need additional imaging evaluation Category 1 - Negative Category 2 - Benign finding, noncancerous Category 3 - Probably benign finding, short-interval follow- up suggested Category 4 - Suspicious abnormality, biopsy considered Category 5 - Highly suggestive of malignancy, appropriate action needed Category 6 - Known cancer, appropriate action should be taken
Treatment by BIRADS Category
Each BI-RADS level recommends or corresponds to the associated plan of management or follow-up including risks of malignancy as shown in Table 1 below [4].
| Category | Description | Risk of Malignancy | Care Plan and Comments |
|---|---|---|---|
| 1 | Negative | 5 in 10,000 | Continue annual screening mammography for women 40 years of age or older. |
| 2 | Benign finding, noncancerous | 5 in 10,000 | Continue annual screening mammography for women 40 years of age or older. This category is for cases with a characteristically benign finding (eg, cyst, fibroadenoma). |
| 3 | Probably benign finding | < 2% | Usually, 6-month follow-up mammography is performed. Most category 3 abnormalities are not evaluated with biopsy. |
| 4 | Suspicious abnormality | A-2 to 10%, B – 10 to 25 % , C - 25- 50% | Most category 4 abnormalities are benign but may require biopsy. |
| 5 | Highly suggestive of malignancy | 50-99%, depending on how individual radiologists define categories 4 and 5 | Classic signs of cancer are seen on the mammogram. All category 5 abnormalities are typically evaluated with biopsy; if the results are benign, repeat biopsy is done to ensure correct sampling. |
| 6 | Biopsy proven malignancy | Surgery, Chemotherapy, Radiation as recommended. |
Table 1: Risk of malignancy and care plan by BI-RADS category.
Postoperative Mammograms
Mammograms for breast cancer screening are necessary for women who have had prior breast cancer surgery. Following a total mastectomy, it is advised to do an annual screening of the breast on the opposite side. Annual screening for the treated breast is advised in cases of subcutaneous, nipple-sparing, partial mastectomy/lumpectomy. Six months following surgery, a baseline mammography of the treated breast is typically performed to document changes resulting from radiation and surgery. After that, screening and follow- up mammograms can be done every six to twelve months [5].
Digital Breast Tomosynthesis
Using a 3D volume acquisition along with the compression and views of 2D mammography, digital breast tomosynthesis, or DBT, is another name for 3D mammography. The whole breast volume is seen on a single 2D image in a traditional 2D exam. Dense parenchyma can mimic cancer by growing over normal breast tissue and can also cause cancers to go undetected by superimposing over them. The radiology technician can identify hidden lesions or cancers by using the DBT acquisition, which increases sensitivity, when it is shown on a monitor in slices as thin as 1 mm. Along with reducing the need for pointless recalls and enhancing specificity, it ought to assist in differentiating between cancers and healthy tissue. Yet, because the DBT examination starts with the four standard views of 2D screening mammography and then moves on to the four tomosynthesis views, it typically exposes the breast to twice as much radiation as 2D digital mammography. That dose is still far lower than the FDA screening mammography limit, nevertheless. Moreover, contemporary high-end mammography equipment has a software-based reconstruction algorithm that converts the DBT images into a 2D picture. For a DBT exam, the dosage is therefore the same as for a 2D exam, but with increased sensitivity and specificity. As a result, it has been said that “breast tomosynthesis has demonstrated to be an improvement over digital mammography, with higher rates of cancer detection and fewer patient recalls for added testing [6].
Digital Subtraction and Contrast-Enhanced Digital Mammography
Contrast-enhanced digital mammography (CEDM) was created to address the lower sensitivity of mammography in dense breasts and the high expense of MRI. However, it is not commonly utilized for screening, but is occasionally used for cancer staging or follow-up in situations where MRI is not readily available. The contrast resolution of CEDM is not as high as that of CT or MRI. Subtraction methods can be carried out using temporal or dual-energy techniques [6].
Other Uses of Radiography in Breast Cancer
While a patient presents with nipple discharge, a ductogram, also known as a galactogram, can be used to obtain images of the lumen of a single duct and aid in the detection of intraductal pathologies. A fine 30-gauge plastic tube is inserted into the nipple’s suspected duct opening in this procedure. To outline the shape of the duct on a mammogram and determine whether a lesion is present inside the duct, a small amount (0.1 to 0.3 cc) of iodinated contrast medium is injected [1, 7] (Figure 9).
Ultrasound
An effective imaging method for assessing breast disease is breast ultrasonography. The screening of dense breast parenchyma is particularly advantageous due to its affordability and accessibility. The combined sensitivity of mammography and ultrasound for the detection of breast cancer rises to 97.3%, with an estimated false positive rate of 24% for ultrasound [8]. The anatomy and physiology of the breast are composed of 15 to 20 lobules, which are made up of smaller breast ducts called terminal duct lobular units (TDLUs). Each of these ducts empties into a separate lactiferous sinus that leads to the nipple. The fatty, fibroglandular, and muscular premammary, mammary, and retromammary zones are the three primary anatomical zones of the breast. Between the superficial fascia immediately deep to the skin and the deep fascial layer superficial to the pectoralis muscle are breast fat and fibroglandular tissue. The breast can be seen as being separated into different hypoechoic and hyperechoic layers on ultrasound imaging. The hyperechoic fibrous bands found in skin; the hypoechoic fat lobules found in subcutaneous fat; the hyperechoic fibroglandular soft tissue found in breast parenchyma; the hypoechoic fat lobules found in retiramammary fat; and the hyperechoic fibrous tissue found in pectoralis major muscle [8, 9].
When assessing nodal disease, the axillary regional anatomy is crucial. The axillary artery and vein, as well as lymph nodes, are located in the axilla. An echogenic, fatty hilum is seen in normal lymph nodes, and the hypoechoic cortices are smaller than 3 mm. The internal mammary (internal thoracic), lateral thoracic, and thoracoacromial artery branches of the axillary and subclavian arteries supply blood to the breast. Only a small portion of the lymphatic drainage originates from the internal mammary chain; the majority empties into the ipsilateral axillary nodal basin. Generally speaking, the ipsilateral axillary nodes supply 10% of the internal mammary chain’s lymphatic drainage and 90% of the drainage overall [8.10]. Breast ultrasound is commonly used to identify the following conditions: palpable lump during clinical breast evaluation; axillary lymphadenopathy on mammography; women under 40 years of age with clinical symptoms such as breast lump; suspicious abnormality identified on mammography imaging; breast discharge; skin retraction or inversion of the nipple; surgical scarring evident on mammography imaging; gynecomastia in males; suspicion of ruptured breast implants to distinguish between intra- and extra-capsular ruptures; needle-guided percutaneous breast biopsy; and follow-up of patients receiving neoadjuvant chemotherapy [8].
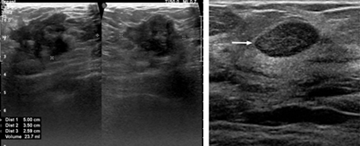
The following characteristics are taken into account when reporting and evaluating masses [9, 10, 11]: Shape: Oval, round, or irregular. Oriental: Parallel or not parallel. Margin: Circumscribed or not circumscribed (further described as indistinct, angular, microlobulated, or spiculated). Echo pattern: Anechoic, hyperechoic, complex cystic and solid, hypoechoic, isoechoic, heterogeneous. Posterior features: No posterior features, enhancement, shadowing, combined pattern (mixed enhancement and shadowing).
On ultrasonography, calcifications can occasionally be seen. If this happens, the location of these foci—whether inside or outside of a mass—should be noted. Architectural distortion, skin thickening or retraction, vascularity (internal or rim), alterations to the related ducts, and elasticity classification (soft, intermediate, or hard) are additional associated features of sonographic findings that should be assessed. Simple cysts, clustered microcysts, complex cysts, masses in or on the skin, foreign bodies, lymph nodes, vascular anomalies like Mondor disease, and arteriovenous malformations are among the findings that have a pathognomonic appearance. Seromas and fat necrosis can also be reliably diagnosed with ultrasound based on clinical history.
Clinical Significance
A comprehensive ultrasonography examination and interpretation of the breast should culminate in a standard breast report that includes the patient’s indications, findings, and results along with additional diagnostics. Both longitudinal and transverse planes are used to measure any lesions found during the examination. Each mass’s location, dimensions, and echogenicity are classified as hypoechoic, hyperechoic, or heterogeneous. The US BIRADS lexicon, which consists of six primary morphological descriptors for breast masses, is used to determine the appropriate use of the various mass descriptors.
The most common morphologic features associated with benign sonographic findings are as follows [9]:
- Smooth and well-circumscribed margins.
- Hyperechoic, isoechoic, or mildly hypoechoic in echogenicity.
- Thin echogenic capsule or well-defined capsule border.
- Ellipsoid shape, wider than tall appearance.
- Macrolobulated; <3 lobulated margins.
- Posterior acoustic enhancement.
- The most common morphologic features associated with malignant findings are as follows:
- Hypoechoic mass, occasionally appearing hyperechoic in appearance.
- Spiculated margins.
- Ill-defined borders, architectural distortion of surrounding soft tissue.
- Taller than wide appearance.
- Microcalcifications present.
Males who have clinically significant fibroglandular tissue usually have a palpable “flame-shaped” focal area of retroareolar fibroglandular tissue. Gynaecomastia is a condition where males with otherwise primitive breast tissue grow larger due to the hormonal effects of certain medications, including drug abuse (Figure 10).
Magnetic Resonance Imaging
Breast MRI has demonstrated utility in high-risk screening, assessment of unclear primary, multicentricity and bilateral evaluation of disease extent, particularly in dense breasts, distinction of scar from local recurrence in women undergoing breast conserving surgery, assessment of response to neoadjuvant chemotherapy, and assessment of implant integrity. Performing a dynamic contrast enhanced (DCE) MRI is the standard recommendation. The foundation of neoangiogenesis is the application of contrast-enhanced magnetic resonance imaging. Gadolinium is absorbed more readily and washes out more quickly in tumor-associated blood vessels due to their higher vascular permeability. Breast cancers can be distinguished from benign lesions by the morphology of the lesions, as well as by the enhancement and washout kinetics. Distinguishing between benign and malignant lesions can be difficult due to breast MRI’s high sensitivity (over 90%) and low to moderate specificity (72%). For particular interrogations, MRI is typically used as a problem-solving tool [12, 13, 14] (Figure 11).
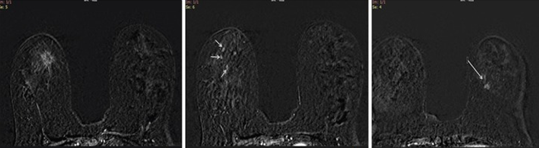
Figure 11: a) Post contrast dynamic MRI axial view showing a contrast enhancing spiculated lesion in the right breast corresponding to the mammographic image. HPE confirmed a tubular carcinoma. b) In addition, there were other areas of contrast enhancement in the right breast. Histopathology of these lesions confirmed an invasive lobular carcinoma. c) The left breast enhancing lesion was reported to be an invasive ductal carcinoma.
Because of its low specificity, which necessitates additional biopsies and increases time and expense associated with technology, MRI is not widely used for screening women at average risk. Breast MRI preferentially detects higher-grade lesions because it does not depend on breast density like 2D mammography does and instead uses intravenous contrast administration (Gadolinium) to detect tumor angiogenesis [13, 15].
Breast Magnetic Resonance Imaging and Ductal Carcinoma In Situ (DCIS)
When microcalcifications are present on a mammography, DCIS is typically detected. The tumor gets larger than its blood supply, experiences necrosis, and calcifies inside the ducts and terminal ductal units. These calcifications are not identifiable by MRI. But because the tumor cells’ protease activity allows gadolinium to enter the ducts through the leaky basement, MRI can identify the non-mass enhancement characteristic of DCIS. So, it’s possible that MRI will identify the higher grade lesions that are more clinically relevant. A mammography can easily detect low-grade DCIS, which an MRI might miss. Furthermore, a mammography may miss 10- 15% of DCIS that present as non-calcifying DCIS, but an MRI will reveal their presence. The characteristic presentation of DCIS in approximately 70–80% of cases is non-mass enhancement with a ductal or segmental distribution and clumped or stippled morphological appearance. Within a focal area or regional distribution, a focus or mass makes up the remaining 20–30% of the different enhancement patterns. Variability in the kinetic curves makes them less indicative of invasive or DCIS cancers [15].
The Role of Breast Magnetic Resonance Imaging in Preoperative Evaluation
Breast MRI is not always used in the preoperative assessment of women with breast cancer. Preoperative MRI is helpful, particularly in patients with lobular cancers and dense breasts, in detecting multifocal and multicentric lesions as well as evaluating the contralateral breast. Nonetheless, it is determined that pre-operative magnetic resonance imaging may be linked to a higher likelihood of patients not undergoing ipsilateral mastectomy and contralateral prophylactic mastectomy. Surgery planning may benefit from an MRI’s ability to more precisely define the tumor’s size and extent. With a decline in local recurrence rates, this is anticipated to lower re-excision rates and raise overall survival rates. But it also increases the number of follow-up biopsies, causes anxiety in patients, raises costs, postpones the start of treatment, and may even raise the incidence of mastectomy. Thus, unless there is a strong indication, MRI is not performed routinely for preoperative assessment [15, 16].
MRI is indicated for special cases as follows as per American College of Radiology (ACR) guidelines:
- High-risk screening.
- Personal history, family history.
- BRCA1 / BRCA2 gene positivity.
- Radiotherapy (>4 gray).
- Li-Fraumeni syndrome +/- first-degree relatives.
- Cowden and Bannayan-Riley-Ruvalcaba syndromes and first-degree relatives.
- Extent of disease (EOD) evaluation in ipsilateral and contralateral breast.
- Positive margins (better accuracy further from lumpectomy site than near lumpectomy site due to postoperative changes).
- Neo-adjuvant chemotherapy: to assess residual disease.
- Metastatic axillary lymphadenopathy of unknown primary (75 - 80% sensitive) - can spare a patient from having management because may be able to undergo BCT; management path only finds cancer in two-thirds.
- Posterior lesion to assess chest wall invasion ,chest wall stage IIIB - serratus anterior muscle, rib, intercostal muscles.
Other indications
- Problem-solving (e.g. post-operative breasts with distortion).
- Recurrent breast cancer/scar changes (not usual before 2 - 3 years; peak 5 - 7 years; increased risk if EIC, younger age, positive margins (wait at least 1 month postop to scan), no radiotherapy).
- To assess for synchronous, multifocal or multicentric disease.
- Patients with breast implants.
- Inflammatory / infective breast parenchymal disorders.
Computed Tomography
Metastatic work up and staging with CECT (Contrast Enhanced) thorax and whole abdomen may be done for HPE proven malignancies whenever cost or logistic constraints are present. However, for all practical purposes PET CT should be preferred modality for preliminary metastatic work up of breast cancer.
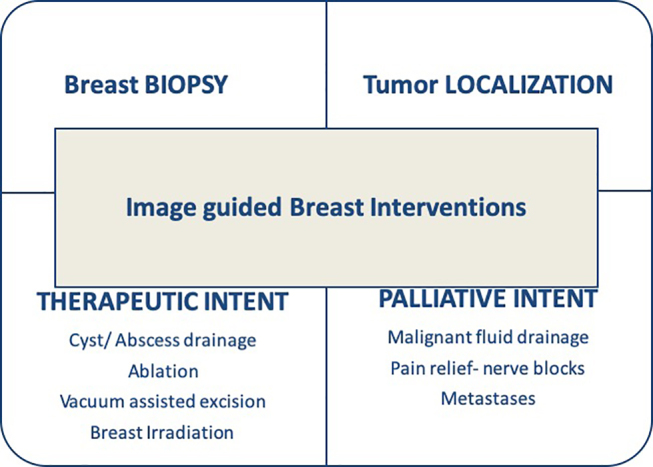
Imaging Guided Breast Interventions
The role of a breast radiologist and an interventionist in the diagnosis and treatment of breast cancer has expanded due to the multidisciplinary approach, personalized care, and breast conservation treatment. The most common image- guided breast intervention is a breast biopsy for suspicious abnormalities. Comparing image guidance to blind biopsies, more precise and sufficient tissue sampling is ensured, and fewer biopsies are required. Additional treatment options based on the tumour’s hormonal (ER, PR, and HER2/neu) receptor status can only be considered after histopathology confirmation. Breast conservative surgery (BCS) is feasible for patients exhibiting a good response when neoadjuvant chemotherapy (NACT) is administered prior to surgery for larger tumours. About 20 to 25 percent of patients respond completely clinically and radiologically to NACT when using more recent, enhanced chemotherapy drugs. Nevertheless, this requires the use of tumor marker clips to localize the tumor site either prior to or during chemotherapy before the tumor fully disappears. Prior to surgery, these marker clips act as a localization point for the placement of the hookwire using image guidance [17, 18] (Figure 12).
Breast Biopsy
The primary indications for a breast biopsy are breast lesions categorized on imaging as BIRADS 4 (suspicious) or BIRADS 5 (highly suspicious). Greater palpable lesions are biopsyed by blind percutaneous technique; nonpalpable, small, deeply seated, or ill-defined masses require biopsyed by image-guided technology. However, blind biopsy is linked to high rates of false negative results and repeat biopsies, highlighting the necessity of image-guided biopsies even when there are palpable lesions because of sampling error. Depending on the operator’s preference and the visibility of the lesion with a particular imaging modality, an image-guided breast biopsy can be carried out using MR, ultrasound, or mammography (stereotactic) guidance. When there is a clear ultrasound demonstration of the breast lesion, ultrasound is the most often used modality (US). Mammography masses and microcalcifications will be subjected to stereotactic biopsy. Likewise, lesions visible only on MRI may be subjected to MR-guided biopsy. Bias guns, or spring-loaded automated 14-gauge core biopsy needles, are frequently used for breast core needle biopsies.
Typically, small caliber (16 or 18 gauge) biopsy needles intended for other body parts are not appropriate for use in breast biopsies. A breast biopsy should typically yield four or five cores at the very least [17].
Vacuum-Assisted Biopsy: The late 1990s saw the introduction of vacuum-assisted breast biopsy (VAB), a refined and modified technique of large core breast biopsy. A motor-driven outer cannula with a sample notch and an inner cutting cannula make up the probe (needle) in this apparatus. A powerful suction pulls the targeted tissue into the sample notch, holds it there, and moves the sectioned cores into a collection chamber outside. With the needle rotating 360 degrees, these devices enable multidirectional sampling from various lesion locations, yielding up to 12 or 20 cores. Depending on the vendor and apparatus, VAB typically uses thick caliber needles with a gauge range of 11 to 7. The primary benefit of VAB is its one-time insertion through a tiny skin incision and faster acquisition of several large tissue cores in a contiguous manner. Furthermore, it permits the use of a strong suction and normal saline irrigation of the biopsy cavity simultaneously with a local anaesthetic agent, thereby decreasing the risk of hematoma formation. Smaller lesions may be totally removed during VAB because of its capacity to remove large volumes of tissue. Because VAB is more accurate than CNB in terms of histological confirmation, false negatives, and the need for rebiopsy, it is necessary to place a tumor marker clip at the biopsy site to guide subsequent surgery in the event that the histopathology result is positive for cancer. A negative predictive value of up to 99.9 percent is possible. Therefore, VAB is regarded as being equivalent to excision [17, 18] (Figure 13).
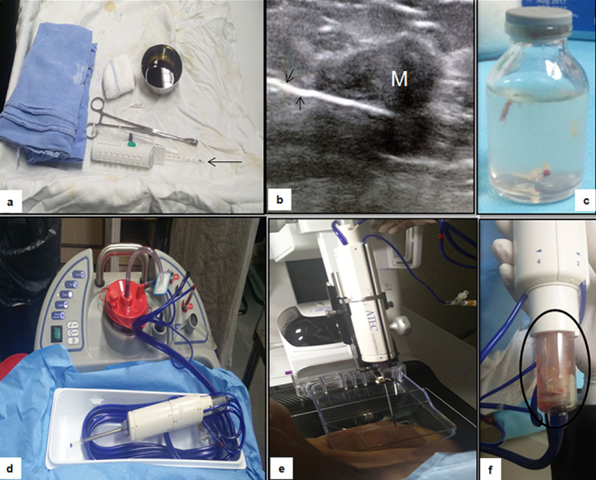
Figure 13: Breast biopsy. Panel (a–c) demonstrates prepared sterile tray with 14-gauge core biopsy needle (arrow in a) with sterile drapes and other accessory items needed. The cores obtained under USG guidance (arrows in b) have settled or are semi-floating in the container (c). Apparatus for vacuum-assisted biopsy (d–f) and the cores get collected in sample notch using vacuum (f) which is then shifted to the formalin bottle.
Tumor Localization Techniques
For patients with small tumor to breast volume ratios, breast conservative surgery (BCS) is being performed more frequently. This allows for locoregional disease removal with clean margins and good cosmesis. When a mastectomy is not an option for locally advanced breast cancer, NACT lessens the tumor burden, enabling BCS. Before surgery, NACT completes the resolution of radiological abnormality and clinically palpable mass in many patients. In order to precisely localize the tumor site at the time of or prior to surgical excision, a number of cutting-edge techniques have been described, including skin marking, imaging-guided radio-opaque tumor marker placement, and the use of custom-made clips made of angiographic wire, commercially available marker clips, radioactive seed (I-125), Magseeds, and radiofrequency identification. Comparing patients who have surgery without tumor marker placement, those who have tumor marker clips placed have a lower chance of experiencing a local recurrence [17, 18].
Preoperative Hook Wire Localization: Previously, surgical excision biopsy of clinically nonpalpable lesions was a common use for this procedure. Placement of two or more hookwires in the same breast may be necessary for multiple lesions to mark the extent of a large lesion and for segmental microcalcifications before breast conservation surgery. However, with the advent of stereotactic biopsy, it is now primarily used as a preoperative localization method prior to therapeutic excision of already diagnosed but nonpalpable breast cancer dot. The most popular hookwire bracketing. The assembly is made by Kopan and is referred to as needle- hookwire assembly. It has a thin, flexible wire that can be introduced through it and a 20-gauge needle. The wire’s distal end retracts to form a sharp angle or has a curved J tip that can be folded back. Usually, on the day of surgery, needle localization is done under US or mammographic guidance. There are also MR-compatible needle hookwire assemblies available to help locate lesions visible only on MRIs [17] (Figure 14).
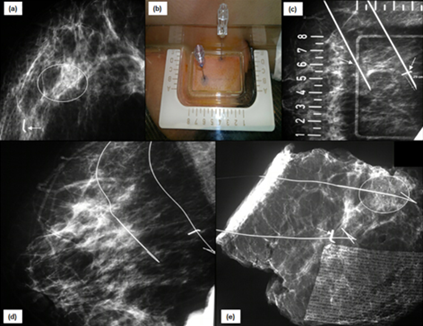
Figure 14: Hookwire bracketing: (a) Mammogram of right breast shows tumor marker clip (arrow) at the site of mass which has resolved post chemotherapy. There is another cluster of suspicious microcalcification in same quadrant (circle). (b) Both the clips and grouped microcalcifications are targeted using alphanumeric grid and two hookwires have been placed (arrows in c). This procedure is known as “hookwire bracketing.” The position of wires is confirmed on MLO view (d). Subsequently performed specimen mammogram (e) demonstrates and ensures removal of marker clip (arrow), microcalcifications (circle) and hookwires.
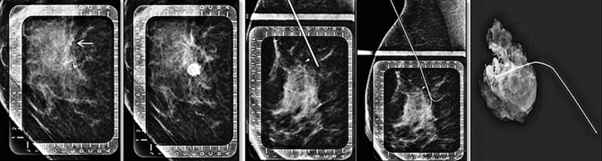
With the help of these hookwires, the surgeon dissects the breast. The thickened wire segment and the surrounding breast tissue are removed, and the specimen is sent for radiography. The confirmation should be that the resected specimen has the target lesion removed and has good margins free of tumours. In order to close the breast, the surgeon waits in the operating room for word on whether the lesion, clip, and hookwire were removed successfully (Figure 15).
A few mild side effects, such as pain, a vasovagal reaction, and bleeding, are extremely rare during this relatively safe process. When it comes to fatty breasts, the patient’s arm movement or awkward handling during surgery can cause the hookwire to unintentionally come out of place. According to reports, the range of negative margin rates following wire-localized BCS is 70.8% to 87.4%. An additional simple technique for guiding surgery is intraoperative ultrasound (IOUS). Ensuring sufficient margins free of tumors surrounding the mass during its removal lowers the frequency of re-excision in cases of BCS. Additionally, by evaluating the specimen in the operating room, it lessens the amount of normal breast tissue removed. Research found that IOUS is at least as successful as wire-guided localization in achieving negative resection margins. It is possible to achieve better cosmesis and achieve adequate excision, negative margins, and small excision volume with IOUS [17, 18].
Interventions with Therapeutic Intent
Cyst Aspiration and Abscess Drainage: Breast cysts are frequently discovered when evaluating patients with nonspecific breast complaints, such as cyclical breast pain, in conjunction with benign breast conditions. When simple cysts get big, they usually don’t cause any symptoms because they are anechoic, containing only fluid and thin, imperceptible walls. A cyst that has been classified as complicated may have moving fluid or fluid-debris levels, or it may have dense internal echoes that indicate a secondary infection or hemorrhage. They only require treatment if they are symptomatic and affecting the patient’s quality of life. Conversely, a complex cyst is one that has thick internal septations or a mural nodule that exhibits vascularity and raises the possibility of a malignancy. Biopsies should be performed on these complex cysts. A fluid sample for cytology should be sent after a cyst is aspirated while adhering to aseptic precautions and real-time USG guidance. After a simple cyst aspiration, the recurrence rate can vary from 20 to 80%. To prevent recurrence linked to aspiration, intralesional sclerotherapy is employed. The needle tip stays in the residual cyst cavity during this procedure, leaving minimal safe residual volume after the majority of the fluid volume has been aspirated. Within 10 minutes, all of the aspirated fluid is re-aspirated without the need to remove the inserted needle, using a volume of 99 percent ethanol equal to 90 percent of the original volume. Some people report mild burning pain, but it’s easily controlled [17, 18].
Elderly women, non-lactating smokers, and young lactating women are more likely to have infected simple cysts or de novo breast abscesses. Breast abscesses were previously treated with surgical incision and drainage. Nevertheless, since this was linked to the development of cutaneous fistulas in 5–12% of patients and recurrences in 10% to 38% of patients, US-guided intervention is currently the recommended alternative technique for the management of this condition because it is less invasive, more accessible, and requires less time to complete. Better cosmetic results are also achieved, there is no need for hospitalization, and breastfeeding can start again right away. After aspirating the abscess cavity, the cavity is lavaged with saline until clear saline is aspirated. For abscesses larger than 3 cm, complete resolution typically requires multiple aspirations and percutaneous catheter drainage. When multiple aspirations attempt at least five times and fail, percutaneous catheter drainage is the next step. Catheters of the 6F or 8F size are used for drainage. Vacuum-Assisted Excision of Benign Tumors: Lesions with a maximum diameter of less than 2 cm and lesions with a predominately cystic component can be completely removed with USG-guided VAB. Lesion presence in the extracted specimen and nonvisualization of the lesion on US can be used to evaluate the completeness of the procedure. Typically, a clip is placed after the procedure is finished, particularly in patients who have suspicious or solid cystic masses. A few of the complications include ecchymosis, pain, and hematoma. There have been reports of complete resection in up to 95–100% of cases for lesions smaller than 2 cm [17]. Radiofrequency & Microwave Ablation: The effectiveness of both radiofrequency and microwave ablation (RFA/MWA) plus surgery or RFA/MWA alone for early-stage breast cancer has been demonstrated in a number of studies. They cause coagulative necrosis in tumors by means of thermal energy. It works best on a single mass that is less than 2 cm in size, even though there is no set cutoff size. Lesions up to 3 to 5 cm in size can be treated with MWA. It should not be used in cases of intraductal tumor extension or invasive lobular carcinoma. To accurately characterize and localize the mass, preprocedure MRI, mammography, and ultrasonography are needed. Sentinel lymph node biopsy ought to be carried out for axillary staging prior to RFA/MWA. RFA/MWA entails inserting an electrode into the lesion while under USG guidance, then pulse-delivering the lesion until the ablation is complete and the lesion appears fully hyperechoic. The ranges for complete ablation and recurrence rate are 76–96 point-15 percent and 1–37–14 point 29 percent, respectively. Common side effects include muscle burns, skin burns, nipple retraction, and mass formation brought on by necrosis of the fat. In order to determine whether RFA/MWA is a better option than surgery, treatment outcomes in terms of long-term recurrence and survival rate still need to be assessed [18].
Interventions with Palliative Intent
There are a number of issues that significantly lower quality of life in patients with metastatic breast cancer. For patients suffering from these morbid complications, radiologists can be of great assistance in easing and lessening that suffering through various pain and palliation measures [17, 18, 19].
Recurrent Pleural Effusion: Drainage and Pleurodesis : The most frequent cause of malignant pleural effusion in women is breast cancer, which frequently manifests as dyspnea. Treatment decisions are typically based on the patient’s performance status, symptoms, response to systemic therapy, and lung re-expansion after pleural fluid drainage. Observation, therapeutic pleural aspiration, indwelling pleural catheterization (IPC), intrapleural sclerosant instillation, and pleurodesis are available treatment options. Patients with short survival times, sluggish fluid re-accumulation, and poor performance status should consider therapeutic thoracentesis. Patients with trapped lung, recurrence following pleurodesis, or unsuitability for talc pleurodesis are typically candidates for an indwelling pleural catheter. It is just as successful in relieving symptoms as pleurodesis and entails inserting a silicone catheter under image guidance into the pleural cavity. The most frequent consequence, which is frequently treated with antibiotics without requiring the removal of the catheter, is IPC-associated pleural infection. Pleurodesis is the process of obliterating the pleural space between the visceral and parietal pleura through an inflammatory response brought on by the application of chemical and mechanical agents. In patients with extended life expectancy, it is recommended for recurrent malignant pleural effusion. The agents talc, bleomycin, tetracycline, and doxycycline are often used. If pleurodesis doesn’t work, IPC or repeat pleurodesis are options (Figure 16).
Pain Management
The morbidity linked to breast cancer has increased as a result of an increase in patient survival. Pain is among the most incapacitating signs and symptoms of cancer. Analgesics and opioids are typically used conservatively to treat pain, which can be caused by a disease (local or metastatic) or developed as a side effect of treatment (surgery, radiation therapy). The earlier described drainage method is used to treat chest pain caused by pleural effusion. Pectoral nerve blocks (PECS I and II), thoracic paravertebral, serratus anterior (SA) plane blocks, and other nerve blocks can be used to provide regional anaesthesia in addition to general anaesthesia to manage perioperative pain. The effectiveness of local anaesthetics is increased by US guidance, which makes it possible to visualize drug spread in real time. In a thoracic paravertebral block, an 18-gauge lumber puncture needle is used to deposit local anaesthetic between the pleura and the costotransverse ligament, about 2.5 to 2.5 cm lateral to the tip of the spinous process. Depending on the degree and duration of analgesic requirement, it can be administered at one, two, or more levels, or with the implantation of a tiny catheter. Hypotension brought on by the drug’s epidural spread is a frequent side effect.
A newer method of regional anaesthesia called PECS blocks the median and lateral pectoral nerves by injecting an anaesthetic between the pectoralis major and minor. The pectoralis major and minor muscles are located at the level of the third rib in PECS I, with the US probe positioned obliquely beneath the lateral third of the clavicle. To block the lateral branch of the intercostal nerve, the long thoracic nerve, and the intercostobrachial nerve in PECS II, a medication is injected between the pectoralis minor and serratus anterior at the level of the fourth rib. To block the lateral cutaneous branches of the thoracic intercostal nerves, a serratus anterior plane block is administered between the latissimus dorsi and serratus muscle in the mid axillary line at the level of the fourth or fifth rib. This can be used as an alternative to thoracic paravertebral block without running the risk of epidural spread (Figure 17).
Chronic pain in patients with metastatic breast cancer is frequently attributed to painful bone metastases. bone metastasis radiofrequency ablation using radiofrequency electrode implantation guided by CT scans or fluoroscopic images while under deep sedation or general anaesthesia. It lessens pain through the generation of cytokines, the destruction of sensory nerve fibers in the periosteum and bone cortex, and the reduction of lesion volume with less stimulation of sensory nerve fibers. After that, the vertebral body can be injected with bone cement, also known as polymethyl methacrylate. Within 24 hours of the pain, there is a noticeable reduction in pain. Tumor necrosis is also encouraged and spine stability is increased.
Discussion & Conclusion
Imaging in breast cancer is usually indicated for 2 purposes: 1) Screening 2) Diagnostic Routine annual screening mammography is usually indicated for all women above the age of 40 years irrespective of any symptom or breast lump. Also for women with risk factors (as in positive family history of breast cancer) annular screening mammography is recommended above the age of 35 years. However, majority of the cases are referred to Radiology Department for diagnostic work up after presenting with clinical history of breast lump, discharge, pain, nipple / skin retraction or other changes.
Firstline sonomammography is usually recommended for such patients which are a combination of bilateral mammography followed by targeted / focussed ultrasound correlation of the abnormalities detected on the mammogram. The combination of both these methods results in combined sensitivity and specificity of upto 95 % which is not achievable with a single modality. . Mammography is especially helpful in detecting any suspicious pleomorphic calcifications which may be missed clinically or with other imaging modalities.
A final assessment is made and BIRADS categorisation (categories 1 to 6) is given to the lesion in question. BIRADS grading is also given for any other incidentally detected lesion within the breast parenchyma. Higher the BIRADS score, higher is the possibility of malignancy for a given lesion. BIRADS 1 standing for normal, BIRADS 2 usually for cysts, benign calcifications , BIRADS 3 for fibroadenomas, BIRADS 4 for equivocal / suspicious lesion, BIRADS 5 for highly suspicious lesions with upto 95% chances of malignancy and BIRADS-6 for biopsy proven malignancy. In addition to diagnostic workup , imaging ( often ultrasound ) guided biopsy is done for BIRADS 4/5 lesions under local anaesthesia whenever lesion is not clinically palpable or approachable. Ultrasound guided FNAC of axillary lymph nodes may also be done in same setting if needed. Metastatic work up and staging with PET CT or CECT (Contrast Enhanced) thorax and whole abdomen may be done for HPE proven malignancies.
Once decision regarding the clinical management of the disease is made depending on whether breast conservation surgery is possible, USG guided fiducial marker or clip may be placed within the lesion before start of neoadjuvant chemotherapy (NACT). Post NACT response assessment of such lesions is once again done with sonomammography and operative intervention is done after that. Imaging guided wire localisation of the previously placed fiducial marker / lesion is usually done on the day of surgery to aid in resection of the tumor. Magnetic resonance imaging (MRI) of breast is usually done with aid of contrast enhancement (gadolinium based dye) and dynamic study is preferred. MRI is indicated for special cases as follows as per American College of Radiology (ACR) guidelines as discussed in detail above. Novel methods of breast imaging such as 3D Tomosynthesis (combined with 2D mammography which is available at our center) and contrast enhanced mammography are also available for use in some advanced oncology setups however the widespread use of these techniques is limited as of now due to logistics issues.
Breast imaging has undergone much evolution since the early years of mammography. Screening mammography is contributing to the substantial decrease in breast cancer mortality through early detection. Screening mammography programs allow depiction of nonpalpable, suspicious findings requiring histologic evaluation. Widespread acceptance of percutaneous breast biopsy techniques represents the most important practice-changing development in breast imaging alongside newer techniques like VABB, tumor marker placement, wire localization as well as RFA / MWA. The radiologist now plays a vital role not only in the detection and evaluation of breast disease, but also in the diagnosis and management of breast cancer.
References
-
Nagwa D (2020) Mammography in Breast Cancer. Drugs & Diseases Radiology.
-
Tari DU, Pinto F (2023) Mammography in Breast Disease Screening and Diagnosis. J Pers Med 13(2): 228.
-
Freer PE (2015) Mammographic breast density: Impact on breast cancer risk and implications for screening. RadioGraphics 35(2): 302-315.
-
Spaka DA, Plaxco JS, Santiago L, Drydenb MJ (2017) ACR BIRADS atlas 5th edition: Diagnostic and Interventional Imaging 98(3): 179-190.
-
Dedy H, Naufal NF (2022) Role of Breast Imaging in Pre- and Post-Definitive Treatment of Breast Cancer. Breast Cancer.
-
Houssami N (2015) Digital breast tomosynthesis (3D-mammography) screening: Data and implications for population screening. Expert Rev Med Devices 12(4): 377-379.
-
Skaane P (2022) Contrast-enhanced mammography for screening recalls: A problem-solving assessment tool ready for use? Eur Radiol 32(11): 7386-7387.
-
Kathryn M, Dawood T (2024) Breast Ultrasound. In: StatPearls. StatPearls Publishing, University of Pretoria Brooke Army Medical Center, USA.
-
Gokhale S (2009) Ultrasound characterization of breast masses. Indian J Radiol Imaging 19(3): 242-247.
-
Mendelson EB, Berg WA, Gordon PB (2019) Benefits of Supplemental Ultrasonography with Mammography. JAMA Intern Med 179(8): 1150.
-
Evans A, Trimboli RM, Alexandra A, Corinne B, Pascal AB, et al. (2018) Breast ultrasound: recommendations for information to women and referring physicians by the European Society of Breast Imaging. Insights Imaging 9(4): 449-461.
-
Flory V, Levy G, Julien V, Renaud S, Laura E, et al. (2020) [Preoperative breast imaging review: Interests and limits of specialized validation in oncology]. Bull Cancer 107(3): 295-307.
-
Selvi R, S Agarwal, Purvish MP, K Kaur, Shikha P, et al. (2018) Role of magnetic resonance imaging in breast cancer management. South Asian J Cancer 7(2): 69-71.
-
Houssami N, Turner RM, Morrow M (2017) Meta- analysis of pre-operative magnetic resonance imaging (MRI) and surgical treatment for breast cancer. Breast Cancer Res Treat 165(2): 273-283.
-
Thibault F, Nos C, Meunier M, El Khoury C, Ollivier L, et al. (2004) MRI for surgical planning in patients with breast cancer who undergo preoperative chemotherapy. AJR Am J Roentgenol 183(4): 1159-1168.
-
Martincich L, Montemurro F, De Rosa G, Marra V, Ponzone R, et al. (2004) Monitoring response to primary chemotherapy in breast cancer using dynamic contrast- enhanced magnetic resonance imaging. Breast Cancer Res Treat 83(1): 67-76.
-
Ekta D, Rashmi S, Seema M, Smriti H (2021) Image- Guided Breast Interventions: Biopsy and Beyond. Indian J Radiol Imaging 31(2): 391-399.
-
Mary CM, Mary SN (2013) Breast intervention: how I do it. Radiology 268(1): 12-24.
-
Therese B, Bethany L, Jennifer L, Debbie L, Ermelinda B, et al. (2023) NCCN guidelines for Breast Cancer. J Natl Compr Canc Netw 21(9): 900-909.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage