Case of Autoimmune Pancreatitis with Pancreatic Mass with Obstructive Jaundice, Timely Diagnosis Saved from the Major Surgery
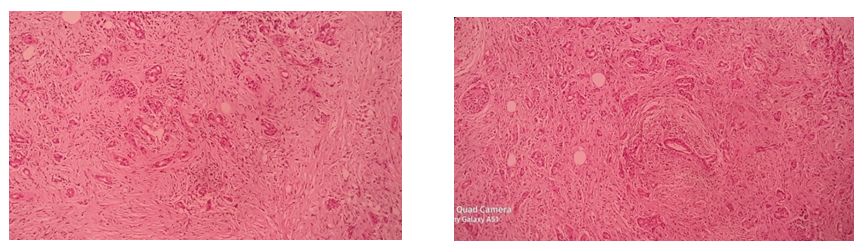
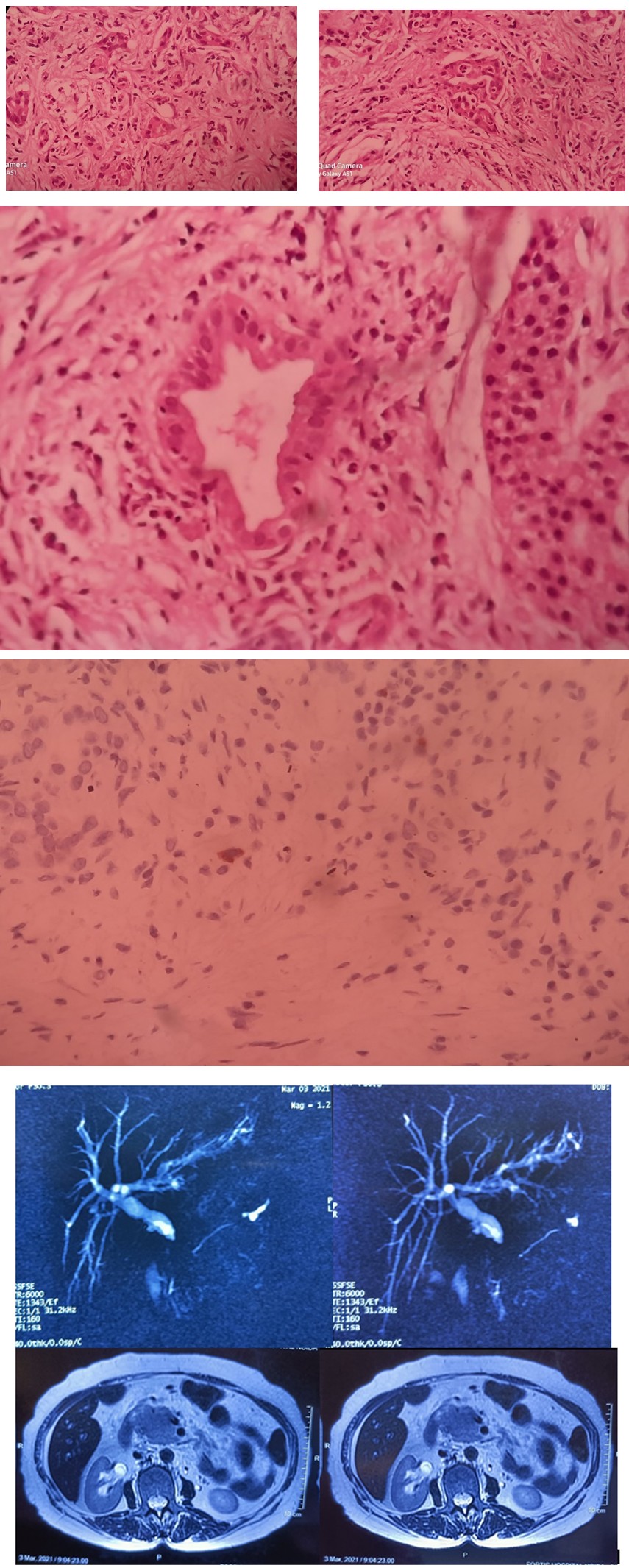
A 68-year-old female presented with a 6 month history of jaundice, epigastric discomfort, anorexia and 4 kg weight loss. Physical examination was unremarkable, except for icterus. Her Liver function tests were deranged. Abdominal computed tomography (CT) revealed pancreatic mass. Magnetic resonance cholangio-pancreatography (MRCP) showed intra hepatic biliary radical dilatation (IHBRD) and Pancreatic mass with double duct sign. Pancreatic malignancy was suspected with increased CA19.9 levels. Endoscopic retrograde cholangio-pancreatography (ERCP) was attempted but cannulation was not possible. Staging laparoscopy and tru-cut biopsy was performed. Histopathology showed plasma cells infiltrates with increased IgG4 suggestive of autoimmune pancreatitis (AIP). Surrounding lymph nodes showed prominent follicular hyperplasia. Patient made an uneventful recovery with steroids, the patient remains asymptomatic with normal liver functions. There is no serological evidence for other autoimmune diseases.
Review of Literature
IgG4-related disease is immune mediated, multi- organ disorders that can mimics malignant, infectious, and inflammatory diseases. The presence of autoantibodies of IgG4 subclass is peculiar for this but not essential criteria. Diagnosis of this condition from its differential diagnosis is paramount as this is a potentially medically treatable condition. Historically this was initially described as Mickulicz disease in 1892, followed by sclerosing cholangitis and autoimmune pancreatitis (AIP) in 1995. Finally recognized as a unified disease only in 2003. Overall prevalence of AIP is 4.6 per 100000 people, Incidence is 1.4 per 100 000 people, Men > women (3.2:1), mean age at diagnosis was 63.3 years [1]. The prevalence of IgG4-related sclerosing cholangitis is unknown, male to female ratio was 4.8:1, median age was 66.2 years, and around 87% patients had associated autoimmune pancreatitis. Biliary manifestation was restricted to the intra-pancreatic portion in 64% patients [2]. AIP manifests predominantly with painless obstructive jaundice (33- 59%), mimicking malignancy, followed by abdominal pain (32%), weight loss (15%) and back pain (15%), whereas clinical presentation of IgG4 SC are obstructive jaundice as a symptom at 77% of cases in the USA, 74% of cases the UK and 35% of cases in Japan , 28% show no symptoms [3].
There are 2 types of AIP presentation, in type 1 AIP, extra pancreatic sites are also involved along with pancreas, elderly age group with male predominance, with elevated serum IgG4 levels, on biopsy predominant have lympho plasmacytic sclerosing pancreatitis (LPSP), and with predominant infiltrating cells are IgG4 and plasma cells. In Type 2 AIP only pancreas involved without extra pancreatic involvement, relatively in young age onset, equal in both gender, serum IgG4 levels are normal and granulocytes are the predominant infiltrating cells on biopsy and have idiopathic duct centric pancreatitis (IDCP) pattern. Relapse rate is high in type 1 as compared to type 2.
| Parameter | Peak values Before treatment | After treatment |
|---|---|---|
| Haemoglobin in g/dL | 10.8 | 12.5 |
| Total leucocyte count/µL | 12.1 | 15.1 |
| Differential count, % | N 82%,L-12% | N 91%,L 7% |
| Platelets/µL ×103 | 169 | 156 |
| Urea in mg/dL | 37 | 38 |
| Creatinine in mg/dL | 0.72 | 0.81 |
| Total /direct bilirubin in mg/dL | 17.9 | 13.63 |
| Aspartate transaminase <40 U/L | 421 | 160 |
| Alanine transaminase <40 U/L | 169 | 74 |
| Alkaline phosphatase 30-120 U/L | 460 | 209 |
| GGT (normal 6-46 U/L) | 498 | 172 |
| Protein in g/dL | 3.6 | 5.1 |
| Albumin in g/dL | 2.01 | 2.9 |
| International normalized ratio | 1.5 | 1.1 |
| S. IgG level (normal 6.2-14.4 g/L) | 15.5 | 12.6 |
| IgG level (normal 0.07-0.88 g/L) 4 | 1.8 | 0.8 |
| CA19.9 ( normal <37 U/ml) | 98.62 | 34.93 |
Diagnosis
Universally accepted criteria for diagnosis of AIP are HISORt Criteria given by the Mayo clinic based on 5 main diagnostic criteria: histological chracterstics, imaging findings, serology, other organ involvement and response to steroid therapy [4]. H-Histological characteristics, 3 histologic key findings are Lymphoplasmacytic infiltration affecting the tissue either diffusely or patchy and focusing on ducts. For the diagnosis of AIP, the number of IgG4 plasma cells should exceed 50 cells/high-power field (HPF) in surgical specimens and 10 cells/HPF in biopsy samples. Storiform fibrosis composed of thick collagen bundles which form a characteristic “swirling” and focally cartwheel-like (e.g., storiform) pattern. Obliterative phlebitis characterized in its early stage by a mainly lymphocytic perivascular infiltrates and in its later stages by an intravascular infiltration that finally leads to fibro inflammatory obliteration. I-Imaging charterstics [3, 5, 6]. Parenchymal changes suggestive of AIP are Diffuse or (multi-) focal enlargement with loss of the normal multi-lobulated pattern (‘sausage-like’ shape); with diffuse involvement, more frequent in type 1 and focal involvement in AIP type 2. Altered imaging characteristics, such as lower signal intensity (SI)/echogenicity on unenhanced T1-w MRI/(E)US, respectively, moderately higher SI on T2-w MRI, impeded diffusion on MRI, and increased 18F fluorodeoxyglucose(FDG)-uptake on PET-CT [5] compared with normal parenchyma. Post injection of (iodine, gadolinium, or microbubble-based) contrast media, there is dotted/patchy enhancement in the late arterial/ pancreatic phase that progressively increases towards the later vascular phases. Rectangular shape of the tail (‘cut-tail sign’). Thin peripancreatic edematous rim or progressively enhancing true capsule.
Ductal changes suggestive of AIP are Long-segment (i.e. 1/3 of the length) or multifocal main pancreatic duct (MPD) involvement (narrowing or vanishing) without upstream dilatation or other signs of obstructive pancreatitis. Skip lesions, i.e. 2 involved MPD-segments separated by a normal MPD-segment. ‘Duct-penetrating’ (i.e. visible MPD- and/or common bile duct (CBD) lumen) and ‘icicle’ (i.e. a progressive decrease of MPD-diameter) signs within an enlarged parenchymal area. Contrast-enhanced CT shows diffuse enlargement with delayed enhancement and rim- like enhancement in the pancreas. 4 types of IgG4 related sclerosing cholangitis described by Nakazawa, et al. [7]. S-Serology: Significance of serum IgG4 level: 2 or 3 times the upper limit of the reference range of the IgG4 level was a useful marker for the diagnosis of various types of IgG4-RD and the optimal cutoff level was 248 mg/dL [8]. Metanalysis (n = 6048), by Xu, et al. [9], showed Sensitivity of 85%, Specificity value of 93% [9]. IgG4/IgG1, with a cutoff value of 0.24. Doorenspleet, et al. [9] showed that IgG4/IgG RNA in blood, have 94% sensitivity, 99% specificity to differentiate IgG4 pancreatobiliary diseses from other etiologies [6].
O-Other Organ Involvement
Hilar/intrahepatic biliary strictures, persistent distal biliary strictures, parotid or lacrimal gland involvement, mediastinal lymphadenopathy or retroperitoneal fibrosis can be present. Type 1 autoimmune pancreatitis (AIP) is the pancreatic manifestation of a multi-organ disease, named immunoglobulin G4 (IgG4)-related disease while type 2 AIP is a pancreas specific disorder not associated with IgG4 [10].
T-Treatment
Spontaneous resolution of symptoms without medical, interventional endoscopic or surgical treatment occurs in 10- 25% of cases. Treatment required in the following patients:
- All symptomatic patients (e.g. suffering from pancreatic pain, obstructive jaundice).
- Asymptomatic patients in case of: Persistence of a pancreatic mass in imaging to rule out cancer.
- Persistence of liver test abnormalities (cholestasis) in case of associated IgG4-related cholangitis.
- In subclinical situations that could lead to severe or irreversible organ failure [11].
Phases of Treatment
Induction Phase: Steroids, methylprednisolone, Dose of 0.6- 0.8 mg/kg/day , ~30-40 mg/day for 1 month, Response is re- assessed at 2-4 weeks interval with clinical, biochemical, and morphological markers, tapered by 5 mg every two weeks (over 3-6 months), Response rate (~98%) [12]. Maintenance Phase: No high quality evidence, dose of glucocorticoids 10 mg/day. Risk of recurrence [12] was around 40% in patients without prior steroid therapy, ~25% in patients who received steroids previously. Expert recommendations -2.5-10 mg/day prednisolone for 12 months. Some Japanese centers continue low-dose (5 mg) prednisolone for as many as 3 years and beyond [13].
Remission Criteria: Defined as fulfilling each of the following criteria after 6 months of treatment: 50% decline in IgG4 levels, Glucocorticoids tapered to maintenance dose 10 mg/day; and No relapse during glucocorticoid tapering within 6 months [12]. Long-term prognosis of autoimmune pancreatitis with and without corticosteroid treatment.
Relapse: Risk factors for relapse: The relapse rate is high and range from 26% -70%, more common in patients with high baseline serum IgG4 levels [14]. Relapse management: Three common regimens for relapse management are:
- High-dose glucocorticoids followed by maintenance treatment with low dose glucocorticoids or a glucocorticoid-sparing agent.
- High-dose glucocorticoids without maintenance treatment.
- Rituximab induction with or without maintenance rituximab. Glucocorticoids (>95% success rate), first option if tolerated by the patient [11]. Role of immunosuppressant/biological are considered in Disease relapse for
- Maintenance of remission strategy.
- High risk of relapse (multi-organ involvement).
- If no change in disease activity or the disease relapsed during glucocorticoid taper or discontinuation.
Rituximab: If resistant or intolerant to high-dose glucocorticoids to maintain remission, Failed to respond to immunosuppressive therapies , Two dose regimens are: dose is 375 mg/m2 body surface area, weekly for 4 weeks infusions every 2-3 months or Two 1000 mg infusions 15 days apart every 6 months. Role of biliary stenting without cholangitis in patients with increases risk of cholangitis and those where condition may propagate pancreatic stone formation [15]. Serum liver test abnormalities are normalized in 80% and 100% at 15 and 21 days, respectively without stenting [16]. Long term prognosis: Both endocrine and exocrine insufficiency can develop on long term, more than 1/3rd patients, after 3 years of diagnosis. Diabetes mellitus 19-67% and exocrine insufficiency in 36-85% [17]. The outcome of patients with type 2 AIP, a condition often associated with inflammatory bowel disease is not different from that of patients with type 1 AIP, except for diabetes [17].
References
-
Kanno A, Masamune A, Okazaki K, Kamisawa T, Kawa S, et al. (2015) Nationwide epidemiological survey of autoimmune pancreatitis in Japan in 2011. Pancreas 44(4): 535-539.
-
Tanaka A, Tazuma S, Okazaki K, Nakazawa T, Inui K, et al. (2017) Clinical Features, Response to Treatment and Outcomes of IgG4- Related Sclerosing Cholangitis. Clin Gastroenterol Hepatol 15(6): 920-926.
-
Kamisawa T, Zen Y, Nakazawa T, Okazaki K (2018) Advances in IgG4-related pancreatobiliary diseases. Lancet Gastroenterol Hepatol 3(8): 575-585.
-
Zhang L, Chari S, Smyrk TC, Deshpande V, Kloppel G, et al. (2011) Autoimmune pancreatitis (AIP) type 1 and type 2: an international consensus study on histopathologic diagnostic criteria. Pancreas 40(8): 1172-1179.
-
Zhao Z, Wang Y, Guan Z, Jin J, Huang F, et al. (2016) Utility of FDG-PET/CT in the diagnosis of IgG4-related diseases. Clin Exp Rheumatol 34(1): 119-125.
-
Doorenspleet ME, Hubers LM, Culver EL, Wenniger LJMDB, Klarenbeek PL, et al. (2016) Immunoglobulin G4(+) B-cell receptor clones distinguish immune globulin G4-related disease from primary sclerosing cholangitis and biliary/pancreatic malignancies. Hepatology 64(2): 501-507.
-
Nakazawa T, Naitoh I, Hayashi K, Okumura F, Miyabe K, et al. (2012) Diagnostic criteria for IgG4-related sclerosing cholangitis based on cholangiographic classification. Liver, Pancreas, and Biliary Tract 47: 79-87.
-
Yu KH, Chan TM, Tsai PH, Chen CH, Chang PY (2015) Diagnostic Performance of Serum IgG4 Levels in Patients With IgG4-Related Disease. Medicine (Baltimore) 94(41): e1707.
-
Xu WL, Ling YC, Wang ZK, Deng F (2016) Diagnostic performance of serum IgG4 level for IgG4-related disease: a meta-analysis. Sci Rep 6: 32035.
-
O’Reilly DA, Malde DJ, Duncan T, Rao M, Filobbos R (2014) Review of the diagnosis, classification and management of autoimmune pancreatitis. World J Gastrointest Pathophysiol 5(2): 71-81.
-
Lohr JM, Beuers U, Vujasinovic M , Alvaro D, Frokaer JB, et al. (2020) European Guideline on IgG4-related digestive disease-UEG and SGF evidence-based recommendations. United European Gastroenterol J 8(6): 637-666.
-
Okazaki K, Chari ST,Frulloni L, Lerch MM, Kamisawa T, et al. (2017) International consensus for the treatment of autoimmune pancreatitis. Pancreatology 17(1): 1-6.
-
Kubota K, Kamisawa T, Okazaki K, Kawa S, Hirano K, et al. (2017) Low-dose maintenance steroid treatment could reduce the relapse rate in patients with type 1 autoimmune pancreatitis: a long-term Japanese multicenter analysis of 510 patients. J Gastroenterol 52(8): 955-964.
-
Lanzillotta M, Mancuso G, Torre ED (2020) Advances in the diagnosis and management of IgG4 related disease. BMJ 369: m1067.
-
Matsubayashi H, Kishida Y, Iwai T, Murai K, Yoshida M, et al. (2016) Transpapillary biliary stenting is a risk factor for pancreatic stones in patients with autoimmune pancreatitis. Endosc Int Open 4(8): E912-17.
-
Yukutake M, Sasaki T, Serikawa M, Minami T, Okazaki A, et al. (2014) Timing of radiological improvement after steroid therapy in patients with autoimmune pancreatitis. Scand J Gastroenterol 49(6): 727-733.
-
Maire F, Baleur YL, Rebours V, Vullierme MP, Couvelard A, et al. (2011) Outcome of patients with type 1 or 2 autoimmune pancreatitis. Am J Gastroenterol 106(1): 151-156.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient