Meningoencephalitis-Neuroimaging in the Era of Polymerase Chain Reaction Based Testing
The Polymerase chain reaction (PCR) test in cerebrospinal fluid (CSF) has proven to have great impact in patient management. It is the fastest test system that allows better assessment of a broad range of infectious agents associated with central nervous system infection. We attempt to describe imaging features of some of these organisms with the hope that in future Neuroimaging can also be used as a non-invasive tool to identify agents.
Introduction
Infections of the central nervous system (CNS) pose significant health risks globally, especially in cases of immunocompromised individuals and the rising incidence of HIV infection exacerbates this issue [1]. While effective antimicrobial treatments are now available, early detection is crucial. Unlike other CNS disorders, invasive tissue diagnosis is challenging, making non-invasive imaging vital for prompt identification. Magnetic resonance imaging (MRI) is the primary imaging tool for CNS disorders, but pinpointing the exact cause based on conventional MRI with Gadolinium enhancement is often difficult due to overlapping features [2]. However, advancements in MRI techniques, such as molecular and functional imaging, provide radiologists with better diagnostic capabilities. This review aims to offer a systematic MRI approach to streamline differential diagnoses, classify, and characterize CNS infections. Here is a few imaging appearances of different infectious agents:
Bacterial
E-Coli: Uncommon in adults-presents with multiple abscesses and ventriculitis [3].
Haemophilus Influenza: Cerebral edema, hemorrhage, or bilateral thalamic lesions, and these neuroimaging abnormalities are associated with poor prognosis Mild encephalopathy patients were also diagnosed with reversible corpus callosum lesion (MERS). Kimura, et al. divided influenza related brain lesions into 5 categories normal (category 1); diffuse involvement of cerebral cortex (category 2); diffuse brain edema (category 3); symmetrical involvement of the thalamus (category 4); and focal encephalitis (category 5) [4].
Listeria Monocytogenes: Mostly rhombencephalitis-rarely ventriculitis [5] (Figures 1 & 2).
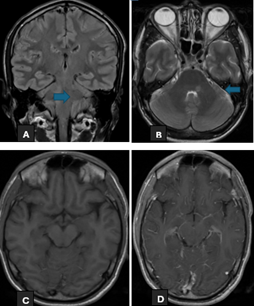
Figure 1: A 38 years old gentleman presented with persistent headache. On examination he had positive signs of miningism. MRI head (Figure A+B) show vertical hyperintense focus involving posterior left hemi-pons on T2 and FLAIR sequences. (Figure C+D) show leptomeningeal enhancement. Patient underwent lumbar puncture; CSF Detailed Report was highly suggestive of infection. Bio-Fire meningitis panel was sent and it detected Listeria Monocytogenes.
Neisseria Meningitides: An ependymal inflammation is mostly seen [6].
Streptococcus Agalactiae: Tiny hyperintensities in the subarachnoid space (ventricles and brain parenchyma. Sometimes with cerebellar abnormalities [7].
Streptococcus Pneumonia: Can resemble ischemic areas but changes are bilateral and are associated with ring enhancement. Supratentorial leptomeningeal enhancement also common [8].
Viruses
CMV Encephalitis: Mostly only non-specific bright T2/ FLAIR signal in the white matter. If ventriculitis is present then enhancement of the ependymal lining surface and hydrocephalus may be seen. High T2 white matter change most prominent in a periventricular distribution. • No enhancement (unless ventriculitis present, in which case 30% or so will enhance).
• No mass effect (often seen with concurrent atrophy) [9].
Enterovirus (EV): The enteroviruses include Coxsackie viruses A and B, poliovirus, echoviruses, and enteroviruses 68 to 71. They may cause hand, foot, mouth disease (Coxsackie virus A16, EV 71) A (3), herpangina (EV 71), hemorrhagic conjunctivitis (enterovirus 70, Coxsackie virus A24)Â (4), poliomyelitis (poliovirus), polio-like paralysis, or radiculomyelitis (EV 70, EV 71, Coxsackie virus A7, A24).
Herpes Simplex Virus 1 (HSV-1): In the immunocompetent adult patient, the pattern is quite typical and manifests as bilateral asymmetrical involvement of medial temporal lobes, insula, and inferolateral frontal lobes. The basal ganglia are typically spared, helping to distinguish it from a middle cerebral artery infarct. Extra limbic involvement is more prevalent in children than in adults. In immunocompromised patients, involvement can be more diffuse and more likely to involve the brainstem [10] (Figure 3).
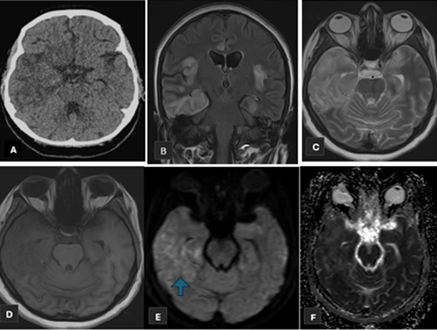
Figure 3: A 43 years old female with no known comorbids presented to ED with complaints of Headache, altered behavior and fever for the last 10 days. (Figure A) non-enhanced CT head shows low attenuation areas in bilateral temporal lobes, more on right side. MRI head (Figure B+C) show hyperintense signals on T2 and FLAIR sequences with corresponding hypointense signals on T1 sequence (Figure D) in bilateral temporal lobes and insular fissure. (Figure E+F) show patchy areas of different restriction. She underwent lumbar puncture and CSF DR showed predominant lymphocytic picture hence CSF HSV PCR was sent which showed HSV 1.
Herpes Simplex Virus 2 (HSV-2): Neuroradiologic manifestations of HSV-2 infection are much less uniform with immunocompetent patients showing mild edema in a similar distribution to HSV-1 infection. However, MRI changes in immunocompromised patients are inconsistent and may be more extensive, atypical or even entirely absent.
Human Herpes Virus 6 (HHV-6): Is a rare CNS infection due to human herpes virus 6 reactivation in immunosuppressed patients, with MRI signal intensity abnormalities of the medial temporal lobe [11].
Human Parechovirus (HPeV): HPeV infection is an
increasingly recognized cause of neonatal sepsis or Meningoencephalitis, often presenting with seizures, and MR imaging is an essential component of the clinical evaluation of seizures in neonates. DWI shows low diffusivity of the Supratentorial white matter with front parietal predominance, and involvement of the corpus callosum, thalami and sparing of, brain stem, basal ganglia and cerebellum [12].
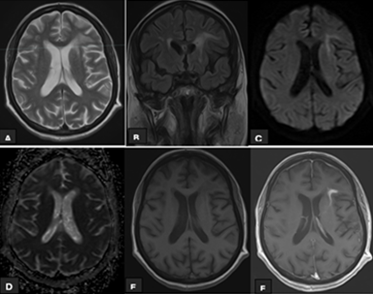
Varicella Zoster Virus (VZV): Vasculitis induced presentations include encephalitis, myelitis, ataxia, Reye syndrome, and Ramsay-Hunt syndrome [13] (Figure 4).
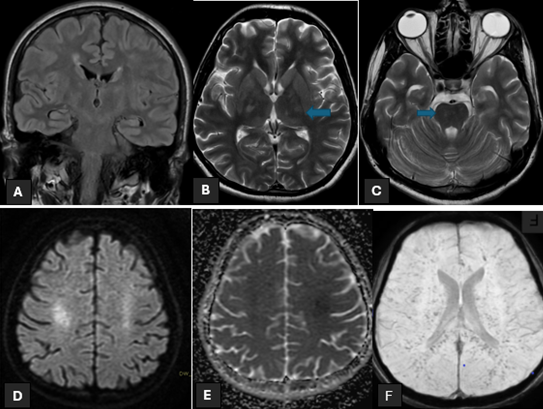
Figure 4: A 22 years old gentleman with no known comorbids presented to ED with history of fever and skin rash for 5days and acute loss of consciousness. MRI head (Figure A+B+C) show hyperintense signals in Bilateral Thalami And Brain Stem on T2 and FLAIR sequences. (Figure D+E) show diffusion restriction in bilateral centrum semiovale. (Figure F) shows micro hemorrhages in bilateral cerebral hemispheres. The patient underwent lumbar puncture and CSF DR showed predominant lymphocytic picture. Bio-Fire film array detected Varicella Zoster Virus.
Fungal
Cryptococcus Neoformans/Aatti: Four basic Manifestations: diffuse meningeal disease (more common), focal or multiple parenchymal lesions (common), disseminated nonfocal disease of the parenchyma (rare), focal lesion with dural base (rare) [14, 15] (Figure 5).
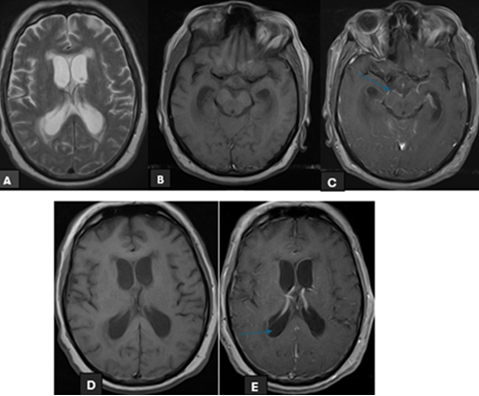
Figure 5: A 68 years old male known hypertensive presented to ED with complaints of headache and drowsiness. MRI head (Figure A) shows hydrocephalus with periventricular seepage. (Figure B+C) show marked Basilar meningeal enhancement. Marked by arrow (Figure C+D) show enhancement of ependymal lining marked by arrow. Patient’s lumbar puncture was done showed infective picture. Bio-Fire film array detected Cryptococcus neoformans.
Conclusion
The imaging characteristics of CNS infections present a complex array of features. Classifying them based on conventional MRI sequences can offer an initial guide to narrowing down the potential diagnoses. Further refinement into specific etiologies can then be achieved using advanced MRI sequences and techniques.
References
-
Aiken AH (2010) Central nervous system infection. Neuroimaging Clin N Am 20(4): 557-580.
-
Whiteman ML, Bowen BC, Post MJ, Bell MD (2002) Intracranial infections. In: Scott WA (Ed.), Magnetic Resonance Imaging of Brain and Spine. 3rd (Edn.), Lippincott Williams and Wilkins, Philadelphia, pp: 1099- 1177.
-
Toh CH, Wei KC, Chang CN, Hsu PW, Wong HF, et al. (2012) Differentiation of pyogenic brain abscesses from necrotic glioblastomas with use of susceptibility- weighted imaging. AJNR Am J Neuroradiol 33(8): 1534- 1538.
-
Desprechins B, Stadnik T, Koerts G, Shabana W, Breucq C, et al. (1999) Use of diffusion-weighted MR imaging in differential diagnosis between intracerebral necrotic tumors and cerebral abscesses. AJNR Am J Neuroradiol 20(7): 1252-1257.
-
Luthra G, Parihar A, Nath K, Jaiswal S, Prasad KN, et al. (2007) Comparative evaluation of fungal, tubercular, and pyogenic brain abscesses with conventional and diffusion MR imaging and proton MR spectroscopy. AJNR Am J Neuroradiol 28(7): 1332-1338.
-
Gaviani P, Schwartz RB, Hedley WET, Ligon KL, Robicsek A, et al. (2005) Diffusion-weighted imaging of fungal cerebral infection. AJNR Am J Neuroradiol 26(5): 1115- 1121.
-
Lai PH, Ho JT, Chen WL, Hsu SS, Wang JS, et al. (2002) Brain abscess and necrotic brain tumor: discrimination with proton MR spectroscopy and diffusion-weighted imaging. AJNR Am J Neuroradiol 23(8): 1369-1377.
-
Gupta RK, Roy R, Dev R, Husain M, Poptani H, et al. (1996) Finger printing of Mycobacterium tuberculosis in patients with intracranial tuberculomas by using in vivo, ex vivo, and in vitro magnetic resonance spectroscopy. Magn Reson Med 36(6): 829-833.
-
Lai PH, Weng HH, Chen CY, Hsu SS, Ding S, et al. (2008) In vivo differentiation of aerobic brain abscesses and necrotic glioblastomas multiforme using proton MR spectroscopic imaging. AJNR Am J Neuroradiol 29(8): 1511-1518.
-
Trivedi R, Saksena S, Gupta RK (2009) Magnetic resonance imaging in central nervous system tuberculosis. Indian J Radiol Imaging 19(4): 256-265.
-
Jain KK, Mittal SK, Kumar S, Gupta RK (2007) Imaging features of central nervous system fungal infections. Neurol India 55(3): 241-250.
-
Smith AB, Smirniotopoulos JG, Rushing EJ (2008) From the archives of the AFIP central nervous system infections associated with human immunodeficiency virus infection radiologic-pathologic correlation. Radiographics 28(7): 2033-2058.
-
Lee GT, Antelo F, Mlikotic AA (2009) Best cases from the AFIP cerebral toxoplasmosis. Radiographics 29(4): 1200-1205.
-
Ho TL, Lee HJ, Lee KW, Chen WL (2005) Diffusion- weighted and conventional magnetic resonance imaging in cerebral cryptococcoma. Acta Radiol 46(4): 411-414.
-
Trenkwalder P, Trenkwalder C, Feiden W, Vogl TJ, Einhaupl KM, et al. (1992) Toxoplasmosis with early intracerebral hemorrhage in a patient with the acquired immunodeficiency syndrome. Neurology 42(2): 436- 438.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage