The Effect of Behavior Change Communication via the Health Development Army on Pregnant Women’s Nutrition and Health Practices in Ambo District, Ethiopia: A Cluster Randomized Controlled Community Trial
Background: A woman’s nutrition and health at conception and during her pregnancy is crucial factors in defining both her own and her unborn child’s health and well-being at this crucial time in her life. Therefore, the objective of the study was to investigate the effect of Behavior Change and Communication (BCC) through the women development Army on optimal nutrition and health practices of pregnant women. Methods: From April 1, 2018 to October 30, 2019, a cluster-randomized controlled trial was conducted in the Ambo district of Ethiopia. Three hundred eighty-five women in the 24 intervention clusters and 385 women in the 24 control clusters were recruited at the start of the study. In the intervention group, health development armies delivered the BCC’s main messages for three months, from July 2018 to September 2018, and end point data were collected from pregnant women (n = 744, 372 in the intervention group, and 372 in the control group) in October 2018. The control group received the standard care provided by the healthcare system during an ANC visit. The researchers used a binary generalized linear model analysis. A p value of <0.05 is used to indicate statistical significance. Statistical analyses were conducted on a per protocol basis. Result: The overall optimal nutrition and health practice were higher in the intervention group than in the control group (62.6% vs. 38.7%, P<0.001). The control group had a larger absolute risk of suboptimal nutrition and health practice (0.613 vs. 0.374, p<0.001) than the intervention group. Pregnant women in the intervention group had an absolute risk difference of 23.9% for suboptimal nutrition and health. Pregnant women who received intervention were 30.9% less likely to have suboptimal nutrition and health practice compared to pregnant women who were in the control group (ARR=0.691, 95% CI: 0.594-0.804). Conclusions: Behavior change communication (BCC) through the women’s development army is effective in improving optimal nutrition and health practices of pregnant women. Therefore, to improve the optimal nutrition and health practices of pregnant women, BCC through the health development army is recommended.
Abbreviations
ANC: Antenatal Care; AOR: Adjusted Odd Ratio; BCC: Behavior Change Communication; CI: Confidence Interval; CONSORT: Consolidated Standards of Reporting Trials; COR: Crude Odd Ratio; CRCCT: Cluster Randomized Controlled Community Trial; EDHS: Ethiopian Demographic and Health Survey; ENA: Essential Nutrition Action; HAD: Health Development Army; HEW: Health Extension Worker; IYCF: Infant and Young Child feeding Practice.
Background
Nutrition throughout life has a major effect on health. Mother’s nutritional and health status at conception and throughout pregnancy plays a key role in determining her health and well-being, as well as that of her child [1]. According to Essential Nutrition Actions (ENA) framework, optimal nutrition and health practice of pregnant women encompasses optimal quantity and quality of diet; essential micronutrient intake; diseases prevention and treatment practices and supportive life style and care [2, 3, 4].
Behavior change communication (BCC) is widely recognized as one of the main health promotion strategies. It is an interactive process of working with individuals and communities to develop communication strategies to promote positive behaviors as well as create a supportive environment to enable them to adopt and sustain positive behaviors [5, 6].
Suboptimal diet that comprises inadequate intake of calories and other nutrients, combined with a heavy maternal workload, impacts adversely on the health of the mother, the developing foetus and the newborn [7]. Pregnant women need at least one extra meal a day than usual, along with plenty of safe water. Consumption of iron-rich foods and iodized salt is also important [4].
Naturally, the urge to eat more is experienced by nearly all pregnant women [8]. Weight gain is a normal process during pregnancy. On average, a woman should gain about 12.5 kg during pregnancy. Many women gain barely half this amount because of poor diets and heavy workloads [4].
Malaria prevention and treatment, deworming treatment, sanitation facilities and practices are very important aspects of nutrition and health practices during pregnancy [2, 4]. Minimizing a heavy work load and reducing work hours enables energy-deficient women to reduce their energy expenditure. If a pregnant woman does not reduce her work load or gets enough rest during her pregnancy, her nutrient stores may be depleted [3, 4].
Women’s status and women’s education play pivotal roles in improving nutrition. In addition to benefiting their nutrition and health status, greater education among women paves the way to greater productivity, empowerment, and control of resources, allowing them to make better choices that ultimately benefit the health and nutrition of children and families [9, 10]. In some cultures, because of their status, women are less able to access resources and make decisions to improve their health and nutrition [11].
Studies were done in Ethiopia on dietary knowledge and practice and the nutritional status of pregnant women. According to the institution-based study done in Mettu Karl Hospital, Southwest Ethiopia, among pregnant women the prevalence of sub-optimal dietary practices was 22% [12]. According to the study done in Gedeo zone, southern Ethiopia, in 2018, around one-third (67.8%) of pregnant women had poor dietary practices [13].
Different researchers show socio-demographic factors like age, wealth index, residence, size of farmland, illiteracy or low education are common factors affecting maternal nutrition and health status and, similarly, maternal and health service related factors like years at marriage, ANC visits, level of nutritional knowledge and food practices (consuming additional food during pregnancy and a variety of food from both animal and plant origins) are common factors affecting the nutrition and health practices of pregnant women [14, 15, 16, 17].
Nutritional and health education interventions for pregnant women were found to be beneficial in improving their dietary habits [18]. However, normal nutrition and health education provided by health professionals in health care facilities in Ethiopia was difficult for pregnant women to understand and was inconsistent. As a result, dietary and health outcomes remain a major public health issue in Ethiopia [19].
This study used health development armies to communicate behavior change as an implementer of the intervention. Health Development Armies are volunteers, have significant potential to improve access to Primary Health Care (PHC) in Ethiopia, and support the work of the Health Extension Workers (HEWs) [20] and there is an impressive improvement in maternal and child health and service use after the introduction of HDA in the country [21, 22, 23]. However, to the best of the researcher’s knowledge, no evidence was found on BCC interventions delivered through HDA whether to improve the nutritional status of pregnant women.
One of the most well-known health promotion tools is behavior change communication (BCC). It is a collaborative approach that involves working with individuals and groups to develop communication methods to encourage positive behaviors and to build a supportive atmosphere in which they may adopt and maintain those behaviors [5, 6].
In Ethiopia, data on the effect of BCC on the nutrition and health practices of pregnant women were scarce. To the best of our knowledge, no research has been done on the effect of BCC through the health development army on pregnant women’s nutritional and health practices. As a result, the objective of this study was to assess the effect of BCC through the health development army on the optimal nutritional and health practices of pregnant women in Ambo district. The results of the study could be an input to policymakers and planners at the national and regional level to nutrition and health practices of pregnant women.
Research Hypothesis
H0: Behavior change communication through the health development army has no effect on nutrition and health practices of pregnant women. H1: Behavior change communication through the health development army has a positive effect on nutrition and health practices of pregnant women.
Methods and Materials
Study Design, Study Period and Setting
A cluster randomized controlled community trial (CRCCT) with baseline and endline measurement was conducted from June 2018 to October 2018 among pregnant women in the Ambo district of West Shoa Zone, Ethiopia. Ambo district is located in the western part of Ethiopia, 114 km from Addis Ababa, the capital of Ethiopia. Based on 2017 district health office data, it has 37,454 and 6976 reproductive age group and pregnant women, respectively [24].
Sample Size Determination and Study Population
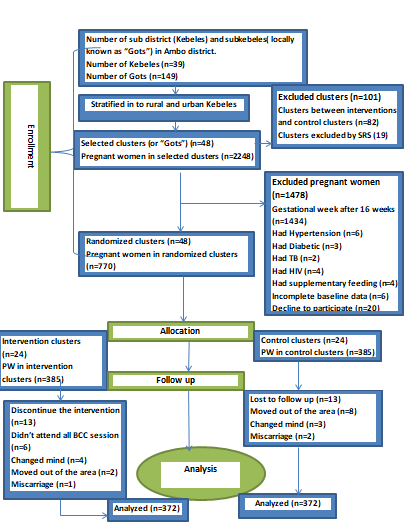
The sample size was calculated using G power 3.1.9.2 program with a power of 80% for Fisher’s exact test and precision of 5%. According to Fekadu B, et al. [25] the proportion of optimal dietary practice among pregnant women (p1) 0.34 was used, effect size (h) of 0.3 and with the allocation ratio case to control (N2/N1) of 1, Proportion (p2) 0.65 was calculated, and with the allocation ratio of intervention to control group (N2/N1) of 1. The calculated sample size was multiplied by design effect of 1.5 due to cluster sampling. Considering a 10% loss to follow up, the final sample size was 770 pregnant women (385 of controls and 385 of interventions group). Due to problems reported in Figure 1, the actual data were collected from 372 women in the intervention group and 372 women in the control group. The study population was pregnant women aged 18–49 years, before 16 weeks of gestation, and permanent residents (who lived in the study area for more than six months) of the Ambo district. Pregnant women with chronic diseases such as hypertension, diabetes, tuberculosis, and HIV/AIDS, those with incomplete baseline data, and those enrolled in supplementary feeding programs were excluded from the study, as these interventions would have an impact on nutritional status and thus bias the results of the study.
Recruitment, Randomization and Intervention Allocation
Recruitment of Participants
A multi-stage sampling technique was used to select study participants. The total number of kebeles (sub districts) in the district was stratified into rural and urban areas. Simple random sampling (SRS) with the lottery method was used to select 12 kebeles (2 urban and 10 rural) from the existing 39 kebeles (6 urban and 33 rural). Each kebele has its own sub kebeles or clusters (locally known as “Gots”), which have been pre-determined by government bodies and are grouped into 149 distinct clusters. The number of clusters in each kebele was then recorded. Forty-eight clusters were selected at random from the entire number of clusters available in the district, including non-adjacent clusters and those that were somewhat far apart from one another. Lists were established to include these clusters in the study. As a result, each arm of this study had 24 clusters. We left at least one cluster between each cluster that was used in our research as a buffer zone. We used a proportionate stratified sampling technique to obtain clusters from each kebele. Using the block randomization technique, we randomly assign the chosen clusters into intervention and control groups, as described in more detail below. Eligible pregnant women were screened utilizing a family folder prepared by the kebele’s health extension workers (HEWs), as well as by inquiring about the first date of their last menstrual cycle and confirming pregnancy using a pregnancy test. Then, were employed simple random sampling technique to select study participants from each cluster for each arm. Equal numbers of participants were selected from each cluster. Health extension workers and data collectors visited a group of selected women at each arm at their residence. Women who agreed to take part in the study were asked to sign an informed consent form to confirm their voluntary involvement. Each subject was interviewed after receiving consent.
Randomization
Random Selection of Clusters
The clusters (locally known as “Gots”) were the units of randomization in our study. We stratified the subdistricts (or kebeles, i.e., urban vs. rural kebeles) before randomization and produced a separate list of kebeles in alphabetical order. The stratification technique was used to distribute any known and unknown confounders at the kebele level equally among the study arms. A unique code was provided to each kebele. As was already mentioned, thirty-nine sub-districts make up the Ambo district. Using simple random sampling (SRS) with the lottery method, we selected 12 kebeles. Each kebele has sub kebeles (or clusters, often known as “Gots”). We used the proportionate stratified sampling method to obtain clusters from each of the 12 kebeles proportionately (48/149) to their population size. A unique cluster code was given to each cluster. The 48 clusters were then divided into two blocks of size 4 in accordance with their alphabetical order by the author. The author randomly selected the randomization sequence of clusters for each block using the sealed lots of the six possible permutations within the block. Each block’s clusters were randomly assigned to the intervention and control arms in the order indicated by the block’s chosen permutation for the stratum. In order to preserve a 1:1 random allocation ratio, we created 24 clusters for the intervention arm and another 24 clusters for the control arm. Actual and potential confounding factors were distributed equally across the study arms due to the stratification and randomization approaches, which ultimately ensured the comparability of the arms. Pregnant women who met the inclusion criteria were enrolled in the same arm in one cluster (either in the intervention or control arms). There were about 12–17 pregnant women in each cluster. Between the intervention and control clusters, buffer zones (non-selected clusters) were also left to reduce information contamination. Health Extension Workers recruited, enrolled, and assigned individuals to interventions after the author randomized the clusters.
Thirteen people from the intervention and thirteen from the control groups were removed from the study for reasons such as discontinuing the intervention and being lost to follow-up. The study was completed with 744 people (Figure 1).
Intervention
To continue with the intervention strategy, the researchers enlisted the help of health extension workers to recruit Health Development Armies (HDA). HDA were chosen from clusters that had been designated as intervention groups. Following recruitment, HDA were trained for one week using a protocol developed by the principal investigator for pregnant women based on the Essential Nutrition Action (ENA) framework, a framework for promoting maternal nutrition developed by the Manoff Group for developing countries, and making a balanced plate for pregnant women in Bangladesh [3, 4, 26]. The ENA framework was recommended by the World Health Organization (WHO) for developing countries and promotes a “nutrition through the life cycle” approach, addressing seven packages, but the authors’ focus was on one package, which was on maternal nutrition during pregnancy. A framework for promoting maternal nutrition developed by the Manoff group for developing countries reflect the benchmarks related to diet and micronutrients, disease prevention and treatment, and lifestyle factors against which maternal nutrition programs can be developed and monitored. Making a balanced plate for pregnant women in Bangladesh was a study protocol which follows practical demonstration (that is) exhibiting the meal preparation in front of the pregnant women. For this, participant women will be encouraged to share food from their own kitchen. Sharing food between participants is possible and culturally acceptable, so Authors adapted this Bangladesh study protocol approach to its study area and participants; it was further explained in the intervention protocol (Supplemental file S1). So, our intervention includes. Both theoretical and practical demonstrations were included in the training, HDA followed the criteria (based on the protocol) to assure the intervention’s adoption. A training handbook, role-playing, participatory meal preparation, and mock BCC sessions were used to deliver HDA training to a group.
To reduce variability among HDA, the researchers established a key assessment question (checklist) (incorporating both theory and skill). The health development army’s knowledge and skills were assessed before and after training, as well as through practical evaluations. After the training, the authors conducted standardization tests to ensure that everyone was on a similar level. Furthermore, the researchers and supervisors actively monitored HDAs during the pretest and during the intervention to see if they were delivering the intended message according to the intervention protocol. Those who failed to communicate the health and nutrition BCC message were identified and prompt corrective action was taken.
The intervention for pregnant women took place in the community’s intervention clusters. However, the exact location of the BCC training was determined by agreement between the pregnant women and the HDA (and so that they have traveled to a common site, but not out of the intervention clusters).The intervention was conducted once every two weeks for 1:00 up to 1:30 hour length on nonworking days; similarly, the researchers monitored the intervention activities every two weeks, and the intervention lasted three months. The typical cluster size was 12-17 pregnant women; therefore one HDA was in charge of each cluster.
The main components of the intervention were adapted from the recommendations of ENA, a framework for promoting maternal nutrition developed by the Manoff group for developing countries, and making a balanced plate for pregnant women in Bangladesh as described above. The core content of the intervention includes the following nutrition and health practice messages: on eating additional foods during pregnancy (increase meal frequency and portion size with gestational age); eating a variety (diversified) of foods from vegetable, fruit, and animal sources; utilization of iodized salt; appropriate timing and storage of iodized salt; decrease consumption of iron-inhibiting foods, such as tea and/or coffee, with meals; decrease alcohol consumption; not avoiding important foods during pregnancy (associated with taboos); importance of taking iron/folate during pregnancy for at least three months; sleep under an insecticide-treated bed net; seek treatment from health institution if developed illness; keep a clean environment, wash hands with soap during critical moments; keep food and food containers clean; drink only treated water (if out of pipe water); reducing heavy workload; taking day rest; improving self-decision making in food and her own health, importance of obtaining support from the family/community during pregnancy and utilization of health care services (Antenatal care (ANC) follow up, plan to deliver at health institution, and plan to have Post Natal Care (PNC) follow up) and birth preparedness and complication readiness. Similarly, at each BCC session, the consequences of not using the above message were discussed. During each BCC session, participants’ knowledge and attitudes about good nutrition and health were also assessed. Then, depending on the detected gaps, a BCC letter was sent out.
A message about food intake centered on locally available, acceptable, and affordable foods. In addition to delivering BCC messages, HDAs were provided posters and brochures with relevant images to display to pregnant women. Pregnant women were given leaflets with key messages written in Afan Oromo and Amharic (local) languages with illustrations. If a woman couldn’t read, it was suggested that she have the leaflet read to her by someone at home or in the community who could. Because the selected HDA were educated (at least read and write), they received written teaching aid; they had a schedule and topics to address in each contact (Supplemental file S1). Each pregnant woman in the intervention group had attended six BCC sessions on nutrition and health.
Meal preparation, exhibiting samples of iron/folate tablets, type and time of adding iodized salt while cooking, how to use an insecticide-treated bed net, and personal and food cleanliness were all covered in a practical demonstration. Participants were urged to share food from their own kitchens (home) to demonstrate meal preparation. Based on this visual display, pregnant women actively identified the food groups and preparation methods they should change.
Pregnant women in the control groups did not receive the intervention but were instead exposed to the typical care provided by the healthcare system during an ANC visit and any intervention at the community level by health extension workers. Women in the control group received nutrition education during their ANC visits, though it may not have been as thorough as other care like diagnose and treat diseases or complications. This service was available to pregnant women in both the control and intervention groups. They were monitored for the same duration of the intervention and given the same evaluations as the intervention group.
From April 1 to June 1, 2018, baseline data on first- trimester pregnant women were collected. All pregnant women who were classified as intervention groups began receiving the intervention on July 1, 2018. The intervention was given over three months, from July 01, 2018 to September 30, 2018.
Blinding
Allocation concealment is not possible due to the nature of the intervention. The participants, as well as the HDA, are aware of the intervention. However, the participants, HDAs, and data collectors were blinded to the study hypothesis. The field supervisors were blinded to the outcome of interest and, finally, we blinded the data collectors for the intervention. Furthermore, the data entry clerk was blinded by coding the groups.
Data Collection Tools and Procedures
Data were collected using a pre-tested and semi- structured questionnaire written in English. To maintain consistency, the questionnaire was translated into two languages (Afan Oromo and Amharic) and then back to English by language experts to keep its consistency. The questionnaire was pretested in Ginchi town, which is nearby to Ambo district, on 39(5%) of the total sample size to identify any ambiguity, length, completeness, consistency, and acceptability of the questionnaire, and some skip patterns were corrected before the real data collection.
Eight diploma nurses were recruited to collect data. Training was given to the data collectors on the objective and relevance of the study; confidentiality of information; respondent’s rights; informed consent; and techniques of interview. The filled questionnaires were checked for consistency and completeness daily by four supervisors who had BSc degrees in Nursing and principal investigators on the spot. Parts one and two of the questionnaire cover socio- demographic and maternal characteristics; part three covers maternal characteristics; part four covers nutritional status; and part five covers birth outcomes such as live or dead, place of delivery, and birth weight. At the baseline, data on sociodemographic, economic, and maternal characteristics were collected. Before and after the trial, data on nutrition and health knowledge, attitude, and practice were obtained, as well as mid-upper arm circumferences.
The household wealth index was assessed using wealth constructs covering household assets, utilities, and agricultural land ownership adopted from the Ethiopian Demographic and Health Survey [23]. The latent factors describing the wealth data were generated using principle components analysis (PCA) and then grouped into wealth terials.
Women’s decision-making power was assessed using eight questions. When a choice was made by the woman alone or jointly with her husband, code one was assigned to each question; otherwise, code zero was assigned to each question. The mean was used to categorize a woman’s ability to make decisions [23].
Food security status was assessed using 27 previously validated questions [27]. A household that experienced less than the first 2, 2–10, 11–17, and > 17 food insecurity indicators was considered food secure, mildly, moderately, and severely food insecure households, respectively.
Questions related to Knowledge, Attitude and practices was adapted from essential nutrition action frame work and the formative research done by the Manoff group to promote maternal nutrition in developing countries [3, 4, 15].
Knowledge of pregnant women about nutrition and health practices was assessed by using 14 questions that were used to assess knowledge of pregnant women regarding optimal nutrition and health. A knowledge score was calculated for each participant based on the number of questions that were correctly answered in the knowledge assessment questions. Each correct response was scored 1, and each incorrect response scored 0. The factor scores were summed and ranked into terciles (three parts). A pregnant woman was considered to have poor knowledge about nutrition and health if she scored below the highest tertile (i.e., in the first and/or second tertile) and good knowledge about nutrition and health if she scored in the highest tertile (third tertile) [28].
Attitude towards nutrition and health practice was assessed by 20 Likert scale questions using PCA. The factor scores were summed and ranked into terciles (three parts). Then the highest tercile was labeled as a favorable attitude, if not unfavorable attitude [28].
The rapid test kit (RTK) was used to determine if the salt used was iodized or not. The interviewer asks each pregnant woman to provide a teaspoon of salt used for food preparation and fill a small cup spread flat, then add two drops of test solution to the surface of the salt by piercing the white ampule, compare the color of the salt to a standard color chart, and determine the iodine concentration. Finally, salt with > 15 parts per million (ppm) was classified as adequately iodized salt, while salt with 15 ppm was classified as inadequately iodized [29, 30].
The outcome variable nutrition and health practice was measured using questions of practice about the dietary quantity, dietary quality, micronutrient intake, disease prevention and treatment and supportive life style and care. The respondents had asked to choose Yes=1 or No=0 answers by indicating whether each practice of nutrition and health were practiced or not. One point was allocated to a correct response for each questions and zero for incorrect response. The factor scores were summed and ranked into terciles (three parts). Pregnant woman was considered to have suboptimal practice about nutrition and health if she scored below the highest tertile (i.e. in the first and/or second tertile) and optimal practice about nutrition and health if she scored in the highest tertile (third tertile) [28].
Data Processing and Analysis
Thirteen pregnant women discontinued the intervention from the intervention group and thirteen lost to follow-up from the control group were excluded from the analysis. Before entering data, data were manually checked for completeness and consistency.Then it was entered into EPI data version 3.1 and exported to SPSS for Windows version 21 for cleaning and analysis. The effect of intervention was measured at the endpoint of follow up.
First, descriptive statistics like mean and Standard Deviation was done for continuous variable and frequency and percentage for categorical data. A chi-square test was performed to compare the baseline characteristics of the intervention and control groups.
The Hosmer-Lemeshow goodness-of-fit statistic is used to assess model goodness of fit. Multicollinearity was checked using Variance Inflation Factors (VIF) at < 8 but the VIF of all variables was less than 2, which means no multicollinearity. Moreover, the interaction of the variables with the intervention at a p-value of < 0.05 was assessed and there was no interaction. Simple logistic regression analysis was performed between nutritional and health practices and associated factors one at a time. Their odds ratios (OR) with 95% confidence intervals (CI) and p-values were obtained. Factors that were significantly associated with nutritional and health practice at a p-value <0.25 in simple logistic regression analysis were entered into multivariable logistic regression analysis. p- Values <0.05 were used to declare statistical significance. Statistical analyses were conducted on an intention-to-treat (ITT) basis, which is appropriate for a cluster randomized design study data analysis.
Data Quality Control
For one week, the health development armies were trained together. Data collectors and supervisors received three days of training as well. Four supervisors with BSc degrees in nursing and investigators supervised the HDA every two weeks. Furthermore, pregnant women in each cluster had the same number and frequency of BCC sessions, and the lengths of contact within each intervention group were similar, resulting in a standardized process. Participants were reminded of the necessity of attending all sessions and acting at home according to the protocol presented to prevent dropout and promote adherence to the intervention and follow-up program. The HDA monitored and recorded adherence to the BCC sessions in a personal training diary (attendance sheet). Pre-testing of the questionnaire was done among 5% (39 pregnant women). Every two weeks, HDAs and their supervisors met to discuss and provide possible remedies to the problems that arose during BCC sessions. The data were collected using a pre-tested questionnaire. Cronbatch’s alpha value of the questionnaire was checked and it was > 0.7 indicating that it is suitable for use in the research domain. The questionnaire was also translated into the most widely spoken languages in the study area (Afan Oromo and Amharic) to aid respondents’ comprehension. The data gathering process was thoroughly monitored by supervisors and the principal investigator. Daily, completed questionnaires were reviewed for completeness, and any missing or incorrect information was updated. Field supervisors randomly evaluated 5% of the data and alerted them to a possible measurement issue [26].
Ethical Consideration
All methods in the study were performed in accordance with relevant institutional, national, and international guidelines. This study is a community trial that was registered with the Pan African Clinical Trial Registry. The date of registration was March 5, 2018. The registry’s unique identification number is (PACTR201805003366358). The results were reported using the CONSORT (Consolidated Standards of Reporting Trials) guidelines (Supplemental file S2). The Jimma University Ethical Review Committee reviewed and approved the study protocol (ref no: RPGC/40724/2016). Permission to conduct the study in the respective kebeles was granted by the Ambo district health office (ref no: ADHO/134/2018). Prior to participation in the study, the nature of the study was clearly disclosed to the study participants in order to gain their written informed consent (fingerprint for those who could not read and write) was secured from the study participants, and all information obtained was kept anonymous. Soft copy data is password protected, while hard copy data is secured with a key and lock to guarantee confidentiality. Personally identifiable information will not be used in any form in the presentation of the findings.
Results
From 770 pregnant women who enrolled in this study, 744(96.6%) (372 in the intervention group and 372 in the control group) were included in the analysis. Thirteen pregnant women discontinued the intervention from the intervention group for the following reasons: six women didn’t attend all BCC sessions, four changed their mind to participate in the intervention, two moved out of the area, and one woman developed a miscarriage. Similarly, thirteen pregnant women lost to follow up from the control group due to the following reasons; like eight women moved out of the area, thres characteristics between the intervention and control groups (p > 0.05) (Table 1).
| Variable | Category | Intervention Group (N1=372) | Control Group (N2=372) | Chi-Square Test, P-Value |
|---|---|---|---|---|
| Number of clusters | 24 | 24 | ||
| Residence | Rural | 296(49.1) | 307(50.9) | 0.303 |
| Urban | 76(53.9) | 65(46.1) | ||
| Religion | Protestant | 153(48.4) | 163(51.6) | 0.228 |
| Orthodox | 169(49.1) | 175(50.9) | ||
| Others | 37(44.0) | 47(56.0) | ||
| Age of the respondent | 18-24 Years | 90 (50.6) | 88(49.4) | 0.560 |
| 25-34 Years | 256(50.0) | 256 (50.0) | ||
| >35 Years | 23 (42.6) | 31 (57.4) | ||
| Respondents’ Occupation | Employed | 19 (47.5) | 21 (52.5) | 0.868 |
| House wives/ Daily laborers | 307 (50.2) | 305 (49.8) | ||
| Merchants | 23 (54.8) | 19 (45.2) | ||
| Farmers | 22 (44.0) | 28 (56.0) | ||
| Women educational status | No formal education | 144 (50.7) | 140 (49.3) | 0.555 |
| 1-4 Grade | 83 (46.9) | 94 (53.1) | ||
| 5-8 Grade | 92 (50.5) | 90 (49.5) | ||
| 9-12 Grade | 40 (54.1) | 34 (45.9) | ||
| Diploma and higher | 10 (37.0) | 17 (63.0) | ||
| Husband educational status | No formal education | 112 (51.6) | 105 (48.4) | 0.680 |
| 1-4 Grade | 72 (51.4) | 68 (48.6) | ||
| 5-8 Grade | 95 (50.5) | 93 (49.5) | ||
| 9-12 Grade | 66 (46.2) | 77 (53.8) | ||
| Diploma and higher | 24 (42.9) | 32 (57.1) | ||
| Household size | 1-3 house hold size | 114 (54.0) | 97 (46.0) | 0.150 |
| 4-5 house hold size | 176 (49.7) | 178 (50.3) | ||
| >5 house hold size | 79 (44.1) | 100(55.9) | ||
| Household wealth tertile | Low | 110 (50.5) | 108 (49.5) | 0.920 |
| Medium | 159 (48.8) | 167 (51.2) | ||
| High | 100 (50.0) | 100 (50.0) | ||
| Household food security status | Unsecured | 151(50.2) | 150(49.8) | 0.976 |
| Secured | 220(49.7) | 223(50.3) | ||
| Estimated time to reach health institution | < 30 minutes | 77(50.0%) | 77 (50.0%) | 0.980 |
| 30-60 minutes | 147 (49.8) | 148 (50.2) | ||
| > 60 minutes | 145 (49.2) | 150 (50.8) | ||
| Parity | <=1 live birth | 109(48.0) | 118(52.0) | 0.659 |
| 2-4 live births | 230(50.9) | 222(49.1) | ||
| >=5 live births | 30(46.2) | 35(53.8) | ||
| Gravidity | <=2 pregnancy | 58(49.6) | 59(50.4) | 0.876 |
| 3-4 pregnancy | 232(50.2) | 230(49.8) | ||
| >=5 pregnancy | 79(47.9) | 86(52.1) |
Table 1: Socio demographic and obstetric characteristics of pregnant women in control and intervention groups at the beginning of
Knowledge, Attitude and Practices on Nutrition and Health
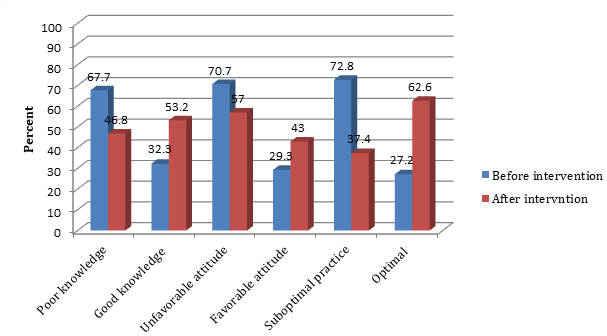
The proportion of pregnant women in the intervention group who had good knowledge, favorable attitudes, and optimal practices about nutrition and health was improved after the intervention (32.3% vs. 53.2%, p 0.001); (29.3% vs. 43.0%, p 0.001); and (27.2% vs. 62.6%, p 0.001), respectively (Figure 2).
The proportion of pregnant women in the control group who had good knowledge and a favorable attitude about nutrition and health at the beginning and endpoints of the study, respectively, was comparable (p = 0.092) and (p =
0.094). However, there was an increase in the proportion of pregnant women with optimal nutrition and health practice at the end of the study (27.7% vs. 38.7%, p<0.001) (Figure 3).
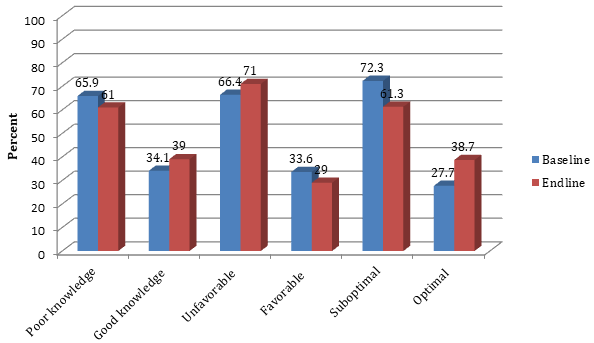
The proportions of participants who had good knowledge, a favorable attitude, optimal nutrition, and health practices were comparable between intervention groups (32.3%, 29.3%, and 27.2%) and control groups (34.1%, 33.6%, and 27.7%) at baseline measurements, respectively. However, at the endpoint of the study period, participants who had good knowledge, a favorable attitude, optimal nutrition and health practices among the intervention group were (53.2%, 43.0%, and 62.6%), while among the control group were (39.0%, 29.0%, and 38.7, p < 0.001), respectively (Table 2).
| Category | Intervention (n1 = 372) N (%) | Control (n2=372) N (%) | p | |
|---|---|---|---|---|
| Knowledge baseline | Poor | 252 (67.7) | 245 (65.9) | 0.586 |
| Knowledge baseline | Good | 120 (32.3) | 127 (34.1) | 0.586 |
| Knowledge endline | Poor | 174 (46.8) | 227 (61.0) | <0.001 |
| Knowledge endline | Good | 198 (53.2) | 145 (39.0) | <0.001 |
| Attitude baseline | Unfavorable | 263 (70.7) | 247 (66.4) | 0.206 |
| Attitude baseline | Favorable | 109 (29.3) | 125 (33.6) | 0.206 |
| Attitude endline | Unfavorable | 212 (57.0) | 264 (71.0) | <0.001 |
| Attitude endline | Favorable | 160 (43.0) | 108 (29.0) | <0.001 |
| Practice baseline | Suboptimal | 271 (72.8) | 269 (72.3) | 0.869 |
| Practice baseline | Optimal | 101 (27.2) | 103 (27.7) | 0.869 |
| Practice endline | Suboptimal | 139 (37.4) | 228 (61.3) | <0.001 |
| Practice endline | Optimal | 233 (62.6) | 144 (38.7) | <0.001 |
Table 2: Nutrition and health Knowledge, Attitude, and Practice between intervention and control group of pregnant women in the A
Quantity of Food
There was no significant difference at base line measurement between the control and intervention groups in the quantity of food-related issues during this pregnancy (p>0.05). However, there was a significant difference in the consumption of additional food during pregnancy (44.1% versus 68.5%, p<0.001) and the absence of food sharing (8.3% versus 27.2%, p<0.0001) at the end of the study as compared to the intervention and control groups, respectively (Table 3).
Quality of Food
There was no significant difference at base line measurement between the control and intervention groups related to the quality of food (p>0.05). However, at the endpoint measurement, a significant increase was seen in the case of consumption of a variety of foods (15.1% VS 29.0%, p<0.001); utilization of iodized salt (18.3% VS 50.8%, p<0.001), appropriate utilization (52.9% VS 86.2%, p<0.001) and appropriate storage of iodized salt (58.8% VS 81.4%, p<0.001). Similarly, there was a significant decrease in avoidance of important foods (because of taboos) during this pregnancy (10.0% VS 26.6%, p<0.001) at endpoint measurements between the control and intervention groups, respectively (Table 3).
Iron/Folate Supplements
There was no significant difference at base line measurement between the control and intervention groups related to micronutrient intake (p>0.05). At the endpoint measurements, a significant difference was observed in iron/folate tablet supplementation at the endpoint measurements (59.9% VS 81.5%, p<0.001) between the control and intervention groups, respectively. However, in this study, there was no significant difference between the control and intervention groups for the duration of iron/ folate supplementation (30.9% VS 34.0%, p=0.622) (Table 3).
Discussion
This trial has documented the effect of BCC through health development army on nutrition and health practices of pregnant women in Ambo District, West Shewa Zone, Ethiopia. The findings of this study confirmed the effectiveness of BCC in improving the nutrition and health practices of pregnant women.
From this study, BCC had a significant effect on optimal nutrition and health practices in the intervention group compared with the control group. Even if it is difficult to compare with a similar target group and topic, this is in line with a cross-sectional study done in the Shabelle zone, Somali region of eastern Ethiopia that found BCC brings change to infant and young child feeding (IYCF) practices. The results confirmed that in order to be effective, BCC needs to be performed using health developmental armies to bridge the gap between knowledge and practice [31]. This suggests that BCC is an important tool to maintain the behavior of pregnant women in improving optimal nutrition and health practices among pregnant women [32]. Similarly, the study done in Indonesia revealed that providing nutrition and reproductive health education improves the practices of pregnant women [33].
Our intervention is also supported by health behavior change communication theory, the ‘Integrative Model of Behavioral Prediction’, which reports a strong intention of a person to perform a behavior, accompanied by the necessary skills and abilities to perform it, and under a conducive environment results in the expected behavior change [34]. This behavior change communication message, other than theoretical aspect it also includes a practical demonstration (visual, interactive and skillful) and since its participatory nature engages the pregnant women involved on preparing a nutritionally diversified and balanced diet, motivated to take iron/folete, follow disease prevention and treatment practices and also a need of support from the family and community. Behavior change communication through health development armies is an affordable; does not require any food supplementation and suitable intervention since conducted at the community level to improve optimal nutrition and health practices of pregnant women and more likely to be sustainable in resource-poor settings including Ethiopia.
The other difference between intervention and control groups regarding the optimal nutrition and health practice of pregnant women might be that the nutrition education delivered by the health care system (i.e., for control) might not be comprehensive enough within the ANC setting due to time management constraints. This is supported by a systematic review on the processes and outcomes of antenatal care that found ANC education sessions were conducted hastily and in less supportive ways due to a lack of time and inadequate skills [35]. Furthermore, we conducted our intervention in their community by grouping pregnant women, which resulted in a more facilitated discourse to promote communication and involvement among the pregnant women.
Even while the proportion of pregnant women in the control groups who had optimal nutrition and health practices at the end of the trial was lower than that of the intervention groups, it increased significantly. This may be because pregnant women who were in the control groups who were followed by ANC can get counseling from health professionals on particular nutrition and health practices [36].
The following components of the intervention were successfully achieved; increasing portion size, frequency, and diversity of meals with increasing gestational age, appropriate utilization of using iodized salt, not avoiding important food (associated with taboos), and taking iron/ folate during pregnancy, follow recommended number of ANC visit, and taking day rest during pregnancy. All of these factors have a substantial impact on pregnant women’s overall nutrition and health practices.
This study revealed that those pregnant women who attended secondary and above education were less likely to be at risk of being suboptimal in nutrition and health practice compared with those with no formal education. This finding is supported by the study done in in Buno Bedele zone, Ethiopia [37] and also supported by the study conducted in America [38] in which women with high level of education had the highest mean and percent of their nutritional knowledge and practice compared to low and moderate educational level.
According to this study, husband education is significantly associated with optimal nutrition and health practices. Those pregnant women whose husbands had secondary and higher education were less likely to be at risk of being suboptimal in nutrition and health practice compared with those with no formal education. This study is congruent with the study done in Dakar, Senegal on factors influencing nutritional practices among mothers, which found that husband education levels were positively correlated with nutritional practices of mothers [39]. Similarly, this finding was consistent with study done in in Gedeo zone, southern Ethiopia on dietary practices and its determinant among pregnant women that revealed respondents husband with formal education were more odds of good dietary practice than those without formal education [13]. This finding implies that a husband’s educational attainment is clearly related to optimal nutrition and health practices of pregnant women.
This finding revealed that pregnant women who travel more than 60 minutes to reach a health institution were more likely to be at risk of being suboptimal in nutrition and health practice compared to pregnant women who travel less than 30 minutes. This finding is consistent with the study done in Tigray, Ethiopia, that mothers reported the unavailability of health facilities close to their locality was a key barrier to utilizing available services from health institution [40]. This has an implication that pregnant women are forced to either travel long distances to get health services or otherwise don’t access the service given at health institution including nutrition and/or health related issues.
In this study pregnant women who had good knowledge of nutrition and health were less likely to be at risk of being suboptimal in nutrition and health practice compared to their counter parts. This finding is supported by studies done in different parts of Ethiopia like Misha Woreda [41], Addis Ababa [42], and West Gojjam [28]. The reason behind the similarity might be due to the fact that when women are knowledgeable about optimal nutrition and health, they may be aware of the consequences of suboptimal nutrition and health practices on their fetus, as well as on themselves, and they will be more inclined to practice optimal nutrition and health-related behaviors. This implies that, though knowledge is not behavior, it determines the practice through motivating mothers to make changes that could maximize optimal nutrition and health practices. As seen from our intervention, our intervention also improves participants’ knowledge of nutrition and health.
Moreover, the study also revealed that those pregnant women who had a favorable attitude towards nutrition and health were less likely to be at risk of being suboptimal in nutrition and health practice compared to pregnant women who were in their counterparts. Our intervention revealed that, participants in the intervention group had a more favorable attitude towards optimal nutrition and health than the control group. This study is in line with the study done among pregnant women in Indonesia that revealed providing nutrition and reproductive health education through small groups with interactive methods improves the attitudes of pregnant women [33].
Strength and Limitation
Strength
The strengths of this study are the use of the randomized controlled design that included a fairly large sample size. Because the intervention was delivered through health development armies who come from the same community, it improved the chance of sustainability.
Limitation
This study admits the following limitations: due to the nature of the intervention, allocation concealment was not achievable; nonetheless, the participants, HDAs and data collectors were blinded to the study hypothesis.
Some nutrition and health-related practices were self- reported and unable to be cross-checked during the data collection period.
Conclusions
This study demonstrated that behavior change communication (BCC) through the health development army using the guide of ENA frame works, and a framework for promoting maternal nutrition in developing countries developed by the Manoff Group is effective in improving the nutritional and health practices of pregnant women. Hence, this replicable behavior change communication intervention, with a focus on health development armies, can be scaled up and sustained with minimal investments through existing community structures. The findings also suggest policy makers should work in developing guideline with core contents on nutrition and health during pregnancy.
Acknowledgements
Jimma University supported the study by helping to create posters and brochures with pertinent images to show pregnant mothers, leaflets with key messages written in (local) languages, for transportation of researchers, data collectors, and perdium for health development armies.
The authors are grateful to West shoa zone and Ambo district personnel for providing permission to conduct the study, and as well as to the supervisor and data collectors who committed themselves throughout the study period.
Our thanks also go to all authors those who have availed their published articles free of charge for our literature review. Finally, we would like to express our gratitude to all participants who voluntarily participated in the study
Consent for Publication
Not applicable.
Availability of Data and Materials
Raw data on this research will be sent to the journal upon request.
Competing Interests
The authors declare that they have no competing interests.
References
-
Black RE, Allen LH, Bhutta ZA (2008) Maternal and Child Under nutrition Study Group. Maternal and child under nutrition: global and regional exposures and health consequences. Lancet 371(9608): 243-260.
-
McClure EM, Goldenberg RL, Dent AE, Meshnick SR (2013) A systematic review of the impact of prevention of malaria in pregnancy on low birth weight and maternal anemia. Int J Gynec Obst 121(2): 103-109.
-
World Health Organization (2013) Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition.
-
The manoff Group (2012) Guidance for Formative Research on Maternal Nutrition: Prepared for the Infant and Young Child Nutrition Project. MOG and University Research Co, Washington DC, USA, pp: 4-6.
-
Canavati SE, CLy P, Shafique M, Boukheng T, Rang C, et al. (2016) Evaluation of intensified behaviour change communication strategies in an artemisinin resistance setting. Malar J 15: 249.
-
Middleton PF, Lassi ZS, Tran ST, Bhutta Z, Bubner TK, et al. (2012) Nutrition interventions and programs for reducing mortality and morbidity in pregnant and lactating women and women of reproductive age: A systematic review. Campbell Systematic Reviews 8: 1-52.
-
WHO (2016) WHO recommendations on antenatal care for a positive pregnancy experience.
-
Oluwafolahan OS, Catherine AB, Olubukunola AJ (2014) Dietary Habits of Pregnant Women in Ogun-East Senatorial Zone, Ogun State, Nigeria: A Comparative Study. International Journal of Nutrition and Metabolism 6(4):42-49.
-
Hye-Kyung Oh, Sunjoo Kang, Sung-Hyun Cho, Yeong- ju Ju, Faye D (2019) Factors influencing nutritional practices among mothers in Dakar, Senegal. Plos One 14(2): e0211787.
-
Victoria Q (2006) Best practice in nutrition. Repositioning Nutrition as Central to Development, the World Bank, pp: 10-11.
-
USAID, WFP, FANTA 2, FHI 360 (2010) Malnutrition in Uganda: Uganda is Paying too High a Price. pp: 13-15.
-
Shemsu S, Argaw A, Zinab B (2020) Dietary Practice and Nutritional Status Among Pregnant Women Attending Antenatal Care at Mettu Karl Referral Hospital, Southwest Ethiopia. The Open Public Health Journal 13: 538-546.
-
Yalewdeg M, Birhane M, Adissu Y (2020) Dietary Practices and Their Determinants among Pregnant Women in Gedeo Zone, Southern Ethiopia: A Community- Based Cross-Sectional Study. Nutrition and Dietary Supplements 12: 267-275.
-
Federal Democratic Republic of Ehiopia, USAID (2012) A Tool to Support Nutrition Advocacy in Ethiopia. Ethiopia Profiles Estimates, Final Report, pp: 15-25.
-
Guyon AB, Quinn VJ (2011) Essential nutrition action frame work. Training guide for health workers. Core Group, Washington DC.
-
USAID/ENGINE, MOG (2014) Maternal Diet And Nutrition Practices And Their Determinants. Engine: A report on formative research findings and recommendations for social and behavior change communication programming in the Amhara, Oromia, SNNP and Tigray regions of Ethiopia, pp: 5-10.
-
Guyon AB, Nielsen J, Quinn V (2015) Understanding the Essential Nutrition Actions and Essential Hygiene Actions Framework. JSI Research & Training Institute, pp: 1-5.
-
Sharifirad GR, Tol A, Mohebi S, Matlabi M, Shahnazi H, et al. (2013) The effectiveness of nutrition education program based on health belief model compared with traditional training. J Edu Health Promot 2:15.
-
Saldanha LS, Buback L, White JM, Mulugeta A, Mariam SG, et al. (2012) Policies and program implementation experience to improve maternal nutrition in Ethiopia. Food Nutr Bull 33(2 Suppl): S27-S50.
-
JU, UG, LSHTM (2016) Facilitating accessible community- oriented health systems: the Health Development Army in Ethiopia. Jimma University, University of Glasgow, London School of Hygiene & Tropical Medicine.
-
Central Statistical Agency (Ethiopia), ORC Macro (2006) Ethiopia demographic and health survey (EDHS) 2005. Ethiopia, Calverton, Maryland.
-
CSA, ICF (2012) Ethiopia Demogeraphic and Health Survey 2011. Central Statistical Agency (CSA), Calverton, Maryland, USA.
-
CSA, ICF (2017) Ethiopia Demographic and Health Survey 2016. Central Statistical Agency (CSA) [Ethiopia], Addis Ababa, Ethiopia, Rockville, Maryland.
-
West Shoa Zone (2015) West Shoa Zone, Health Office.
-
Fekadu B, Daba G, Habtamu F, Garoma W (2013) Assessment of Knowledge and practice of Pregnant Mothers on Maternal Nutrition and Associated Factors in Guto Gida Woreda, East Wollega Zone, Ethiopia, J Nutr Food Sci 3(6): 1-7.
-
Morseda C, Camille RG, Ashraful A, Michael JD (2017) Making a balanced plate for pregnant women to improve birthweight of infants: a study protocol for a cluster randomised controlled trial in rural Bangladesh. Nutrition and metabolism 7: 1-10.
-
Gebreyesus SH, Lunde T, Mariam DH, Woldehanna T, Lindtjørn B (2015) Is the adapted Household Food Insecurity Access Scale (HFIAS) developed internationally to measure food insecurity valid in urban and rural households of Ethiopia? BMC Nutrition 1: 1-10.
-
Yeshalem MD, Getu DA, Tefera B (2020) Dietary practices and associated factors among pregnant women in West Gojjam Zone, Northwest Ethiopia. BMC Pregnancy and Childbirth 20(1): 18.
-
Meseret MB, Walelegn WY, Aysheshim KB (2018) Knowledge and practice of iodized salt utilization among reproductive women in Addis Ababa City. BMC Res Notes 11: 734.
-
Walleligne BT, Amare LM (2019) Knowledge and Utilization of Iodized Salt and Its Associated Factors at Household Level in Mecha District, Northwest Ethiopia. J Nutr Metab 2019: 9763830.
-
Guled RA, Bin Mamat NM, Abu Bakar WAM, Assefa N, Balachew T (2016) Knowledge, Attitude and Practice of Mothers/caregivers on Infant and Young Child Feeding in Shabelle Zone, Somali Region, Eastern Ethiopia: A Cross Sectional Study. Revelation and Science 6(2): 42-54.
-
Samdal GB, Eide GE, Barth T, Williams G, Meland E (2017) Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act 14(1): 42.
-
Endah Permatasari TA, Rizqiya F, Kusumaningati W, Suryaalamsah II, Hermiwahyoeni Z (2021) The effect of nutrition and reproductive health education of pregnant women in Indonesia using quasi experimental study. BMC Pregnancy and Childbirth 21: 180.
-
Beiguelman B, Colletto GMDD, Franchi-Pinto C, Krieger H (1998) Birthweight of twins: 1. the fetal growth patterns of twins and singletons. Genet Mol Biol 21(1): 151-154.
-
Downe S, Finlayson K, Tuncalp O, Gulmezoglu AM (2016) What matters to women: a systematic scoping review to identify the processes and outcomes of antenatal care provision that are important to healthy pregnant women. BJOG 123(4): 529-539.
-
Taddese AZ (2015) Dietary practices of pregnant women and its associations with maternal and perinatal outcomes in rural Central Ethiopia.
-
Worke SY, Tigist ST (2022) Nutritional practice of pregnant women in Buno Bedele zone, Ethiopia: a community based cross-sectional study. Reproductive health 19: 84.
-
Shehab NS, Fouda ML, Ahmed MH (2012) Nutritional awareness of women during pregnancy. J Am Sci 8(7): 10.
-
Hye-Kyung O, Kang S, Sung-Hyun C, Yeong-ju J, Faye D (2019) Factors influencing nutritional practices among mothers in Dakar, Senegal. Plose One 14(2): 1-14.
-
Beyene SA, Weldegerima L, Tela FG, Seid O, Brown AT, et al. (2021) Barriers to utilize nutrition interventions among lactating women in rural communities of Tigray, northern Ethiopia: An exploratory study. Plose One 6(4): 1-14.
-
Abute L, Beyamo A, Erchafo B, Tadesse T, Sulamo D, et al. (2020) Dietary Practice and Associated Factors among Pregnant Women in Misha Woreda, South Ethiopia: A Community-Based Cross-Sectional Study. Journal of Nutrition and Metabolism 2020: 5091318.
-
Zelalem T, Erdaw A, Tachbele E (2018) Nutritional knowledge, attitude and practices among pregnant women who attend antenatal care at public hospitals of Addis Ababa, Ethiopia. International Journal of Nursing and Midwifery 10(7): 81-89.
- The Role of Podocyte Apoptosis and the Involvement of SIRT1 in Diabetic Nephropathy
- Dealcoholization of Beer by Osmotic Distillation for the Beverage Industry
- Biopolymer-Based Edible Packaging- Biomaterials, Methods, and Applications in Food Industry: An Updated Review
- Influence of Bioprocessing Methods on 'China Rice' (Gawal R1), and Soyabean Supplementation on the Quality of Complementary Food
- Cassava (Manihot esculenta) Varietal Growth, Yield and Cyanide Content Performance in Three Sites in the South- Eastern Semi Arid Regions of Kenya
- Food Waste Treatment, Recycling, Management and Production of Value-Products-An Update on Methodologies and Current Trends