Tibiotarsus Osteosynthesis Using Tie-in in Blue-Fronted Amazon Parrot (Amazona aestiva)-Case Report
In avian orthopedics, various conservative and surgical techniques are reported for fracture treatment, with the choice of an appropriate osteosynthesis technique being challenging due to the biological, mechanical, and clinical aspects of each species. Within this context, the objective of the present study is to report the use of Tie-in fixation in the treatment of a distal diaphyseal tibiotarsus fracture in a Blue-fronted Amazon parrot (Amazona aestiva). The bird was presented with a history of trauma due to a fall and radiographic examination revealed a complete, oblique fracture in the distal third of the right tibiotarsus. Osteosynthesis was performed by an open fracture reduction and normograde insertion of a Kirschner wire into the tibiotarsus. Subsequently, three additional Kirschner wires were inserted as a Type II external skeletal fixator. A external bar made of polymethylmethacrylate (PMMA) was used to connect the intramedullary pin with the external fixator. Fracture healing progression was monitored by radiographs at 21, 35, and 48 days postoperatively. By day 35, bone callus formation and early remodeling were observed, prompting implant removal. It was concluded that the treatment was appropriate for the patient, with biological, clinical, and mechanical factors contributing to the success of the therapy.
Introduction
In avian medicine, orthopedic conditions are common, occurring in both birds under human care (pets, zoo birds, breeding stock, or production birds) and wild birds [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. Various conservative and surgical techniques are reported for the treatment of fractures in birds, with the selection of the most appropriate technique posing a challenge due to the biological, mechanical, and especially clinical aspects of each species [12, 14].
The tibiotarsus is one of the most important long bones in the biomechanics of pelvic limb movement in birds and is frequently affected by traumatic injuries [1]. Thus, the treatment of tibiotarsal fractures in birds can be performed conservatively or surgically, with the animal’s size being a determining factor in the choice of orthopedic treatment [4, 10]. Among the implants indicated for the treatment of tibiotarsal fractures in birds, lightweight implants—either external or internal—are recommended, including the use of intramedullary pins (IMPs) and/or external skeletal fixators (ESFs) [6, 9, 8].
When the ESF is interconnected with an intramedullary pin through the use of an external connecting bar, a hybrid fixation known as Tie-in is established. This technique may represent a promising option for stabilizing long bone fractures in birds [1, 3]. In this context, the present study aims to report the use of Tie-in external skeletal fixation for the treatment of a distal diaphyseal fracture of the tibiotarsus in a Blue-fronted Amazon parrot (Amazona aestiva).
Case Report
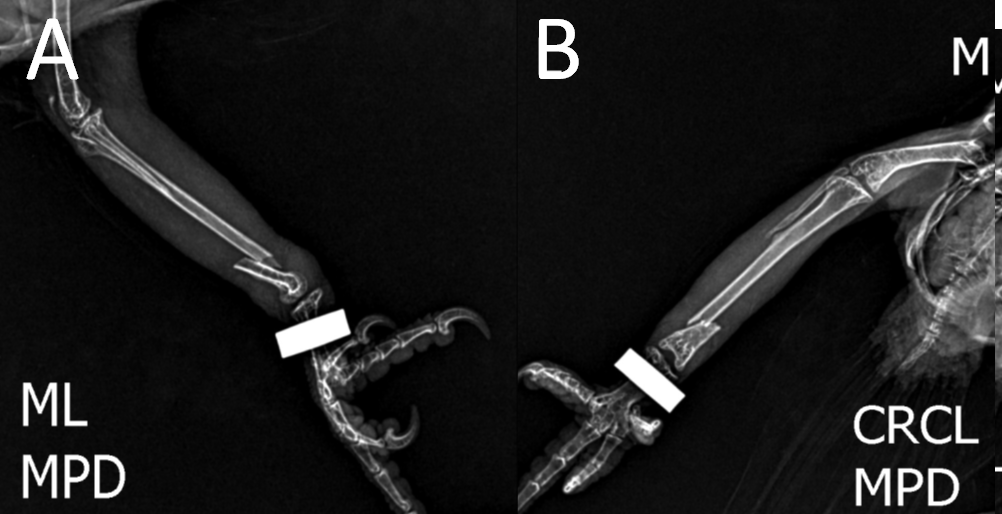
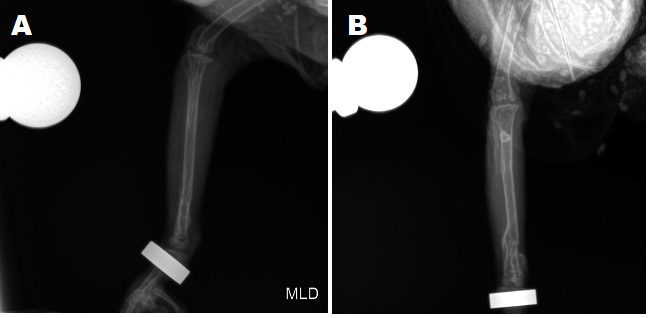
A two-month-old, 330-gram (g) pet Blue-fronted Amazon parrot (Amazona aestiva) presented with a history of trauma due to a fall. Physical examination revealed functional impairment of the limb, angular deviation, hematoma, pain, and swelling in the distal region of the right tibiotarsus, as well as local crepitation. Following sedation with isoflurane to effect and analgesia with butorphanol (1 mg/kg), radiographic examination in two orthogonal projections (craniocaudal and mediolateral) confirmed a complete, short oblique fracture in the distal third of the right tibiotarsus (Figure 1).
Treatment was initiated with analgesic therapy using butorphanol (1 mg/kg, BID, IM, for 9 days), dipyrone (25 mg/kg, TID, PO, for 15 days), and meloxicam (0.5 mg/kg, SID, IM, for 7 days), combined with comfort stabilization through a preoperative Robert Jones bandage for the osteosynthesis of the right tibiotarsus.
After four days of stabilization and analgesia, the surgical osteosynthesis procedure was performed. Pre- anesthetic medication was administered intramuscularly with butorphanol (1 mg/kg), followed by venoclysis of the ulnar vein using a 26G catheter. Anesthetic induction and maintenance were achieved with isoflurane inhalation to effect, vaporized in 100% oxygen using a Baraka system with a calibrated vaporizer. After induction, a femoral perineural block guided by a peripheral nerve stimulator was performed using lidocaine (4 mg/kg) without a vasoconstrictor in the right pelvic limb.
With the patient in dorsal recumbency, feathers were removed from the medial femur to the distal tibiotarsus region. Antisepsis was performed using 70% alcohol and 4% chlorhexidine in the area. For osteosynthesis, a medial approach to the distal tibiotarsus near the fracture site was made, involving retraction of the gastrocnemius and adjacent muscles. The fracture was then openly reduced, exposing the proximal and distal fragments.
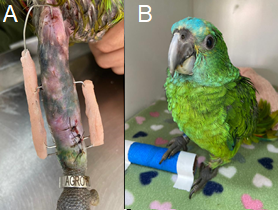
A 0.8 mm Kirschner wire was inserted normograde into the medullary canal of the tibiotarsus, achieving reduction and initial stabilization of the fracture. Subsequently, three 0.8 mm Kirschner wires were placed in a Type II external skeletal fixator arrangement: one in the proximal diaphyseal region and two distal to the fracture site. A small external bar made of polymethylmethacrylate (PMMA) was then constructed, connecting the intramedullary pin to the external fixator to achieve the Tie-in configuration (Figure 2A).
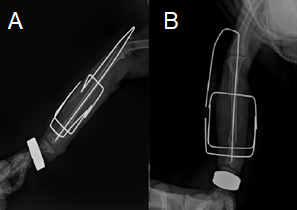
Local dermorrhaphy was performed using 4-0 monofilament nylon with simple interrupted sutures. Postoperative management included radiographic control at 24 hours (Figures 3A & 3B), which demonstrated appropriate alignment and fracture apposition of the tibiotarsus with a minor displacement of the tarsal bone in the distal region, without any functional impairment. During the postoperative dressing change, early functional recovery of the limb was already evident (Figure 2B).
Treatment was initiated with analgesic therapy using butorphanol (1 mg.kg⁻¹, BID, IM, for 9 days), dipyrone (25 mg.kg⁻¹, TID, PO, for 15 days), and meloxicam (0.5 mg.kg⁻¹, SID, IM, for 7 days), combined with comfort stabilization through a preoperative Robert Jones bandage for the osteosynthesis of the right tibiotarsus.
After four days of stabilization and analgesia, the surgical osteosynthesis procedure was performed. Pre- anesthetic medication was administered intramuscularly with butorphanol (1 mg.kg⁻¹), followed by venoclysis of the ulnar vein using a 26G catheter. Anesthetic induction and maintenance were achieved with isoflurane inhalation to effect, vaporized in 100% oxygen using a Baraka system with a calibrated vaporizer. After induction, a femoral perineural block guided by a peripheral nerve stimulator was performed using lidocaine (4 mg.kg⁻¹) without a vasoconstrictor in the right pelvic limb.
With the patient in dorsal recumbency, feathers were removed from the medial femur to the distal tibiotarsus region. Antisepsis was performed using 70% alcohol and 4% chlorhexidine in the area. For osteosynthesis, a medial approach to the distal tibiotarsus near the fracture site was made, involving retraction of the gastrocnemius and adjacent muscles. The fracture was then openly reduced, exposing the proximal and distal fragments.A 0.8 mm Kirschner wire was inserted normograde into the medullary canal of the tibiotarsus, achieving reduction and initial stabilization of the fracture. Subsequently, three 0.8 mm Kirschner wires were placed in a Type II external skeletal fixator arrangement: one in the proximal diaphyseal region and two distal to the fracture site. A small external bar made of polymethylmethacrylate (PMMA) was then constructed, connecting the intramedullary pin to the external fixator to achieve the Tie-in configuration (Figure 2A). Local dermorrhaphy was performed using 4-0 monofilament nylon with simple interrupted sutures. Postoperative management included radiographic control at 24 hours (Figures 3A & 3B), which demonstrated appropriate alignment and fracture apposition of the tibiotarsus with a minor displacement of the tarsal bone in the distal region, without any functional impairment. During the postoperative dressing change, early functional recovery of the limb was already evident (Figure 2B).
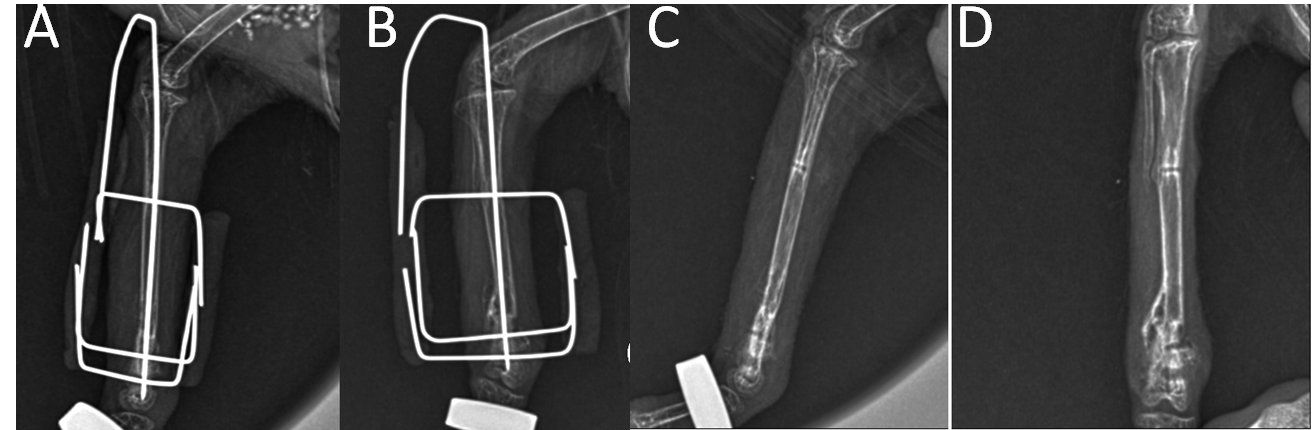
The progression of bone consolidation was monitored through mediolateral and craniocaudal radiographs at 21, 35, 48, and 91 days postoperatively. From the first follow-up at 10 days for dermorrhaphy suture removal, the patient was active, exhibited mobility in the affected limb, and showed no noteworthy changes near the implant sites. At 35 days, the presence of callus formation and the onset of remodeling were observed, prompting the recommendation for implant removal. The skin at the implant insertion sites showed minor crust formation, which was clinically insignificant. At 48 days postoperatively, the implants were removed, and the patient was discharged for physical activities (Figure 4). At this time, meloxicam (0.5 mg/kg, IM) was administered, and dipyrone (25 mg/kg, PO, BID) was prescribed for 3 days.
At 91 days postoperatively, a follow-up surgical review was conducted for radiographic evaluation and clinical discharge of the patient (Figure 5). Radiographic examination revealed proper consolidation of the tibiotarsus with the presence of a callus in the distal third, leading to the patient’s discharge.
Discussion
The patient in this report demonstrated good progression with the use of the Tie-In hybrid fixator. According to studies, the use of external skeletal fixation (Type II) is relatively well-tolerated by animals, promoting early ambulation and preventing muscle atrophy, as observed in this case [15]. The use of hybrid fixators, such as the Tie-In, where the intramedullary pin is connected to the external fixator, offers advantages such as reduced intramedullary pin migration, lightweight construction, and the possibility of dynamization [3, 8, 11]. This technique ensures proper bone alignment and prevents rotational forces on the fracture site.
Performing osteosynthesis techniques can be challenging due to implant weight, mechanical properties of the bones, and patient behavioral characteristics such as implant avulsion or pecking at external components [8]. As employed in this case, the Tie-In technique is particularly advantageous for birds due to their light and delicate bone structure and the dynamization potential of the implant. The intramedullary pin provides internal support, while the external Kirschner or Schanz wires add external stability, preventing fragment displacement and excessive mobility [3]. This promotes proper bone consolidation and allows for faster functional recovery, with young birds being more prone to early consolidation [7].
A relevant study supporting the choice of implants for this patient was conducted by Khan et al. (2015), who evaluated the effectiveness of Tie-In stabilization for tibiotarsus fractures in chickens. The results showed that Tie-In use facilitated fracture consolidation without deformity or functional compromise of the affected limb, resulting in high surgical success rates and rapid functional recovery. Similarly, the present case demonstrated early limb functionality and relatively rapid clinical and radiographic consolidation, likely associated with biological factors, effective analgesia, the bird’s high metabolism, and young age.
In this context, fracture consolidation in young birds is a complex process critical for adequate recovery after trauma. A bird’s ability to repair fractures depends on factors beyond age, including fracture location, bone type, and the extent of surrounding tissue damage [11]. In this patient, hard callus formation began approximately 20 days postoperatively;
however, the exact repair time in birds can vary considerably. The literature does not provide an exact timeframe applicable to the taxonomic group, but an estimate can be made based on general information about fracture consolidation in young birds from various studies [8].
A study by Stahl, et al. concluded that consolidation could take several weeks to months for complete resolution. Early restoration of normal pelvic limb function in birds minimizes potential complications such as muscle atrophy, limb contracture, and pododermatitis development [9]. In this case, limb functionality returned within 24 hours post- surgery, progressing gradually to full recovery. Hard callus formation in this patient’s tibiotarsus was observed in the first radiographic evaluation at 21 days postoperatively. Due to increased vascularization and bone metabolism in birds, osteogenesis occurs more rapidly, with healing often progressing within 21 days. Other studies, such as West, et al. report extensive cartilaginous callus formation as early as 15 days post-fracture. However, as in mammals, bone healing depends on several factors, including vascular integrity, infection presence, fragment displacement, and mobility at the fracture site [8].
In this patient, the remodeling process (bone cells replacing the repair tissue with new bone) began at 35 days, with progression observed in imaging up to 90 days postoperatively. However, bone remodeling can take several additional weeks or months following consolidation [2, 13]. Implant selection is a key determinant for successful consolidation, whether internal or external. For this case, a combination of an external skeletal fixator (ESF) and an intramedullary pin (IMP) using the Tie-In technique was selected.
According to the literature, fractures in parrots can be treated with external skeletal fixators, providing adequate stability and support for fractured bones during consolidation [1, 8]. This technique involves external devices such as pins or wires, bars, and/or rings secured to the bone using stainless steel or durable materials like polymethylmethacrylate, as used in this clinical case [1, 2]. The use of external skeletal fixators has proven effective in treating fractures in various bone regions, including the tibiotarsus, tarsometatarsus, humerus, and radius-ulna in parrots [1, 2, 8].
Among the potential complications of Tie-In use are infections and inflammation from pin insertion in soft tissues and implant rejection. Additionally, inadequate fracture stabilization can result in permanent bone deformity and functional impairment of the affected limb [1]. These issues were not observed in this patient. During the postoperative period, prophylactic meloxicam, a COX-2 selective nonsteroidal anti-inflammatory drug (NSAID), and an antibiotic from the quinolone class (enrofloxacin) were prescribed for five days.
Osteosynthesis procedures may warrant antimicrobial treatment for 7–10 days, particularly in cases involving transoperative contamination or complications with osteomyelitis risk, requiring treatment to extend to two weeks or more [8]. For this patient, antimicrobial treatment was advised due to soft tissue invasion by the Tie-In system and challenges in cleaning pin insertion sites, given the patient’s size and implant proximity.
Pre-, intra-, and postoperative analgesia is essential for treatment success and patient welfare. Multimodal analgesia, combining opioids and NSAIDs, was administered in this case. NSAIDs offer analgesic, anti-inflammatory, and antipyretic properties, frequently used for managing acute and chronic pain in birds. Commonly employed NSAIDs, such as meloxicam and carprofen, reduce pain and enhance welfare in birds undergoing surgical procedures [8, 11] as observed in this case.
In addition to NSAIDs, other analgesic strategies include opioid administration, local anesthetics, and nerve blocks, as performed in this case. Opioids like buprenorphine and butorphanol effectively control acute pain in birds, providing comfort and promoting early limb functionality, though dosage and administration intervals must be adjusted to avian physiology. For nerve block in this patient, lidocaine, a local anesthetic, was used to block pain conduction, employed during surgical procedures or as analgesic support. Nerve blocks, such as femoral or sciatic nerve blocks in avian pelvic limb surgeries, reduce pain effectively, as demonstrated in this case [5].
Conclusion
The use of a Tie-In external skeletal fixator for tibiotarsus fracture repair in a Blue-fronted Amazon parrot was appropriate, without surgical or postoperative complications, resulting in successful surgical outcomes and patient recovery. Biological, clinical, and mechanical factors, both pre- and postoperative, such as overall health, adequate nutrition, age, and care during the recovery period, play a significant role in bone consolidation and surgical success.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Aron DN, Foutz TL, Keller WG, Brown J (1991) Experimental and clinical experience with an IM pin external skeletal fixator tie-in configuration. Veterinary and Comparative Orthopaedics Traumatology. 4(3): 86- 94.
-
Alievi MM, Oliveira ANC, Ferreira PA, Traesel C, Guimarães LD, et al. (2008) Osteossíntese de úmero em pombos domésticos (Columba livia) associando-se pinos metálicos e polimetilmetacrilato intramedulares após osteotomia diafisária. Arquivo Brasileiro de Medicina Veterinária e Zootecnia. 60(4): 843-850.
-
Baniadam A, Jahany S, Khajeh A (2014) The ESF-IM Pin Tie-in Fixation in Multiple Fracture of Humerus in an Eagle. In: Proceeding of the 4th International Symposium of Veterinary Surgery-ISVS (Mashhad, Iran) pp: 143-145.
-
Ferrigno CRA, Schmaedecke A, Ferraz V (2014) Ortopedia. In: Cubas ZS, Silva JCR, et al. (Eds.), Tratado de Animais Selvagens: medicina veterinária. In: 2nd (Edn.), São Paulo: Rocca, Brazil, pp: 2095-2112.
-
Flecknell PA, Waterman-Pearson AE (2070) Pain management in animals. W.B. Saunders Company.
-
Gull JM, Saveraid TC, Szabo D, Hatt JM (2012) Evaluation of three miniplate systems for fracture stabilization in pigeons (Columba livia). Journal of Avian Medicine and Surgery 26(4): 203-212.
-
Guzman DSM, Bubenik LJ, Lauer SK, Vasanjee S, Mitchell MA (2007) Repair of a coracoid luxation and a tibiotarsal fracture in a bald eagle (Haliaeetus leucocephalus). Journal of Avian Medicine and Surgery 21(3): 188-195.
-
Helmer P, Redig PT (2006) Surgical Resolution of Orthopedic Disorders. In: Clinical Avian Medicine. Florida: Spix Publishing 1: 761-774.
-
Hollamby S, Dejardin LM, Sikarskie JG, Haeger J (2004) Tibiotarsal fracture repair in a bald eagle (Haliaeetus leucocephalus) using an interlocking nail. Journal of Zoo and Wildlife Medicine 35(1): 77-81.
-
Martin H, Ritchie BW (1994) Orthopedic surgical techniques. In: Ritchie BW, Harrison GJ, et al. (Eds.), Avian Medicine: principles and application. Florida: Wingers Publishing, Inc., pp: 1137-1169.
-
Piermattei DL, Flo GL, Decamp CE (2006) Handbook of Small Animal Orthopedics and Fracture Repair. In: 4th (Edn.), St. Louis, Missouri: Saunders Elsevier.
-
Tully TN, Divers SJ (2008) Manual of Exotic Pet Practice. In: 2nd (Edn.), St. Louis: Saunders.
-
Zafalon-Silva B (2019) Determinação do defeito crítico em ulna de codorna-doméstica (Coturnix coturnix japonica). Master’s degree dissertation, Programa de Pós-Graduação em Ciências Veterinárias, Universidade Federal do Rio Grande do Sul, UFRGS. Porto Alegre, pp: 49.
-
Zijlstra M, Redig PT (2001) Surgical anatomy of the avian orthopedic patient. Veterinary Clinics: Exotic Animal Practice 4(2): 297-317.
-
Zumbado VR, Graham JE, Waln ER (2011) External fixation of tibiotarsal fractures in birds of prey using carbon-fiber-reinforced polymer rod with stainless steel pins. Veterinary Surgery 40(4): 416-422.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework