Interest of Open Surgical Treatment in Trigger Fingers Resistant to Corticosteroid Injections (About 20 Cases)
Background: The aim of this study is to draw up the epidemiological profile of our patients, to estimate our results of the open resection of A-1 pulley and to show the interest of the surgical treatment in trigger fingers which are resistant to corticosteroid injections. Methods: It is a retrospective study made through the analysis of 20 exploitable files among several cases of trigger fingers, between January 2003 and October 2015. We included in our study patients aged of more than 18 years old, having symptoms dating of 6 months at least, and who have already benefited from at least one corticosteroid injection. Results: All our patients benefited initially from one or two injections. The use of surgery was indicated in the persistence of symptoms. The criteria of evaluation included the size of the skin incision, the pain, the residual symptoms, the satisfaction and the complications. The opening of the pulley A1 was done in all the patient cases, coupled with the premature active and passive mobilization, this was successful in all cases with satisfying Quick DASH score achieved after 3 months and 6 months postoperatively. Conclusion: The resection of A-1 pulley gives good results with an unimportant rate of complications and the surgical indication seems to be accepted when the symptoms persist after medical treatment by corticosteroid injection.
Introduction
The trigger finger is a stenosing digital tenosynovitis, most often involving a "catching" of the flexor tendon (s) in its sheath, usually at the A1 pulley [1, 2].
It is relatively common in middle-aged women around the fifth decade but it can sometimes touch children [2, 3, 4]. This pathology which predominates at the level of the thumb is mostly idiopathic [1]. It is often associated with pain and functional discomfort. The therapeutic modalities are different according to the teams but a large percentage of the trigger fingers are treated successfully by one or two injections of corticosteroids [2]. Surgical release is usually indicated when medical treatments have failed; thus, the opening of pulley A1 can be performed either open-pacedly or percutaneously or by endoscopic treatment [1, 3, 4]. The aim of this study is to establish the epidemiological profile of our patients and to evaluate and compare our results of open resection of the A1 pulley through a review of the literature.
Patients and Methods
We report a monocentric retrospective series made through the analysis of 20 usable records among several trigger finger cases admitted between January 2003 and October 2015. We have analyzed the records by using an operating card. We included in our study patients aged 18 years and over, having symptoms old of 6 months at least, and having already received at least one corticosteroid injection. Data collected was processed using Microsoft Office Excel software, and then validated for analysis by Epi info software (version 7).
Results
There were 16 women and 4 men, with an average age of 51.5 years (ranging from 18 to 85 years). The right side was affected in 12 cases (60%); whereas, the left side was affected in 8 cases (40%). 8 patients, that is 40 % of the cases had a professional activity at the time of surgery: 2 primary school teachers, 2 students, 1 patient exercising manual labor requiring precision (seamstress), a patient of manual labor requiring strength ( construction worker) and 2 drivers (truck, taxi). 12 patients, that is 60 % were unemployed (10 were housewives and 2 retired). The finger affected by the symptoms was thumb in 13 cases, middle finger in 2 cases, ring finger in 4 cases and the 4th finger in one case. The dominant hand was involved in 12 cases, and all patients were right-handed. The symptoms appeared averagely 2 years (1 to 4 years) before surgery. Four patients had pathological conditions which predisposed them to the occurrence of a trigger finger (Diabetes, hypertension, rheumatoid arthritis).
All the patients underwent surgery because of a typical symptomatology: 5 fingers had simple clings to movements, 11 fingers were blocked in flexion, which 8 of them were actively corrected and 3 others were passively corrected, 4 fingers were blocked in flexion with no possibility of correcting the deformation. The blockages were accompanied by pains for 12 fingers. A quick DASH (disability of the arm shoulder hand) questionnaire was used to assess the impact of pathology on daily activities (Table 1).
| Score | Percentage |
|---|---|
| score from 21 to 40 | 20% |
| score from 41 to 60 | 70% |
| score more than 61 | 10% |
Table 1: The quick DASH preop.
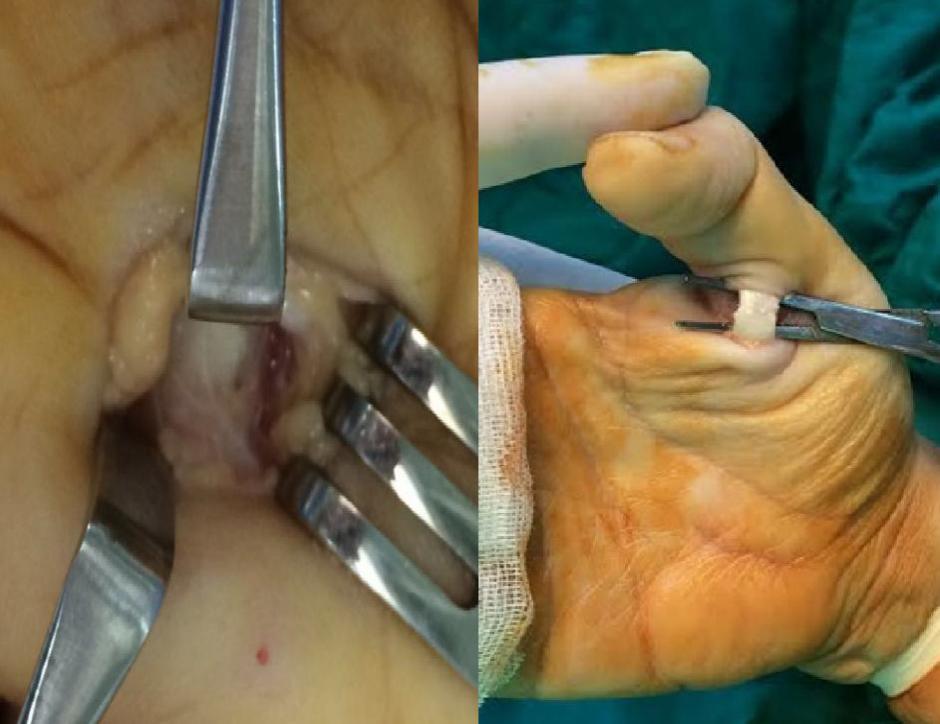
Table 1: The quick DASH preop. In our series, the opening of pulley A1 was carried out in all the patients, coupled with the early active and passive mobilization; this was successful in all cases (100% of cases). A transverse or oblique pathway was used when incising the pulley in all cases at the level of the distal palmar fold (Figure 1) and the size of the incision is on average 12 mm (extremes ranging from 10 to 18 mm).

We performed two types of gestures on the pulley A1: - A section of the pulley A1 was made 2 times (2 inches) approximately at 1 cm of the fibrous flexor tendon, the sheath being respected. A partial excision of the pulley A1 20 times (Figure 2).
mean follow-up of 24 months, the blocking was eliminated without recurrence for all patients, and no further treatment was performed. Besides, no residual pain was observed. Range of motion was measured in comparison with that of the same finger on the healthy contra-lateral hand. However, range of motion was normal. A patient with metacarpophalangeal osteoarthritis prior to follow-up surgery had persistent stiffness due to inadequate rehabilitation and physical therapy. Unfortunately, one patient presented cutaneous disunion due to the negligence when using the dressing and also due to his unbalanced diabetic ground and one patient retained a retracting bridle. No patient had a metacarpophalangeal joint flexion deformity (flessum) during the revision, and no patient had a distal sensory deficit. All patients resumed their regular activities after the 15th postoperative day with all patients reporting to their previous professions.
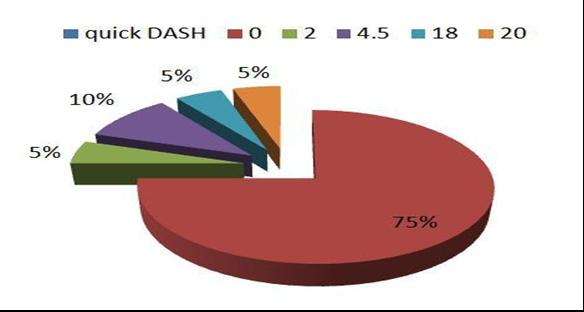
A quick DASH score was satisfactory at 3 months (Table 2) and at 6 months postoperatively (Figure 3). Finally, a subjective "survey on patient satisfaction" was carried out on patients’ impression on outcomes: are you "very satisfied", "satisfied", "averagely satisfied" or "not satisfied" with the treatment of your trigger finger? All patients were satisfied with the outcome of treatment.
| Score | Percentage |
|---|---|
| score at 11(*) | 80% |
| score from 12 to 20 | 15% |
| score from 21 to 40 | 5% |
Table 2: Evolution of the quick DASH at 3 months.
Discussion
The trigger finger is a pathology, which is often idiopathic, characterized by a locking of the flexor apparatus at the metacarpophalangeal level facing the pulley A1. Its frequency is estimated at 2.6% of the population. It is also the consequence of an inadequacy between the volume of the flexor tendons and that of the digital canal, mainly in its proximal part [2]. For some patients, the primum movens would be the thickening of the pulley A1 secondary to the repeated micro-trauma, with a deep fibrocartilaginous metaplasia of this pulley that is in chronic phase if we consider it from a histological point of view [5, 6, 7].
mucopolysaccharidoses, etc.) [4]. The patient may initially complain of pain when mobilizing his finger, or suffer from discomfort due to a sensation of trigger and / or a decrease in the complete mobility of the finger. The trigger may become painful, and can be localized by the patient and palpated by the practitioner (doctor). Its form is initially a small mobile nodule felt during the mobilization of the finger: in the palm, in metacarpophalangeal (MP) or interphalangeal joints (IP) [2]. In the most severe cases, the finger may remain locked in flexion or extension [2]. The diagnosis of the trigger finger is obvious and easy to pose by a simple clinical examination [2]. Complementary examinations are usually unnecessary. The main therapeutic methods used to heal the trigger finger are immobilization, corticosteroid injection and / or surgery. Concerning the modalities of surgical treatment, they are very varied [4, 8], according to the approach, and surgical technique and despite this diversity, they allow to obtain regularly good and lasting results [2]. Therefore, the modalities of surgical treatment are very varied: • According to the approach that may be longitudinal for Stefanich and Peimer [9] or transversal for Hodgkinson et al. [10], or punctiform with the percutaneous technique of Lyu [11];
• According to the technique of release that may be a simple opening for Bonnici and Spencer [12], or a resection for Thorpe [13], or plastic enlargement for Kapandji [11, 14]. Endoscopic surgery allows an endoscopic section of the pulley A1 by the introduction of an endoscope. This technique requires short postoperative rehabilitation and it is still poorly accessible financially [16].
The open-pole release of the A1 pulley has been used for over 100 years in the treatment of trigger fingers. Under a tourniquet, we make a complete opening of pulley A1 about 1.5 cm by using a short transversal incision upstream of the pulley A1, without opening the second pulley, that is to say close to the palmar flexion fold, and this, after having located and separated on each side the vasculo-nervous pedicle [10]. This simple opening of the pulley A1 does not cause any misalignment, but if the pulley A2 is also severed, the flexors will take a bowstringing form and cause an ulnar deviation of the finger, especially for the index finger [1]. The partial resection of pulley A1 is a method which consists of excising a rectangular fragment in the longitudinal direction of about 1 cm near the palmar flexion fold of the pulley A1 of the flexor tendon. It is a quick, non-painful move that is usually radical and definitive [2, 6]. The plastic enlargement of the metacarpophalangeal pulleys is a very delicate technique, which involves an oblique opening of the pulley A1, followed by a sliding between the two banks, and then we proceed to a closing of the pulley by a few Prolene 4-0 points (sutures, stitches) [2, 7, 11]. According to the literature: in the Marks series [10], a success rate of 91% is observed for patients treated with steroid injections. However, in the series of Lin et al [17], 84.9% of success is observed in percutaneous needle therapy and 94% of success is obtained in the use of a new percutaneous tenolysis technique in the Werthel, et al. series [18]. On the other hand, in the series of HA, et al. [19], a success rate of 93% was obtained by the use of percutaneous technique by tenotomy. Concerning the series of Hodgkinson, et al. [10], a success rate of 95% of treated cases was achieved by the surgical opening of the pulley, and in the series of Migaud, et al. [15], the plastic enlargement was successful in 93% of cases. But in the series of Bonnici and Spencer [12], a rate of 100% is observed when the resection of the pulley is done. Unlike other series, the technique of partial resection of the pulley A1 gives excellent results since the success rate is also 100% in our patients' cases (Table 3).
| Authors | Cases | Technique | Hit rate (%) | ||||||||
| Chin-jung lin [19] | 126 | Percutaneous (needle therapy) | 84.9 | ||||||||
| Ha ki [5] | 185 | Percutaneous (tenotomy) | 93.5 | ||||||||
| Wen-chih liu [20] | 203 | Percutaneous alone | 99.1 | ||||||||
| Wen-chih liu [20] | 229 | Percutaneous + Injections | 97.5 | ||||||||
| Hodgkinson [10] | 101 | Opening of the pulley | 95 |
| Migaud [15] | 15 | Plastic enlargement | 93 |
|---|---|---|---|
| Bonnici [12] | 75 | Resection of the pulley | 100 |
| Our serie | 20 | Resection of the pulley | 100 |
This explains that despite the success rate of corticosteroid injection, the percutaneous technique and plastic enlargement in some patients' cases, surgical resection of the pulley remains the best treatment for a lower risk of recurrence or rupture of the tendon [2]. The surgical release of trigger fingers exposes them to a number of complications, although rare, such as: infection, nerve damage, «bowstringing effect" of flexor tendons, recurrence, scar pain, stiff fingers [2, 4]. We notice that the most important complication rate in the literature was published by Thorpe [13] (7%). However, more recent studies have reported a higher success rate [3] and a very low morbidity rate (1%). In our series, we did not observe any major complications, which is not the case for the other experiments. Conclusion The trigger finger is a relatively common, benign, easily treated pathology, which symptoms are unfortunately ignored by a large number of physicians, and that often leads to a delayed diagnosis for the patient and consequently a delay in a proper treatment. Even if we have achieved good results for all our patients, we must take into account the efficiency and the mildness of the injections which do not require any pre- therapeutic assessment and which can be done on an out- of-hospital care (outpatient clinic, ambulatory care). The surgical indication seems acceptable when symptoms persist after a medical treatment by steroid injection.
References
-
Lange-Riess D, Schuh R, Hönle W, Schuh A (2009) Long-term results of surgical release of trigger finger and trigger thumb in adults. Arch Orthop Trauma Surg 129(12): 1617-1619.
-
Durand S, Daunois O, Gaujoux G, Méo S, Sassoon D, et al. (2011) Trigger digits. Chir Main 30(1): 1-10.
-
Moore JS (2000) Flexor tendon entrapment of the digits (trigger finger and trigger thumb). J Occup Environ Med 42(5): 526-545.
-
Ryzewicz M, Wolf JM (2006) Trigger digits: principles, management, and complications. J Hand Surg Am 31(1): 135-146.
-
Sampson SP, Badalamente MA, Hurst LC, Seidman J (1991) Pathobiology of the human A1 pulley in trigger finger. J Hand Surg Am 16(4): 714-721.
-
Sbernardori MC, Bandiera P (2007) Histopathology of the A1 pulley in adult trigger fingers. J Hand Surg Eur 32(5): 556-559.
-
Sbernardori MC, Mazzarello V, Tranquilli-Leali P (2007) Scanning electron microscopic findings of the gliding surface of the A1 pulley in trigger fingers and thumbs. J Hand Surg Eur 32(4): 384-387.
-
Diab RA (2015) Percutaneous release of trigger finger. J Orthop Surg (Hong Kong). 23(2): 241-242.
-
Stefanich RJ, Peimer CA (1989) Longitudinal incision for trigger finger release. J Hand Surg Am 14(2 Pt 1): 316-317.
-
Hodgkinson JP, Unwin A, Noble J, Binns MS (1988) Retrospective study of 120 trigger digits treated surgically. J R Coll Surg Edinb 33(2): 88-90.
-
Lyu SR (1992) Closed division of the flexor tendon sheath for trigger finger. J Bone Joint Surg Br 74(3): 418-420.
-
Bonnici AV, Spencer JD (1988) A survey of 'trigger finger' in adults. J Hand Surg Br 13(2): 202-203.
-
Thope AP (1988) Results of surgery for trigger finger. J. Hand Surg 13(2): 199-201.
-
Kapandji IA (1983) Plastie d’agrandissement des poulies métacarpiennes. Ann Chir Main 2(3): 281- 282.
-
Migaud H, Fontaine C, Brazier J, Pierchon F, Duquennoy A, Kapandji (1996) Enlargement plasty of A1 pulley. Results in 15 primary trigger fingers with a 5 year (2-8 years) follow-up. Ann Chir Main Memb Super 15(1): 37-41.
-
Pegoli L, Cavalli E, Cortese P, Parolo C, Pajardi G (2008) A comparison of endoscopic and open trigger finger release. Hand Surg 13(3): 147-151.
-
Lin CJ, Huang HK, Wang ST, Huang YC, Liu CL, et al. (2016) Open versus percutaneous release for trigger digits: Reversal between short-term and long- termoutcomes. J Chin Med Assoc 79(6): 340-344.
-
Werthel JD, Cortez M, Elhassan BT (2016) Modified percutaneous trigger finger release. Hand Surg Rehabil 35(3): 179-182.
-
Ha KI, Park MJ, Ha CW (2001) Percutaneous release of trigger digits. J Bone Joint Surg Br 83(1): 75-77.
-
Liu WC, Lu CK, Lin YC, Huang PJ, Lin GT, et al. (2016) Outcomes of percutaneous trigger finger release with concurrent steroid injection. Kaohsiung J Med Sci Dec 32(12): 624-629.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results