Conjunctival Pedicle Graft for the Treatment of Deep and Perfuraded Corneal Ulcers in Dogs
The purpose of this study was to present the conjunctival pedicled graft technique in the surgical treatment for deep stromal ulcers, decemetoceles, and corneal perforations in dogs, and to determine the effectiveness of this technique in ulcer healing and preservation of vision. This type of ulcer has been and should be treated as a surgical emergency because of the risk of rupture and vision loss. The conjunctival graft is the treatment of choice, because it provides blood supply to the cornea, contributing to the healing and integrity of the segment. The pedicle type graft was employed because it provides tissue mobility, easy visualization, and topical application of drugs, therefore reducing the dehiscence rate. This study included 10 dogs of different breeds, with procedures performed between January and October 2022 at the Animal Eye Institute clinic, located in Cincinnati/OH. With data collection, it was possible to verify the effectiveness of this technique to treat deep and perforated ulcers and the prevalence of these types of ulcers in brachycephalic dogs.
Introduction
The cornea is located in the anterior portion of the ocular bulb, being the outermost layer, which gives protection to the internal structures and transparency to the eye. It is composed of four layers: stratified epithelium and its basement membrane, stroma, Descemet’s membrane, and epithelium Maggs DJ, et al. [1].
The corneal sensitivity varies by species, corneal region, and in the dog, by skull conformation Gelatt KN, et al. [2]
Corneal ulceration, or ulcerative keratitis, is one of the most common eye conditions seen in small animal clinics, especially in dogs. When an ulcer compromises more than 50% of the stroma, the regeneration of the fibrils is slow, as there is no blood supply coming from the cornea Maggs DJ, et al. [1] and for this reason, conjunctival grafts are the treatment of choice, as they preserve corneal and ocular integrity, replace lost corneal tissue and provide vascularization. The pedicled graft created from the bulbar conjunctiva is the most used in these cases Gelatt KN, et al. [2].
Deep stromal and/or perforated ulcers and descemetoceles, are considered ophthalmic emergencies Gogova S, et al. [3] These types of ulcers are infected by bacteria, and of rapid progression, which compromise the integrity of the eyeball, and consequently, the vision, and clinical findings can be found such as: uveitis of the anterior chamber, edema, aqueous “flare”, hyphema and hypopium Gelatt KN, et al. [2].
The common causes for the occurrence of these ulcers are related to inadequate protection of the cornea, abnormal exposure of the orbit, as in brachycephalic dogs, deficiency in the film and tear production, presence of abnormal eyelashes and/or abnormal position of the eyelids, eyelid masses and traumas Maggs DJ, et al. [1].
This study aims to present 10 cases of conjunctival pedicle graft in 2022 for the treatment of deep and/or perforated ulcers in dogs, present the eminent causes and from the results evaluate the effectiveness of the technique.
Case Report
The procedures for the treatment of deep and/or perforated corneal ulcers were performed at the Animal Eye Institute, located in Cincinnati/Ohio, and this clinic specializes only in the diagnosis and treatment of diseases and ophthalmic changes of animals. The study had the participation of 10 dogs, of different breeds and ages, and 7 of them were followed from the diagnosis of the ulcer, performance of the procedure, until the returns after its completion. The other 3 dogs, had already performed the procedure, and came to the clinic for returns. Conjunctival pedicle grafts were performed in 2022, from January to October [3, 4, 5, 6, 7].
All patients in this study underwent complete ophthalmologic examination. Following the order of its realization, the first test was to check if the vision was preserved, for this is observed the eyelid response to the attack and the light, and pupillary reflex, and the first two mentioned are directly related to vision. The positive response shows the relative functional integrity of the retina and optic to the optic nerve, which performs the feed-back mechanism to the visual cortex, conferring vision, but being positive does not ensure that the posterior segment is normal [8, 9, 10, 11, 12].
To confer the pupillary reflex, direct and indirect pupillary constriction to light was observed, whether the pupil of the orbit receiving the light is contracting and whether the other side also responds equally to this reflection, respectively [13]. This reflex is related to the optic (II) and oculomotor (III) cranial nerve pairs, being considered a reflex related to the muscles, and may be present in dogs that do not have vision. In cases of edema, uveitis, watery flare and hyphema in the anterior chamber secondary to the ulcer, it may not be possible to visualize the reflexes, as it will compromise the dog’s vision.
Afterwards, the Schirmer Tear Test (SLT) was performed, being a quantitative test to check the tear production of the patients [14, 15, 16, 17]. With this test, it was possible to identify whether or not the patient had Keratoconjunctivitis sicca (CCS), and to check whether those who were already positive before the test, are responding well to the treatment and with tear production within normal limits. The paper filter, where the values are arranged in millimeters (mm), was inserted into the lower conjunctival sac of the animal. Dogs that presented values between 10 and 15 mm/min are considered suspicious, and those below this value of 10 mm/ min are suffering from CCS. The test was not carried out in the eye that was affected, the patients have an increased painful stimulus and there is an alteration in the values due to tearing. There were no new cases of CCS [18, 19, 20, 21].
Subsequently, a tonometry exam was performed, with Tonopen®, to check the intraocular pressure (IOP) only in the unaffected eye, and results above 25 mmHg are considered positive for glaucoma. This exam was not performed in the eye with suspected ulcer in any of the patients, since deep ulcers normally cause high discomfort, in addition to being extremely sensitive, as they are at risk of rupture. None of the patients tested positive for glaucoma.
Therefore, the Colorimetry test was performed, being the most important in this case, to verify the presence of ulcers in the cornea. Fluorescein eye drops (dye) were used, fluorescing green, which, when dripped, are absorbed by the photoreceptors of the stroma and indicate the presence of the ulcer in the cornea. Through slit-lamp biomicroscopy and the use of fluorescein, it is possible to differentiate a deep corneal ulcer from a superficial or indolent ulcer, and diagnose its type, whether it is a stromal ulcer, descemetocele or perforation, and how much of the cornea was compromised. This exam also contributed to clinical findings in the anterior chamber of the lens, such as uveitis, edema, hyphema, epithelium and/ or cornea degeneration, in addition to being able to verify if there were unwanted eyelashes in the palpebral conjunctiva, which could be the cause for the formation of the ulcer.
The last examination performed was Ophthalmoscopy or Indirect Fundoscopy, to evaluate the structures of the eye fundus, retina, retinal vessels and optic nerve. Animals with mature cataracts, inflammation and edema prevented the visualization of these structures (Table 1).
| Vision in the Pre-Surgery | Vision on Return | Ulcer (1st Return) | Ulcer (2nd Return) | Dehiscence | Year of Surgery | |
|---|---|---|---|---|---|---|
| 1 | RP a ameaça (+) RP a luz (+) RPP (+) | RP a ameaça (+) RP a luz (+) RPP (+) | -- | No | October, 2022 | |
| 2 | RP a ameaça (+) RP a luz (+) RPP (+) | RP a ameaça (+) RP a luz (+) RPP (NV) | -- | No | June, 2022 | |
| 3 | RP a luz OD e OE (+)(+) RPP OD e OE (NV)(NV) RP a ameaça OD e OE (--)(--) | RP a luz OD e OE (+)(+) RPP OD e OE (NV)(NV) RP a ameaça OD e OE (+)(--) | -- | No | September, 2022 | |
| 4 | RP a ameaça (--) RP a luz (+) RPP (NV) | RP a ameaça (+) RP a luz (+) RPP (NV) | -- | No | September, 2022 | |
| 5 | RP a ameaça (--) RP a luz (--) RPP (NV) | RP a ameaça (--) RP a luz (+) RPP (NV) | + | -- | No | January, 2022 |
| 6 | RP a ameaça (+) RP a luz (+) RPP (+) | RP a ameaça (+) RP a luz (+) RPP (+) | -- | No | September, 2022 | |
| 7 | RP a ameaça (+) RP a luz (+) RPP (+) | RP a ameaça (+) RP a luz (+) RPP (+) | + | -- | No | August, 2022 |
| 8 | RP a ameaça (+) RP a luz (+) RPP (NV) | RP a ameaça (+) RP a luz (+) RPP (+) | -- | No | September, 2022 | |
| 9 | RP a ameaça (+) RP a luz (+) RPP (NV) | RP a ameaça (+) RP a luz (+) RPP (NV) | -- | No | October, 2022 | |
| 10 | RP a ameaça (--) RP a luz (--) RPP (NV) | RP a ameaça (+) RP a luz (+) RPP (NV) | -- | No | September, 2022 |
Table 1: How was the Patient’s Vision Before the Surgery, with the Acronym Rp Meaning Eyelid Reflex, Rpp Referring to Pupillary R
Table 1: How was the Patient’s Vision Before the Surgery, with the Acronym Rp Meaning Eyelid Reflex, Rpp Referring to Pupillary Reflex, and Nv Meaning not Visible, Being In (-) the Dogs that Presented Negative Reflexes and (+) For Dogs that Presented Positive Reflex. all Dogs Underwent Follow-up 15 Days after the Procedure, with (-) for Dogs that no Longer had the Ulcer and (+) For Dogs that were Still Found to have an Ulcer. The Dogs with the Present Ulcer Underwent a new Follow-up 15 Days Later, Showing (-) as Negative for ulcer.
After the complete examination, the cases in this study were treated as ophthalmic emergencies, as they had ulcers with involvement of more than 50% of the cornea. After the tutor’s consent, they were taken to the pre- and post-surgical area, and submitted to a blood test, complete blood count and serum biochemistry (total proteins, albumin, globulin, ALT, AST, alkaline phosphatase, GGT, amylase, bilirubin, urea and creatinine, glucose, phosphorus, calcium, sodium, potassium, cholesterol and triglycerides), to assess red and white blood cells, kidney, liver and pancreatic function of the dog, for anesthetic risk. Some of the older dogs had a small increase in the result of the enzyme Alanine aminotransferase (ALT), which is associated with the liver, this being a common alteration to be found in older dogs, but not limiting the patient to undergo general anesthesia.
Parameters of temperature, blood pressure, heart and lung auscultation were also performed, and all patients were clinically healthy, with vital parameters within normal limits.
All patients were placed on intravenous (IV) access for administration of anesthetic drugs. The dogs received Rimadyl (Rimadyl® - Zoetis), a non-steroidal anti-inflammatory drug (NSAID), at a dose of 4.4 mg/kg, subcutaneously (SC), 30 to 40 minutes before the procedure, contributing to analgesia and providing anti-inflammatory action.
Induction was performed with Propofol (PropoFlo®- Abbott) at a dose of 3 to 8 mg/kg IV. Afterwards, the antibiotic Cefazolin (Ancef®) was administered at a dose of 10 to 30 mg/kg IV, to prevent bacterial infections during and after the surgical procedure. The induction being effected, through the loss of reflexes, the patient was intubated with an orotracheal tube, and its thickness was determined according to the thickness of the patient’s trachea (𝑃𝐸𝑆𝑂 × 4 = √𝑥). Atracurium (Atracurium – USP) was also administered at a dose of 0.1 to 0.3 mg/kg IV, which performs neuromuscular blockade, contributing to rapid control of the airways and centralization of the eyeball for the performance of of the procedure.
Anesthetic maintenance was performed with Isoflurane (Forane® – USP), diluted in 100% oxygen using a universal vaporizer, in a partial gas rebreathing circuit. For field preparation, aseptic cleaning of the periocular region and eyelids of the affected eye was performed with a topical degerming solution (polyvidone iodine 10%) and the excess was removed with gauze containing lactated Ringer’s serum.
The pedicled conjunctival graft for the treatment of deep or perforated ulcers is performed with the aid of a surgical microscope, for enlargement of the structures and better visualization by the surgeon. The graft was then harvested from the dorsal bulbar conjunctiva with Westcott scissors, dissecting Tenon’s fascia through blunt excision, and trimming according to the size of the ulcer, taking care not to create holes in the graft (Figure 1). The necrotic corneal epithelium associated with the ulcer was debrided with a Beaver blade nº 64 up to 1 mm in circumference from the edge of the ulcer. The fibrin clot was gently removed from the corneal perforation and the anterior chamber was secured with viscoelastic. The graft was sutured to the cornea through a simple interrupted suture in the ulcer bed with absorbable vicryl 9-0 thread with a single cardinal stitch at the apex of the ulcer. The conference was held of the size of the graft in the area and was further dissected from Tenon’s fascia to optimally size the area, and thus reduce tension for greater mobility. The remainder of the graft was sutured in place using a simple continuous suture with 9-0 vicryl absorbable thread and the base of the graft fixed in the dorsal extension of corneal perforation with interrupted single stitch with absorbable vicryl 9-0 suture (Figure 1).
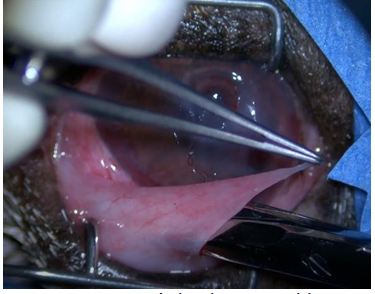
Source: Personal Collection. Figure1: Tenon’s Fascia Being Dissected from the Bulbar Conjunctiva Using Westcott Scissors for Placement of the Pedicle Graft.
The same technique was used for all dogs in this study, but with variations in size and sutures performed on the edges of the graft, as both are dependent on the extent of the ulcer in the corneal epithelium.
The procedure time ranged from 15 to 50 minutes. There was this variation according to the extent of the ulcer, the more fragile, the more delicate the procedure and the longer the time to be spent. And the more extensive the ulcer, the greater the debridement, the size of the graft, and consequently more interrupted than continuous sutures are needed, in order not to run the risk of dehiscence, which also contributes to this increase in time. It is normal that after this procedure, patients have the operated eye more red, swollen and with increased tearing, for the next 7 to 10 days.
Conjunctival graft tissue has a pink to reddish color on the surface of the cornea. During the process it will become more and more clear and transparent, but it will always be visible. Vision is improved as the inflammation created by the ulcer and also the healing process reduces.
The dogs in this study had no complications during the trans-surgery. After the dogs returned from the anesthetic plane and became alert, parameters were made to check intraocular pressure, cardiac and respiratory auscultation, temperature and blood pressure, all of which were within normal limits. They were medicated for comfort and pain relief with Carprofen (NSAID) at a dose of 2.2 to 4.4 mg/kg and oral Tramadol (Opioid) at a dose of 1 to 4 mg/kg, and were discharged on the same day.
The sutures performed are quite fragile, so to avoid possible trauma to the cornea and make the graft unfeasible, all patients were discharged using Elizabethan Necklace, and recommended to use it for 15 days, until their return.
The prescribed medications varied for each patient according to their history and needs. All dogs received two topical antibiotic eye drops, which have a spectrum for gram positive and gram negative bacteria, Ofloxacin 0.3% (Fluoquirolone) and Terramycin (Oxytetracycline), respectively, being prescribed to be instilled in the eyes with the pedicled graft four times a day (QID). A broad-spectrum oral antibiotic was also prescribed, varying the prescription between Doxycycline (50 mg, 100 mg or 200 mg) or Amoxicillin (50 mg, 150 mg or 300 mg), twice a day (BID). All patients received Tramadol (Opioid) for analgesia, and Carprofen (NSAID), which is anti-inflammatory and analgesic, also helping to control pain. Patients with perforated ulcers were also given Atropine 1% (ointment), BID, to reduce painful spasms. All medications were prescribed for use until return, in 15 days. The medication for the treatment of CCS (Tacrolimus or Cyclosporine) in carrier dogs was suspended until complete healing of the ulcer.
All patients underwent follow-up, which worked as follows: 15 days after the procedure, they returned to the clinic, underwent a complete ocular examination, with the objective of verifying whether the sutures were intact, whether the graft was healthy and viable, diagnosing whether it was not. there was more infection and the ulcer had healed after graft placement. All patients who tested negative, ceased using previously prescribed medications, and received a new prescription, anti-inflammatory topical eye drops, ranging from Diclofenac (NSAID), NeoPoliDexa (AIE), or using both simultaneously, with the aim of to cease intraocular edema and inflammation. They were prescribed until the new return visit, varying between BID or TID, depending on the patient’s needs. These dogs return again after a month, to check if there is no longer any type of active inflammation and to wean off the anti-inflammatory drugs. Patients who did not have the ulcer completely healed at the first follow-up after the procedure stopped using oral antibiotics and pain medication, and maintained the use of antibiotic eye drops, oral anti-inflammatory and the use of Elizabethan collar, with a new return after 15 days. After 15 days and the verification that the ulcer was healed and without the presence of infection, they followed the same guidelines as the other patients.
Discussion
Within Veterinary Ophthalmology, deep ulcerative keratitis is one of the diseases that most affects dogs, leading, in most cases, to corneal perforation and loss of vision, due to its rapid progression. It is characterized by the destruction of the corneal epithelium and the partial or total loss of the corneal stroma, according to Neto S, et al. [4]. As can be seen in this study, all dogs had more than 50% of the cornea compromised, being stromal ulcers, descemetoceles and/or perforations (Table 2).
It was reported by tutors that the progression of clinical signs such as differences in corneal coloration was observed within 24 to 48 hours, confirming the rapid progression of these infected ulcers, which should be treated as ophthalmic emergencies.
According to the results shown in Table 2 50% of the dogs were diagnosed with descemetoceles, with approximately 99% involvement through the cornea; 20% were diagnosed with perforated ulcers, with 100% of the cornea compromised; 50% were diagnosed with stromal ulcers, and in this study, 50 to 95% of corneal involvement was considered. Of these results, 2 patients were diagnosed with two ulcers, a French Bulldog and a Shih Tzu, respectively, and one was diagnosed with descemetocele and a stromal ulcer in the same eye and the other was diagnosed with an ulcer in each eye, one perforated ulcer and a descemetocele.
For Mezzadri V, et al. [5] the ulcer that extends deeper into the corneal stroma usually involves a secondary microbial infection that initiates stroma destruction. A bacterially infected corneal ulcer, although some of the collagen loss is caused by enzymes released by the bacteria, the enzymes released to confer invasive innate immunity contribute significantly to the loss of corneal tissue. It is this response that can lead to greater fibrosis, as well as other tissue changes that can decrease ocular function, according to Gelatt KN, et al. [2] It was observed in the dogs of this study, momentary visual loss due to active inflammation, since, after the procedure for the treatment of the ulcer, despite the corneal edema, the patients were visual.
For Gelatt KN, et al. [2] the sensitivity of the cornea in dogs, measured by the Cochet-Bonnet esthesiometer and by the histology of the corneal nerves, was higher, intermediate and lower in the dolichocephalic, mesocephalic and brachycephalic skull types, respectively. In this study, there was a prevalence of brachycephalic dogs, totaling 70% of cases, against 20% mesocephalic and 10% dolichocephalic. The most common causes of corneal ulcers in dogs include trauma, foreign bodies, infection, inadequate tear secretion, corneal dysfunction, spontaneous, toxic and anatomical/functional anomalies, according to Gogova S, et al. [3] Corroborating with the author, the cases in this study had the following histories: 7 out of 10 dogs have abnormal cranionasal conformation; 2 out of 10 dogs correspond to inappropriate tear secretion (CCS); 2 out of 10 dogs have corneal endothelial dysfunction, showing corneal degeneration; 1 out of 10 dogs was found to have ectopic eyelashes; 5 out of 10 dogs had nothing in their history, however, 3 of these 5 cases are from brachycephalic breeds, which with prominent eyes are predisposed to ulcers; the other two cases had no definite cause (Table 2).
| Race | Sex | Age | Affected Eye | Historic | Corneal Involvement (%) | |
|---|---|---|---|---|---|---|
| 1 | Australian Shepherd | Female | 4 years | OE | - | Aprox. 99% |
| 2 | English Bulldog | Male | 2 years | OE | CCS | 100% |
| 3 | Shih Tzu | Male | 13 years | OD e OE | Corneal degeneration | 100% OD, Aprox. 99% OE |
| 4 | French Bulldog | Male | 10 years | OE | Aprox. 99% e 60% a 75% | |
| 5 | Hungarian Pointer | Male | 11 months | OD | - | Aprox. 95% |
| 6 | Beagle | Female | 15 years | OE | Corneal degeneration and cataracts | Aprox. 99% |
| 7 | Boston Terrier | Male | 10 years | OD | - | 50% a 65% |
| 8 | Pekingese | Male | 9 years | OE | CCS | Aprox. 70% |
| 9 | American Bully | Female | 2 years | OE | Entropion | 50% a 60% |
| 10 | English bulldog | Female | 2 years | OE | - | Aprox. 99% |
Table 2: The table was Divided into 7 Specifications, Containing the Number of Cases, Race, Gender, Affected Eye, with Le for Lef
Table 2: The table was Divided into 7 Specifications, Containing the Number of Cases, Race, Gender, Affected Eye, with Le for Left Eye And Re for Right Eye; History, and How Much of the Cornea was Compromised According to Its Extension, and those that Resulted in Involvement of Up to 95% are Stromal Ulcers; Approximately 99% Were Descemetoceles; And 100% Perforated Ulcers. Dog 4 Had Two Ulcers in The Same Eye.
In a study carried out by Gelatt KN, et al. [2] dogs with nasal folds were almost 5 times more likely to be affected by corneal ulcers than those without, and brachycephalic dogs (craniofacial ratio< 0.5) were 20 times more likely to be affected than non-brachycephalic dogs. As shown in Table 2, the prevalence of brachycephalic dogs in this study can be observed, corresponding to 70% of the cases.
Corneal integrity is most readily assessed with fluorescein stain. Fluorescein dye is hydrophilic and readily binds to exposed corneal stroma if an ulcer is present, but the dye does not bind to intact healthy corneal epithelium or Descemet’s membrane and endothelium, per Gelatt KN, et al. [2]. All cases had the cornea stained with fluorescein dye for definitive diagnosis and better visualization of the ulcer during the performance of the biomicroscopy examination.
According to Table 2, the left orbit (LE) was the most affected, with 80% of the dogs in this study affected in this eye. However, no study found a correlation with a greater predisposition when compared to the right eye (OD).
The most common clinical signs seen in the cases of this study were: blepharospasm, suggesting ocular pain, epiphora, photophobia, hyperemic sclera, active inflammation of the anterior segment (uveitis), corneal edema and aqueous flare. In consensus with Neto S, et al. [4] the loss of corneal transparency is a common clinical sign and can be caused by the presence of inflammatory cell infiltration, mild or intense edema, depending on the depth. Prior to the procedure, 60% of the patients in this study had impaired vision due to the presence of uveitis and/or corneal edema (Figures 1 & 2), with loss of visual reflexes shown in Table 1. The diagnosis of corneal ulcer was made on the basis of clinical signs and retention of topically applied fluorescein dye by the corneal stroma.
The factors that support the transparency of the normal canine cornea include the absence of blood vessels and pigment, the absence of keratinization of the anterior surface epithelium, a well-organized stromal collagen network and the small diameter of the collagen fibrils, and when there is a change in this pattern, the color of the cornea and the vision are altered, as can be seen in Figure 1 and results in Table 1.
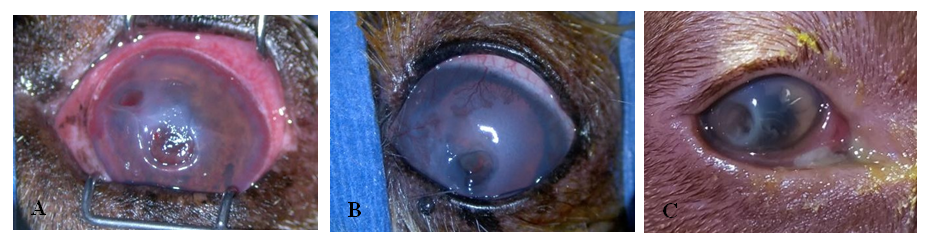
Source: Personal Collection. Figure 2: (A) English Bulldog Showing two Corneal Ulcers (LE), one Nasal Descemetocele, with Approximately 99% Involvement and one Dorsonasal Stromal Ulcer, with Approximately 50-75% Involvement of the Cornea. (B) Shih Tzu Presenting a Perforated Ulcer in the Central Cornea (LE), With 100% Involvement. (C) Hungarian Arm Showing Paracentral Lateral Stromal (OD) Corneal Ulcer, with Approximately 95% Involvement.
For tutors who choose not to undergo surgical treatment, intensive topical/systemic drug treatment is an option, however, not recommended. The corneal stroma has a limited capacity for regeneration and, when successful, corneal healing by secondary intention can induce a fibrovascular response causing excessive scarring of the affected site. Therefore, as drug treatment is often insufficient for the effective and rapid repair of a deep corneal defect, or when there is a corneal perforation, surgery is considered the initial gold standard treatment, according to Gogova S, et al. [3].
For Maggs DJ, et al. [1] conjunctival grafts are the gold standard treatment, as they preserve corneal and ocular integrity, replace lost corneal tissue and provide vascularization, since there is no blood supply from the cornea. There are at least 5 types of conjunctival grafts, the main ones being described: island or free, complete or 360º grafts, advancement or hood flaps, rotational pedicle and bridge.
The pedicled graft created from the bulbar conjunctiva is the graft most used by veterinary ophthalmologists, and this was the type chosen for the present study, which can be seen in Figure 3. The advantages described by Gelatt KN, et al. [2] are the vision is maintained while the graft is in place, the technique is performed to cover any part of the cornea, the graft moves in relation to the globe and no tension is created with the movement of the eyelid, and being able to perform the application of topical medication. It was recommended to patients with the aim of providing rapid healing and maintaining preserved vision, since the cornea is a segment that does not have a blood supply, and therefore, its healing is slow even with antibiotic therapy, and in the case of easily ruptured ulcers, it can lead to loss of vision by compromising the posterior segment, and even in enucleation.
That said, it was possible to observe that there was relevance with the author according to the results of this study. Grafts were performed in different locations on the cornea, the graft remained mobile with the movement of the conjunctiva and there were no cases of dehiscence (Table 1). It was also possible to carry out the entire drug prescription through the topical route, in this way the graft absorbs more easily, being an important coadjuvant in the healing of the graft. In addition, the graft is visible, the tutor can have a complete view and follow the progression of the case’s improvement. According to Gelatt KN, et al[2] preparation of the ulcer site is important for graft retention. Necrotic and collagenolytic corneal stroma should be debrided with a scalpel blade. Often, a partial-thickness keratectomy is indicated to remove necrotic tissue. Sutures should be placed in healthy corneal stroma to prevent graft dehiscence. Grafts do not adhere to the corneal epithelium; therefore, if corneal epithelium is present at the edge of the wound, it should be excised with a scalpel blade. All procedures in this study involved debridement of the necrotic epithelium with the aid of a Beaver scalpel nº64 (Figure 2).
![Figure 3: The advantages described by Gelatt KN, et al. [2] are the vision is maintained while the graft is in place, the technique is performed to cover any part of the cornea, the graft moves in relation to the globe and no tension is created with the movement of the eyelid, and being able to perform the application of topical medication. It was recommended to patients with the aim of providing rapid healing and maintaining preserved vision, since the cornea is a segment that does not have a blood supply, and therefore, its healing is slow even with antibiotic therapy, and in the case of easily ruptured ulcers, it can lead to loss of vision by compromising the posterior segment, and even in enucleation.](/fulltextimages/10709/fig_3.png)
Source: Personal Collection Figure 3: Necrotic Stroma Being Debrided and Carefully Removed to Receive the Conjunctival Graft. Source: Personal Collection.
Grafts must be wide enough to maintain an adequate blood supply and the base must be wider than the tip to avoid graft retraction (Figure 3). Tenon’s capsule must be dissected from the substance propria, as the graft must be thin enough that the tips of the scissor blades can be seen through it. The graft tissue must also be sufficiently loose so that, when positioned over the corneal lesion, it does not retract. That said, all procedures were performed according to the technique and guidance by Gelatt KN, et al. [2].
According to Gogova S, et al. [3] corneal vascularity was determined to be one of the most important risk factors for graft rejection. Theoretically, this risk is not present in corneal conjunctival grafts, since the grafted corneal and conjunctival tissues are autologous. In addition, conjunctival and lymphatic vessels offer significant antibacterial, antifungal, antiviral, antiprotease, and anticollagenase effects, which are rapidly incorporated into the corneal ulcer bed, aiding in the healing process. With the administration of systemic antibiotics, and concomitantly with the conjunctival blood vessels, they can reach the ulcer site at higher levels, accelerating the healing process.
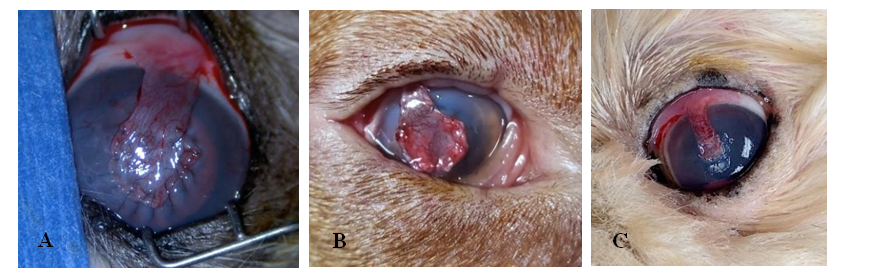
Source: Personal Collection. Figure 4: (A) Shih Tzu in the Immediate Postoperative Period, Showing a Pedicled Graft in the Central Cornea (LE). Note the Pinkish Graft. It is Possible to Observe Active Inflammation in the Epithelial Cornea and Intraocular Edema, Presenting a Cloudy and Bluish Cornea. (B) Hungarian Arm in the Immediate Post, with Pedicled Graft in the Paracentral Lateral Cornea (OD). Note the Active Episcleral Vessels and The Pinkish Graft. There is Edema in the Anterior Chamber. (C) Pekingese in the Immediate Post-Operative Period, Showing a Pedicled Graft in the Central Cornea (LE). Note the Pink Graft and Edema in the Anterior Chamber.
All patients in this study had active blood vessels in the cornea, heading towards the ulcer, demonstrating a viable graft, and ulcer healing being effective, since the blood supply is of paramount importance for stromal repair in cases of ulcers deep. The vessels were seen in greater numbers, mainly in the return visit, 15 days after the procedure.
Regardless of the primary cause of the ulcer, disruption of the epithelium predisposes the corneal stroma to infections, leading to rapid progression through the cornea and delayed healing. In this case, the globe and vision are threatened by the rapid degradation process of the cornea, and therefore, it is necessary to use antibiotics together after the placement of the conjunctival graft. The combination of three drugs, resulting in the “triple antibiotic”, is well tolerated by the ocular region and provides a broad spectrum of activity, the combination of Neomycin, Polymyxin and Gramicidin (topic NeoPoliGram), is a good example in this case, according to Maggs DJ, et al. [1] This combination was prescribed to 2 of the 10 patients in this study, along with oral Doxycycline.
The class of Cephalosporins and Fluoquirolones, are also indicated for the treatment of these ulcerations, both classes have bactericidal action and broad action, against gram-positive and gram-negative bacteria, respectively, and can be used concomitantly with the Tetracyclines class in oral formulations , which have broad spectrum and bacteriostatic action. In this study, 8 of the 10 dogs received this prescription, the drugs of choice being Ofloxacin (Fluoquirolone) and Terramycin (Oxytetracycline), both of which are topically presented, associated with Doxycycline (Tetracycline) in oral formulation.
According to Maggs DJ, et al. [1] the class of Tetracyclines are considered broad-spectrum antibiotics with bacteriostatic and immunomodulatory effect, capable of inhibiting the protein synthesis of microorganisms, and protecting against apoptosis and tissue destruction mediated by proteinases, preventing the deep ulcer, also becomes a “melting” ulcer, with destruction of collagen and softening of the cornea, which would make the graft unfeasible. Oral administration, in this case Doxycycline, produces more notable concentrations of its action than topical use. The organisms Stapylococcus, Pseudomonas and Proteus spp., are generally resistant to this class, however, Ofloxacin and Terramycin, which are used associated, have a spectrum against the mentioned organisms. Fluorchirolones are broad-spectrum bactericides, inhibiting DNA gyrase, that is, the multiplication of organisms. It has excellent penetration into the cornea, and is mainly recommended for deep and rapidly progressive corneal ulcers, such as those seen in the present study.
Stimulation of the corneal nerves can produce significant ulcer reflex anterior uveitis with painful spasm of the ciliary body and in these cases Atropine 1% in ophthalmic solution is recommended. However, when corneal ulceration occurs as a sequel to CCS, local administration should be used judiciously and only for as long as necessary to treat the concomitant uveitis, because it causes cyclopsia. In this study, Atropine 1% was prescribed for only two patients, who had the diagnosis of perforated ulcer, and had anterior uveitis and exacerbated painful stimuli. One of them has a positive diagnosis of CCS, therefore, its use was strict for the first 15 days after the procedure, being prescribed only twice a day (BID) and concomitantly with a lubricating gel, Optixcare.
Topically administered NSAIDs may delay the healing process, but systemic administration is safe and beneficial for reducing uveal inflammation and painful stimuli. Its administration must be judicious, since it can delay the entry of blood vessels into the cornea, which are necessary for the healing process of the ulcer. Following this, the patients in this study were prescribed Carprofen orally, twice a day (BID), which did not interfere with the results of the technique. After the negative diagnosis of ulcer in the returns, 7 of the 10 dogs received Diclofenac topically, to reduce edema and inflammation.
Corticosteroids are beneficial in the treatment of anterior uveitis, but they decrease leukocyte migration and depress macrophage phagocytosis. Depression of the ingestive capacity of monocytes and macrophages can result in changes in the number of receptors on their cell membranes and a decreased activation of macrophages. As a result, corticosteroids can potentially activate or exacerbate bacterial, viral, or fungal eye infections and are generally considered contraindicated in most eye infections Gelatt KN, et al. [2].
The dogs in this report made use of corticosteroids strictly after confirmation of complete healing of the ulcer, and it was used in the prescription of only 3 dogs in this study, which had exacerbated anterior uveitis. EIA selection and frequency of administration are variable according to the severity and location of the inflammation. Therapy was continued at a reduced frequency for several days to weeks after signs of ocular inflammation resolved, as premature discontinuation of medication can lead to a relapse of inflammation. The dogs that received this type of anti-inflammatory used Dexamethasone topically, varying between BID and TID.
Proper use of antibiotics is essential to stop the bacterial infection and not run the risk of new contamination, which would make the graft unfeasible and could lead to perforation and possible enucleation. I emphasize that, for a completely effective treatment, the tutor plays a crucial role in the evolution of the success of the technique, contributing with the correct use of medications and Elizabethan necklace. At the same time, the primary cause of the ulcer must be identified and treated. In the present study, 5 were the causes identified as primary, being CCS (20%), corneal degeneration (20%) and ectopic eyelashes (10%), all dogs received the appropriate treatments for their resolution.
According to the data gathered in this study, 80% of the dogs that underwent the conjunctival pedicle graft procedure had the ulcer completely healed within 15 days after the procedure (Figure 4). The other 20% in a first follow-up had the ulcer still present, but with ongoing healing, the use of antibiotics being maintained and a new return scheduled in 15 days. In this new visit, the ulcer was completely healed (Table 2), demonstrating an effective approach in the treatment of deep and/or perforated ulcers in 100% of the cases in this study.

Source: Personal Collection. Figure 5: French Bulldog, Shih Tzu and Pekingese Patients with Pedicled Graft in the Central Cornea After 15 Days of the Procedure, Respectively. It is Possible to Observe A Healthy Graft, With A Lighter Color and with the Sutures Being Well Absorbed By the Cornea. All Patients had the Ulcer Already Healed. Note the Cornea of the Dogs in Images A And B Showing A Bluish and Blurred Color, Due to Edema of the Anterior Chamber.
Upon return, 15 days after the procedure, it was possible to notice the improvement in the patients’ vision. According to the results displayed in (Table 2), 4 dogs (40%) that previously were not showing visual reflexes, presented in the return, these being the palpebral reflexes the threat and the light. 6 dogs (60%) were unable to visualize the pupillary reflex, due to the presence of edema, which is considered normal after the procedure, due to active inflammation in the cornea. Despite the presence of edema, I emphasize that, 100% of the dogs, had visual reflexes in the return, that is, it was possible to preserve the vision of all the cases after the pedicled conjunctival graft, those that had previously lost due to the ulcer, managed to recover after procedure.
After the following weeks, months, the sutures are completely absorbed and the conjunctival graft is adhered to the cornea in the region where the lesion was located, and the blood supply is being dissipated, in this way, the tissue becomes increasingly transparent, but it will always be possible to visualize it (Figure 5).

Source: Personal Collection. Figure 6: Dog with Pedicled Conjunctival Graft (OD) 3 Months after the Procedure for the Treatment of a Descemetocele. Anterior Chamber Intact, with No Active Inflammation or Edema. It is Possible to Observe the Graft From A Light to Transparent Color and Completely Adhered to the Cornea. Source: Personal Collection.
The pedicled conjunctival graft is considered one of the best techniques for cases of corneal perforation. However, graft dehiscence can occur, and this is related to the following causes: incomplete corneal debridement, leakage of aqueous humor, excessive tension, pedicle angulation greater than 45º in relation to the vertical axis, presence of melting and large lesions, according to Ramos RMT, et al[6] In this study, there were no cases of dehiscence, as can be seen in the results in Table 1. The sutures of the grafts were being well absorbed, the grafts were healthy and were incorporating well into the cornea (Figure 4).
According to Gelatt KN, et al. [2] the graft can be excised from 8 weeks after the procedure. for Maggs, DJ et al. [1] regression and hypoperfusion of corneal vessels that spontaneously grew from the limbus are usually a reliable sign that vascular support from the graft is no longer needed. In disagreement with the cited authors, the grafts were not excised, they are left permanent, with the intention of not ceasing the blood supply to the cornea, so that in cases of a new ulcer, this can contribute to healing.
Conclusion
There was a prevalence of 70% of brachycephalic races affected in the study, confirming the predisposition to acquire this type of ulcer.
The conjunctival graft provides blood supply, replaces the lost corneal tissue and maintains the integrity of the cornea, since the vision of the dogs was preserved after the procedure. The effectiveness of the pedicled conjunctival graft was verified for the treatment of deep and perforated ulcers in this study, since there was complete healing of the ulcer in 100% of the cases, during the period of 30 days.
References
-
Maggs DJ, Miller PE, Ofri R (2016) Slatter’s fundamentals of veterinary ofthalmology. 6th (Edn.), Elsevier Saunders, Gainesville FL, USA.
-
Gelatt KN, Shlomo GB, Gilger BC, Hendrix DVH, Kern TJ, et al (2021) Veterinary ophthalmology. 6th (Edn.), John Wiley & Sons, Hoboken, USA.
-
Gogova S, Leiva M, Ortillés A, Laguna F, Crasta M, et al. (2020) Corneoconjunctival transposition for the treatment of deep stromal to full-thickness corneal defects in dogs: A multicentric retrospective study of 100 cases (2012-2018). Vet Ophthalmol 23(3): 450-459.
-
Neto S, Da FX (2020) conjunctival coverage in the treatment of melting ulcerative keratitis in a brachycephalic dog 30 f. Center for Agricultural Sciences - Federal University of Paraíba.
-
Mezzadri V, Crotti A, Nardi S, Barsotti G (2021) Surgical treatment of canine and feline descemetoceles, deep and perforated corneal ulcers with autologous buccal mucous membrane grafts. Vet Ophthalmol 24(6): 599- 609_._
-
Ramos RMT, Rodrigues LMN, Passos YDB, Palácio L da P (2019) Pedicled conjunctival graft in the surgical treatment of ocular perforation in a canine patient. Science animation (Print) 29(S3): 41-44
-
Silva Dias AI DA (2017) Ocular emergencies in small animals retrospective study of 72 cases Integrated master’s thesis in veterinary medicine. Veterinary Medicine.
-
Bertolino BF, Junior AZ, Tamehiro CY, Zacarias FG da S, Blaschi V (2022) Study of biological membranes for repair of corneal lesions in dogs and cats. Brazilian Journal of Development Flight 8(8): 2002.
-
Capacchi DC (2017) Biological membranes in the cornea of dogs and cats, Veterinary Medicine - Federal University of Rio Grande do Sul.
-
Gelatt KN, Gelatt, JP, Plummer C (2021) Veterinary ophthalmoly surgery. 2nd (Edn.), Elsevier Saunders, Gainesville, FL, USA (2011).
-
Guyonnet A, Desquilbet L, Faure J, Bourguet A, Donzel E, et al. (2020) Outcome of medical therapy for keratomalacia in dogs. Journal of Small Animal Practice, J Small Anim Pract 61(4): 253-258.
-
Guyonnet A, Desquilbet L, Faure J, Bourguet A, Donzel E, et al. (2020) Outcome of medical therapy for keratomalacia in dogs, Journal of Small Animal Practice, 61(4): 253-258.
-
Lacerda RP, Gimenez MTP, Laguna F, Costa D, Ríos J, et al. (2017) Corneal grafting for the treatment of full- thickness corneal defects in dogs: a review of 50 cases. Veterinary Ophthalmology Vet Ophthalmol 20(3): 222- 231
-
Laignier CS, Nunes Neto OG, Silva Melo KP DA, lira IP, Oliveira SS, et al. (2022) Deep ulcerative keratitis in a canine – case report. Brazilian Journal of Development. Flight 8(1): 2022.
-
Lobo TV, Fayad AR, Lima AMV, Sant’Anna ARM (2021) The cornea and ulcerative keratitis in dogs: a review of anatomy, etiopathogenesis and diagnosis. Biosphere Encyclopediav 18(36): 17.
-
Moreira ARL (2015) Feline corneal sequestration: a retrospective study. University of Lisbon. College of Veterinary Medicine.
-
Muphy CJ, Samuelson DA, Pollock RVH (2012) Miller’s Anatomy of the dog (4th ed.). Chapter 21: The eye. 746- 785. Elsevier Saunders, Gainesville FL, USA.
-
Sá MEA, De B (2016) Ophthalmic antibiotic therapy on the ocular surface of dogs ill. Agronomy and Veterinary Medicine-University of Brasília, DF, Brazil.
-
Sampaio HM, Gomes MC, Costa PPC, Melo MS (2016) Descemetocele with “melting” edges in a brachycephalic dog – case report. Journal of Veterinary Science and Public Health 3(2): 137-142.
-
Silva KF (2019) Occurrence of Corneal Ulcer in Canines: Retrospective Study of 310 Cases. Medicina Veterinary - Federal University of Uberlândia, Brazil.
-
Vilela DPA (2019) Etiology of Corneal Ulcers In Dogs- Retrospective Study of 69 Clinical Cases University of Lisbon, Faculty of Veterinary Medicine.
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework
- Hymenoptera Specimens from the Caño Negro Wetland, of the National Museum Collection, Costa Rica
- Science 4.0: Comprehensive Architecture of the Biological Operating System (Bio-OS) A Framework for Systemic Resilience and Industrialized Bio-Governance
- Rabbit on, or Hare Back? Understanding Climate Change
- Clinical Validation of Science 4.0: Flow Steering and Epigenetic Drift Inversion on a 76-Year-Old Hybrid System
- Seeds Planted by another Mind