Clinical Efficacy of Platelet-Rich Plasma on Allograft Transplantation after Core Decompression for Osteonecrosis of the Femoral Head
Purpose: This study explored the outcomes and clinical use of autologous, platelet-rich plasma (PRP) infusion after allograft bone transplantation for osteonecrosis of the femoral head (ONFH) by comparing the time to bone fusion and clinical symptoms. Method and Materials: From January 2008 to June 2015, 36 patients with a follow-up of at least 12 months were enrolled. 18 who underwent autologous PRP infusion after allograft bone transplantation were compared with 18 who underwent allograft bone transplantation only. Changes in pain and activities of daily living were assessed by a visual analog scale (VAS), the Harris Hip Score (HHS) and the time to bone fusion respectively, to evaluate differences between the two groups. Results: The VAS scores of patients who underwent autologous, PRP infusion was significantly improved compared to patients who did not undergo autologous, PRP infusion at post-operative 3 months(From 7.44 to 3.28 in PRP/ From 7.06 to 5.67 without PRP), but not at post-operative 12 months(From 7.44 to 6.95 / From 7.06 to 7.00). The HHS which showed no significant difference between groups(75 / 76). The mean time to bone fusion was 3.0 months (range, 1.5 to 5.7 months) in PRP group and 5.5 months (4.0 to 8.0 months) in without PRP group. Conclusion: Autologous, PRP infusion after allograft bone transplantation of core decompression for ONFH can promote bone fusion and initially produces effective pain control. However, the natural progression of disease, including femoral epiphyseal depression or osteonecrosis of the femoral head, is unlikely to be affected.
Introduction
Complete treatment of osteonecrosis of the femoral head remains an unsolved issue in orthopedic surgery. Many treatments that involve articular preservation have been introduced; however, the best treatment has not yet been established. Most patients who undergo non- operative treatments eventually require hip joint transposition owing to post-operative progression to early femoral head depression and articular dissonance [1]. Core decompression, an articular salvage operation, is used most frequently due to its simplicity and superior outcomes [2]. Core decompression treats the initial non- traumatic femoral head osteonecrosis, and many authors have hypothesized that restoration of femoral head circulation induced by facilitated venous flow in the bone marrow and decreased internal pressure of the femoral head leads to osteogenesis [3]. Recently, the post core decompressive track has been used for bone transplantation due to the expected effects of bone transplantation on adaptation to weight loading [4]. Through a review of previous papers [1] that reported no difference in success rate between decalcified bone matrix transplantation and autologous bone graft performed simultaneously with core decompression, we concluded that the issue of donor area could be resolved. Further, administration of platelet-rich plasma enables the heavy discharge of highly concentrated platelet- derived growth factor (PDGF), transforming growth factor-β (TGF-β), and insulin-like growth factor-1 (IGF- 1),[5] suggesting that platelet-rich plasma infusion could promote simultaneous bone cell differentiation and proliferation with unlimited allogeneic bone transplantation and could greatly improve the post- operative outcomes of bone transplantation through core decompression. Hence, in this retrospective study, we compared the outcomes of post-operative allogeneic bone transplantation performed with and without the administration of platelet-rich plasma after core decompression to treat femoral head osteonecrosis. We evaluated the following outcomes: rate of successful operation by Ficat-Arlet and ARCO staging, percentage of necrotic area on the MRI image, pain alleviation on a visual analogue scale (VAS), and mobility by the Harris Hip Score.
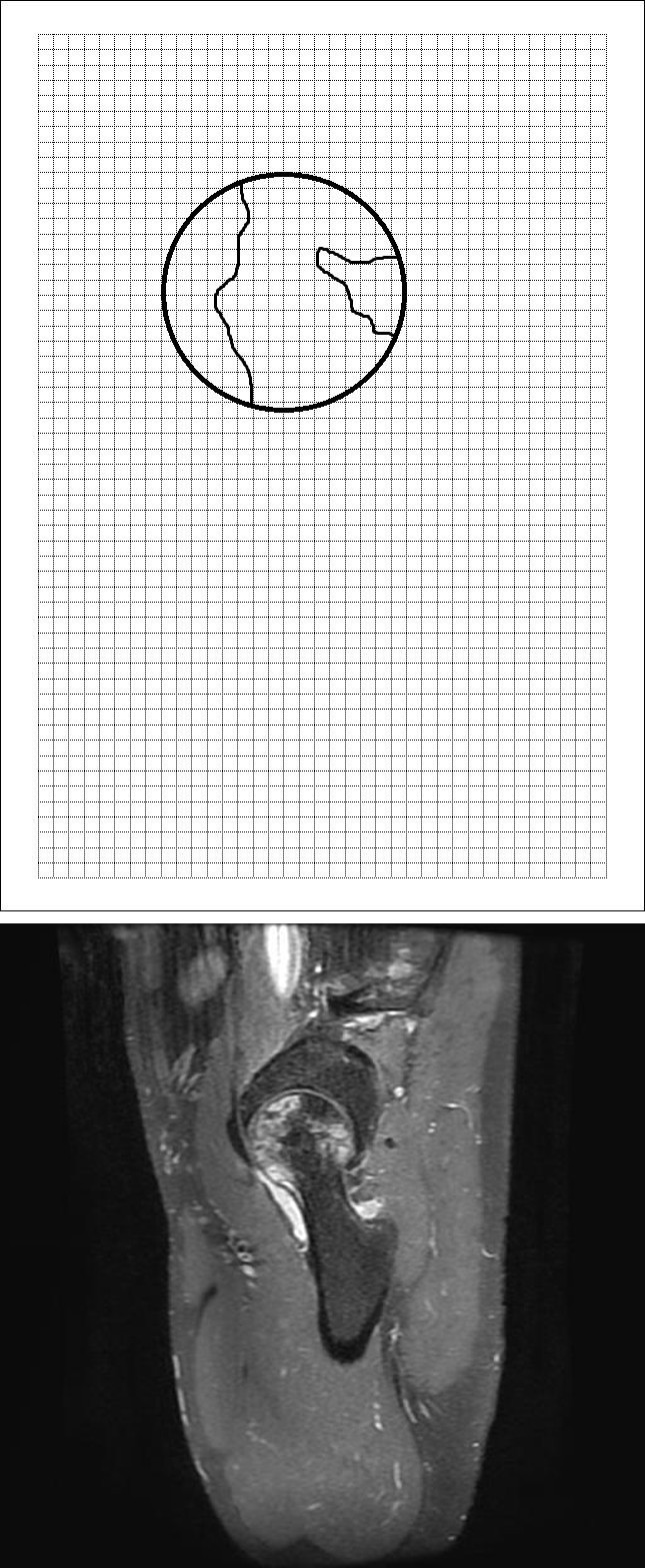
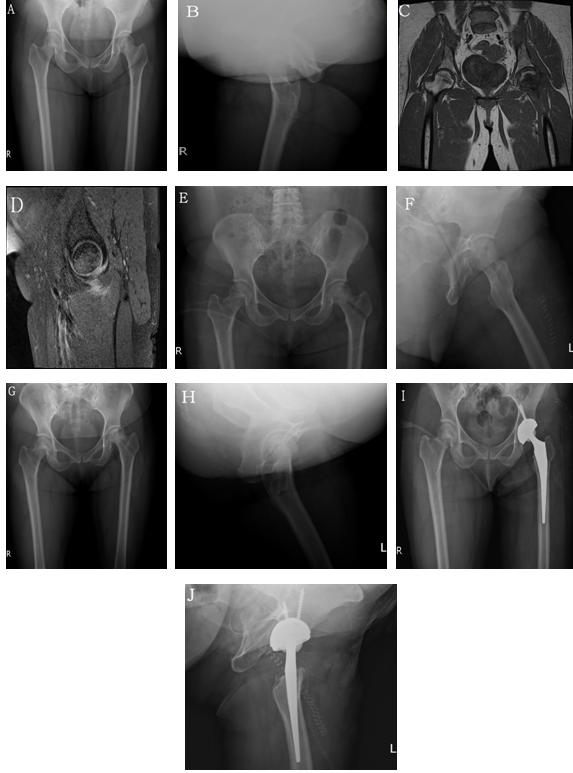
Simple radiographs and MRI images were used to determine the pre-operative radiographic Ficat-Arlet and ARCO stages. The percentage of necrotic area to the entire area of the femoral head on the midsagittal section of the MRI image was measured with graph paper (Figure 1,2,3); these measurements were categorized as follows: group A, up to 25% necrotic area; group B, 26% to 50% necrotic area; group C, 51% to 75% necrotic area; and group D, over 75% necrotic area. The MRI images (T1-weighted spin-echo image [TR = 686.0 msec, TE = 10.3 msec] and T2-weighted spin-echo images [TR = 4577.0 msec, TE = 75.3 msec]) of the coronal and sagittal views of the hip joint around the center of the femoral head were obtained with 2 mm of thickness and spacing using the DISCOVERY MR750w (GE Healthcare, America).
Patients and Methods
Selection of Study Subjects
This retrospective comparison study included patients who underwent post-operative allogeneic bone transplantation for the core decompressive track after core decompression for femoral head osteonecrosis below Ficat-Arlet stage IIB and ARCO stage III diagnosed in our hospital between January 2008 and June 2015. All patients signed an informed consent form, and the institutional review board of our institution (Kosin University Gospel Hospital, Busan, South Korea) approved this retrospective study. The subjects selected for the study were followed up for at least 12 months and were comprised of 36 patients who completed the post- operative core decompressive track without autologous bone graft, composed of 18 patients (20 cases) who underwent infusion of platelet-rich plasma and 18 patients (20 cases) who did not undergo platelet-rich plasma infusion. There were 27 male patients (30 cases) and 9 female patients (10 cases), and the average age at the time of operation was 36.0 years (range, 21 to 55 years). The mean follow-up period was 19.5 months (range, 12 to 64 months) for all cases combined, 19.6 months (12 to 64 months) for cases of platelet-rich plasma infusion, and 19.4 months (12 to 55 months) for cases without infusion. Four patients had core decompression on both sides. For most cases, osteonecrosis was caused by steroid use (15 cases), followed by drinking (14 cases), unidentified idiopathic causes (9 cases), and caisson disease (2 cases).
Characteristics of the Study

Failure of operation was defined as radiographic evidence of disease progression that advanced more than one stage compared to the pre-operative state or a transition to total hip arthroplasty due to clinically or radiographically identified progression within 12 months after the operation. In all patients, the success of core decompression was based on the pre-operative and final radiographic findings and clinical symptoms. In addition, based on radiographic images captured during the follow- up period, the length of time without any evidence of femoral head depression or progression of clinical symptoms while the boundary between the allogeneic and host bones disappeared or the shape of the bone trabeculae changed with the restoration of the marrow cavity and formation of newly generated bone by the absorption of the grafted allogeneic bone was considered to be the beginning of the fusion of the grafted allogeneic bone. The time to fusion of the grafted bones was then compared between groups. The preoperative VAS scores and those at postoperative 3, 6, and 12 months were compared within and between the two groups to identify the degree of post-operative pain alleviation. The Harris Hip Scores at the 12-month follow-up were compared to assess the mobility of patients.
Surgical Technique
The corresponding author(s) of this paper performed all operations. Patients were placed supine on the operation table. For the anterolateral approach, approximately 7 cm of the skin external to the femoral greater trochanter was incised. The femoral fascia was longitudinally incised, and the vastus lateralis was excoriated in the shape of an ‘L’ from its origin to expose the proximal lateral side of the femur. The inlet and direction of the ‘marker needle’ were set under the image intensifier. With insertion of the marker needle into the necrotic area, core decompression was executed using a trochar that was 8 mm in diameter. Thereafter, the necrotic area was curetted and cleaned, and compressive bone transplantation was carried out with the allogeneic bone used for the core decompression track, a 15-cc bone chip (Korea Bone BankⓇ, Seoul, Korea). The bone chip had previously been collected from the femoral head, chemically treated with peroxide and ethanol, dried, frozen for 24 hours at -70℃, and sterilized by gamma ray (25k Gy). To collect the platelet-rich plasma, 9 cc of venous blood was collected from a vein in either the upper arm or the lower limb of patients under general or spinal cord anesthesia during the operation. To minimize damage to the platelets during blood collection, an 18- gauge needle was used, with 1 cc of anticoagulant citrate dextrose-A (ACD-A) added. Then 2.5-cc of platelet-rich plasma was extracted using Dr. Shin’s PRP System Thrombo Kit (Korea MELSMONⓇ, South Korea) and centrifuged at 3,200 rpm for 8 min. The concentration of platelet in the plasma extracted for this study averaged 15 x100,000 pcs/ul, a clinically significant amount for the intended purpose. The extracted platelet-rich plasma was preserved in a sterilized syringe and then mixed with the allogeneic bone to be grafted during the operation.
Follow-up protocol
Patients left the hospital after the operation with the aid of a pair of crutches, which enabled them to walk under partial load (50%) that was gradually increased to full load after 6 weeks. Patients who underwent bilateral operations continued to use crutches until walking was no longer painful. In addition, patients performed exercises focused on strengthening of the abductor muscle and were instructed to avoid high-impact activities for 1 year.
Statistics
SPSS for Windows version 15.0 was used for statistical analyses. Fisher’s exact test was used to compare the failure rate of the operation types and the difference in time to bone fusion between groups that did or did not receive platelet-rich plasma. Student’s t-test was used to compare the VAS scores and Harris Hip Scores between groups. P-values < 0.05 were considered statistically significant.
Results
The pre-operative radiographic classification according to the Ficat-Arlet stage revealed that the group that received the platelet-rich plasma with the allogeneic bone graft included 4 cases of Stage I, 10 cases of Stage IIA, and 6 cases of Stage IIB. Success rates were 100% (4 cases) for Stage I, 60% (6 cases) for Stage IIA, and 0% (0 cases) for Stage IIB. The group that underwent the operation without platelet-rich plasma included 5 cases of Stage I, 11 cases of Stage IIA, and 4 cases of Stage IIB. Success rates were 80% (4 cases) for Stage I, 36.4% (4 cases) for Stage IIA, and 0% (0 cases) for Stage IIB. For each group, the lower stages were associated with higher rates of success (p=0.01, p=0.02, respectively; Tables 1, 2).
Pre-operative radiographic classification with ARCO staging revealed that the platelet-rich plasma group included 2 cases of Stage I, 12 cases of Stage II, and 6 cases of Stage III, with associated success rates of 100% (2 cases), 66.6% (8 cases), and 0% (0 cases), respectively. The groups that underwent allogeneic bone graft without platelet-rich plasma included 3 cases of Stage I, 13 cases of Stage II, and 4 cases of Stage III, with associated success rates of 100% (3 cases), 38.4% (5 cases), and 0% (0 cases), respectively. Lower stages were associated with higher rates of successful operation for each group (p=0.02, p=0.04, respectively; Tables 3,4).
Table 1: Success Rate in Relation to Ficat and Arlet Stages in the PRP Group
| No. | No. of Successes | Success Rate (%) | P-Value* |
| :--- | :--- | :--- | :--- |
| I | 4 | 4 | 100 |
| IIA | 10 | 6 | 60 |
| IIB | 6 | 0 | 0 | 0.01 |
| Total | 20 | 10 | 50 |
Table 2: Success Rate in Relation to Ficat and Arlet Stages in the Non-PRP Group.
| No. | No. of Successes | Success Rate (%) | P-Value* |
| :--- | :--- | :--- | :--- |
| I | 5 | 4 | 80 |
| IIA | 11 | 4 | 36.4 |
| IIB | 4 | 0 | 0 | 0.02 |
| Total | 20 | 8 | 40 |
Table 3: Success Rate in Relation to ARCO Stage in the PRP Group.
| No. | No. of Successes | Success Rate (%) | P-Value* |
| :--- | :--- | :--- | :--- |
| I | 2 | 2 | 100 |
| II | 12 | 8 | 66.6 |
| III | 6 | 0 | 0 | 0.02 |
| Total | 20 | 10 | 50 |
Table 4: Success Rate in Relation to ARCO Stage in the Non-PRP Group
The pre-operative classification of necrotic area based on findings from MRI included 12 cases of Group A, 23 cases of Group B, 4 cases of Group C, and 1 case of Group D. The average percentage of necrotic area was 34.1% (range, 12.5% to 87.5%). The associated failure rate of each operation was 16.7% (2 cases) in Group A, 78.2% (18 cases) in Group B, 100.0% (4 cases) in Group C, and 100.0% (1 case) in Group D. Six cases in Group B (33.3%), 4 cases in Group C (100.0%), and 1 case in Group D (100.0%) underwent total hip arthroplasty.
The average dosage of platelet-rich plasma administered for allogeneic bone transplantation was 6.0 cc (range, 5.0 to 7.0 cc). The average dosage of allogeneic bone administered to all patients was 26.7 cc (20 to 30 cc; Tables 5,6). All 36 patients (40 cases) achieved fusion of the grafted bone; however, 9 patients (50%) in the group that received platelet-rich plasma and 12 patients (66.6%) in the group that underwent allogeneic bone graft only experienced failure of the operation. Among these patients, 4 (22.2%) who received platelet-rich plasma and 6 (33.3%) who underwent allogeneic bone graft only were changed to total hip arthroplasty.
| No | Age/Sex | Site | F/U | Union | Bone | PRP | *Result | Harris Hip Score | *Preop | *Postop 3month VAS | *Postop 6month VAS | *Postop 12month VAS | ||||
| No | Age/Sex | Site | (months) | (months) | Size | (cc) | (cc) | *Result | Harris Hip Score | |||||||
| 1 | 55/M | Left | 12 | 3 | A | 30 | 6 | Success | 75 | 7 | *Postop 3month VAS | *Postop 6month VAS | *Postop 12month VAS | 3 | 3 | 7 |
| 2 | 54/M | Left | 15 | 3 | C | 25 | 6 | Failure(Arthroplasty) | 71 | 8 | 3 | 2 | 9 | |||
| 3 | 47/M | Right | 12 | 3 | A | 30 | 6 | Success | 76 | 6 | 3 | 3 | 6 | |||
| 4 | 43/F | Left | 17 | 2.5 | A | 25 | 6 | Success | 77 | 6 | 3 | 3 | 6 | |||
| 5 | 42/F | Both | 12 | 3 | B/B | 25 | 6 | Failure(Arthroplasty) | 71 | 7 | 2 | 2 | 7 | |||
| 6 | 32/M | Both | 13 | 1.5 | A/A | 25 | 7 | Success | 79 | 6 | 3 | 3 | 6 | |||
| 7 | 31/M | Right | 12 | 3 | B | 25 | 6 | Failure(Arthroplasty) | 73 | 8 | 4 | 3 | 8 | |||
| 8 | 28/F | Left | 20 | 4 | A | 30 | 6 | Success | 75 | 7 | 3 | 3 | 6 | |||
| 9 | 26/M | Both | 64 | 2.5 | B/B | 30 | 6 | Failure | 72 | 7 | 3 | 3 | 6 | |||
| 10 | 26/M | Right | 42 | 2 | B | 25 | 6 | Failure | 79 | 9 | 4 | 3 | 7 | |||
| 11 | 22/M | Right | 32 | 2 | B | 25 | 5 | Success | 79 | 8 | 3 | 3 | 6 | |||
| 12 | 21/M | Both | 15 | 2.5 | B/B | 25 | 6 | Success | 78 | 8 | 3 | 3 | 7 | |||
| 13 | 55/M | Left | 16 | 3 | B | 25 | 6 | Success | 79 | 7 | 3 | 3 | 6 | |||
| 14 | 45/F | Right | 13 | 2.5 | D | 25 | 5 | Failure(Arthroplasty) | 71 | 8 | 3 | 3 | 8 | |||
| 15 | 33/M | Left | 14 | 3 | B | 25 | 6 | Failure | 75 | 8 | 3 | 3 | 8 | |||
| 16 | 24/M | Right | 15 | 3 | B | 30 | 6 | Failure | 72 | 8 | 4 | 4 | 7 | |||
| 17 | 20/M | Left | 15 | 7.5 | B | 30 | 7 | Success | 78 | 7 | 5 | 5 | 6 | |||
| 18 | 35/M | Left | 15 | 3 | B | 25 | 6 | Failure | 70 | 9 | 4 | 3 | 9 |
Table 1: Success Rate in Relation to Ficat and Arlet Stages in the PRP Group
*Result, Operative success and failure, including arthroplasty; †Preop, Preoperative; ‡Postop, Postoperative. Table 5: Details of the Patients in the PRP Group
| No | Age | Site | F/U | Union | Bone | *Result | Harris Hip Score | †Preop VAS | ‡Postop 3months VAS | ‡Postop 6months VAS | ‡Postop 12months VAS | |
| No | /Sex | Site | (months) | (months) | Size | (cc) | *Result | Harris Hip Score | †Preop VAS | ‡Postop 3months VAS | ‡Postop 6months VAS | ‡Postop 12months VAS |
| 1 | 21/F | Left | 15 | 4.5 | A | 25 | Success | 76 | 7 | 5 | 4 | 7 |
| 2 | 44/M | Left | 12 | 4 | C | 25 | Failure(Arthroplasty) | 77 | 7 | 6 | 4 | 7 |
| 3 | 55/M | Right | 17 | 4.5 | B | 30 | Failure(Arthroplasty) | 78 | 6 | 5 | 4 | 6 |
| 4 | 23/M | Left | 12 | 5 | A | 30 | Success | 76 | 7 | 6 | 3 | 7 |
| 5 | 50/M | Left | 13 | 5.5 | C | 20 | Failure(Arthroplasty) | 75 | 7 | 5 | 4 | 7 |
| 6 | 28/F | Right | 12 | 5.5 | A | 30 | Success | 77 | 6 | 5 | 3 | 6 |
| 7 | 31/M | Right | 20 | 6 | C | 30 | Failure(Arthroplasty) | 76 | 8 | 6 | 4 | 8 |
| 8 | 28/M | Left | 12 | 5.5 | B | 20 | Failure | 75 | 8 | 6 | 4 | 8 |
| 9 | 26/F | Left | 42 | 7.5 | B | 30 | Failure | 76 | 7 | 5 | 4 | 7 |
| 10 | 36/M | Right | 32 | 8 | B | 30 | Failure | 77 | 6 | 6 | 3 | 6 |
| 11 | 54/M | Right | 64 | 6.5 | B | 30 | Failure(Arthroplasty) | 76 | 7 | 4 | 4 | 7 |
Table 2: Success Rate in Relation to Ficat and Arlet Stages in the Non-PRP Group.
| 12 | 52/F | Right | 16 | 6.5 | B | 25 | Failure(Arthroplasty) | 72 | 8 | 7 | 4 | 8 |
| 13 | 43/M | Left | 15 | 5.5 | B | 20 | Failure | 75 | 6 | 4 | 5 | 7 |
| 14 | 23/M | Right | 15 | 6 | A | 30 | Success | 76 | 7 | 6 | 4 | 7 |
| 15 | 50/F | Left | 14 | 5.5 | A | 30 | Success | 77 | 7 | 6 | 4 | 6 |
| 16 | 23/M | Right | 13 | 4.5 | B | 30 | Failure | 76 | 8 | 7 | 5 | 8 |
| 17 | 22/M | Left | 15 | 4.5 | B | 25 | Failure | 75 | 7 | 7 | 4 | 7 |
| 18 | 34/M | Left | 15 | 5 | A | 20 | Success | 78 | 8 | 6 | 3 | 7 |
Table 3: Success Rate in Relation to ARCO Stage in the PRP Group.
- *Result, Operative success and failure, including arthroplasty;
- †Preop, Preoperative; ‡Postop, Postoperative.
- The average time to the initiation of bone fusion after the operation was 3.0 months (1.5 to 7.5 months) in the
- 18 patients (20 cases) who received platelet-rich plasma and 5.5 months (4.0 to 8.0 months) in the 18 patients
- No.: Number *p-values by Student’s t-test
- PRP group No. (%)
- Non-PRP group No. (%)
- P-Value*(Union(month))
- Union Failure
- 0 (0)
- 0 (0)
- Operation Failure
- 9 (50%)
- 12 (66.6%)
- Arthroplasty
- 4 (22.2%)
- 6 (33.3%)
- Union (month)
- 3
- 5.5
- 0.021
Table 4: Comparison of Failure Rates between the PRP and Non-PRP Groups
The VAS scores that were used to assess pain alleviation over time were collected pre-operatively and at post-operative 3, 6, and 12 months. These scores were 7.44, 3.28, 3.06, and 6.95, respectively, for the group that received platelet-rich plasma and 7.06, 5.67, 3.89, and 7.00, respectively, for the group that had allogeneic bone graft only. Both groups showed significant pain alleviation through post-operative 6 months (p-value < 0.05). Pain alleviation at postoperative 3 months was significantly greater in the group that received platelet-rich plasma than in the group that had bone graft only; however, at post-operative 12 months, this difference was no longer apparent. The Harris Hip Scores were used to compare the mobility of patients. Pre-operative measurements were unavailable. However, the post-operative measurements at the 12-month follow-up did not differ significantly between the two groups (platelet-rich infusion group: 75; allogeneic bone graft only group: 76). No complications associated with infusion of the platelet- rich plasma, such as infections, were observed.
Discussion
Osteonecrosis of the femoral head triggers collapse of the femoral head and secondary coxitis resulting from necrosis of bone cells, causing structural change. The disease primarily occurs in patients undergoing artificial hip joint transposition surgery and mainly affects patients aged 30-50 years. The disease is a serious one because a large lesion can cause breakdown of the hip joint when the necrotic area invades the part of the bone responsible for weight bearing [6]. Treatment of femoral head osteonecrosis aims to preserve the femoral head through early diagnosis and to prevent expansion of the area of the lesion to avoid the need for total hip arthroplasty [7]. Many methods for articular salvage have been introduced. One such method, core decompression, is often used to treat initial lesions, and studies have documented diverse clinical results. In the current study, core decompression was performed in 38 patients (40 cases), 21 of whom (22 cases, 52%) demonstrated failure of the operation and 10 of whom (26.3%) underwent total hip arthroplasty. In addition, the rate of successful operations was higher for lower staged lesions and those with a smaller area. These results are consistent with those of Fairbank et al. [8] who reported a higher survival rate for lower staged lesions, and those of Rajagopal et al. [9] who reported that 26% of post-operative cases of core decompression eventually transitioned into total hip arthroplasty. Therefore, core decompression for osteonecrosis of early, pre-collapse disease stages [10] (i.e., lesions in Ficat Stage I [11]) is expected to lead to favorable outcomes through early treatment based on early diagnosis with MRI images [12]. Kim et al.[13] combined calcium phosphate transplantation with compressive bone graft to prevent post-operative collapse of the femoral head attributable to the weakening of subcartilaginous support. They found that the Harris Hip Score had increased at the final follow- up. Wei and Ge et al.[14] reported that a sole vascular, anchorage-independent bone graft resulted in better clinical outcomes in terms of survival rate and Harris Hip Score. In addition, an Indian study compared patients who underwent post-operative allogeneic bone graft with infusion of autologous, platelet-rich plasma after core decompression with patients who underwent bone graft after core decompression [15]. Those patients who received autologous, platelet-rich plasma showed better results as measured by simple radiographs and MRI images, VAS scores, and Harris Hip Scores. However, the authors did not explain the function of the autologous, platelet-rich plasma. Other authors have focused on the benefits of bone graft fusion in simple bone cyst operations [16] and proximal tibial osteotomy [17] induced by infusion of autologous, platelet-rich plasma combined with allogeneic bone transplantation. These authors expected the infusion of autologous, platelet-rich plasma to promote bone graft fusion through the core decompression track. The results of the current study showed an average of 3.0 months to the initiation of bone graft fusion for patients who received autologous platelet- rich plasma, which was shorter than the average of 5.5 months for patients who received bone graft only. Bone fusion can be defined as a change in the shape of bone trabeculae between the host bone and grafted bone or as a radiographic loss of the boundary between them [18]. In this study, the initiation of allogeneic bone fusion was determined by simple radiographic images captured during follow-up. The images showed no evidence of clinical progression or femoral head depression when the marrow cavity was restored. There was evidence of formation of newly generated bone after absorption of the grafted allogeneic bone, with the shape of bone trabeculae changing between the host and bone graft. However, Ranly et al.[19] reported that osteoinductivity, formation of newly generated bone, and the size of ossicles decreased 8 weeks after the infusion of human platelet- rich plasma combined with demineralized bone matrix (DBM) inserted into the gastrocnemius muscles of immunocompromised mice. They suggested that infusion of platelet-rich plasma disrupted bone formation. Further, Arpornmaeklong et al. [20] conducted experiments with mice and suggested that platelet-rich plasma disturbs the bone cell differentiation of pre-osteoblasts. Thus, the effects of platelet-rich plasma infusion on bone fusion require additional follow-up observations. In our study, both groups showed significant improvements in pain through post-operative 6 months; however, pain alleviation was greater in the group that received autologous, platelet-rich plasma at postoperative 3 months. Nonetheless, VAS scores and Harris Hip Scores did not differ significantly between the two groups at post-operative 12 months, suggesting that the administration of autologous, platelet-rich plasma did not stop the natural progression of femoral head necrosis. In this study, 38 patients (40 cases) with femoral head necrosis were examined to identify the effects of platelet- rich plasma infusion combined with allogeneic bone transplantation after core decompression. However, further comparative studies that enroll a larger number of patients and include control and experimental groups are needed. Studies should also consider the effects of platelet-rich plasma on osteonecrosis by considering its functions in the joint cavity, which should be identifiable percutaneously or through arthroscopy for the treatment of femoral head necrosis.
Conclusion
Through the post-operative core decompressive track generated after core decompression to treat initial femoral head osteonecrosis, allogeneic bone graft can be administered with autologous, platelet-rich plasma to promote bone fusion and to maximize the effects of the treatment. In the current study, administration of autologous platelet-rich plasma also led to initial post- operative pain alleviation. However, suspension of the natural progression of femoral head necrosis, including the transition into femoral head depression, through the administration of platelet-rich plasma appears unlikely. Thus, further studies on the effects of platelet-rich plasma infusion for the treatment of femoral head osteonecrosis are required.
References
-
Shim KB, Kwon DS, Oh SJ, Kang JS, Moon KH (2009) The efficacy of core decompression for treating avascular necrosis of the femoral head. J Korean Hip Soc 21(3): 219-225.
-
Mont MA, Carbone JJ, Fairbank AC (1996) Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop 324: 169-178.
-
Yoo MC, Cho YJ, Kim KI, Park BJ, Hwang DW, et al. (1999) Core decompression in nontraumatic osteonecrosis of the femoral head – A comparison study of results between radiographic classification and magnetic resonance imaging. J Korean Hip Soc 11(3): 141-152.
-
Rijnen WH, GardeniersJ W, Buma P, Yamano K, SlooffTJ, et al. (2003) Treatment of femoral head osteonecrosis using bone impaction grafting. Clin Orthop 417: 74-83.
-
el-Ghannam A, Ducheyne P, Shapiro IM (1995) Bioactive material template for in vitro synthesis of bone. J Biomed Mater Res 29(3): 359-370.
-
Kang JS, Park S, Song ru, Jung YY, Cho MR, et al. (2009) Prevalence of osteonecrosis of the femoral head: a nationwide epidemiologic analysis in Korea. J Arthroplasty 24(8): 1178-1183.
-
Markel DC, Miskovsky C, Sculco TP, Pellicci PM, Salvati EA (1996) Core decompression for osteonecrosis of the femoral head. Clin Orthop 323: 226-233.
-
Fairbank AC, Bhatia D, Jinnah RH, Hungerford DS (1995) Long-term results of core decompression for ischemic necrosis of the femoral head. J Bone Joint Surg 77(1): 42-49.
-
Rajagopal M, Balch Samora J, Ellis TJ (2012) Efficacy of core decompression as treatment for osteonecrosis of the hip: a systematic review. Hip Int J Clin Exp Res Hip pathol Ther 22(5): 489.
-
Yoon TR, Song EK, Rowe SM, Park CH (2001) Failure after core decompression in osteonecrosis of the femoral head. Int Orthop 24(6): 316-318.
-
Iorio R, Healy WL, Abramowitz AJ, Pfeifer BA (1998) Clinical outcome and survivorship analysis of core decompression for early osteonecrosis of the femoral head. J Arthroplasty 13(1): 34-41.
-
Genez BM, Wilson MR, Houk RW, Weiland FL, Unger HR Jr, et al. (1988) Early osteonecrosis of femoral head: Detection in high risk patient with MR imaging. Radiology 168: 521-524.
-
JH Park, HS Kim, ST Chung, JH Yoo, JH Kim, et al. (2010) Osteonecrosis of femoral head treated with core decompression & impacted bone graft - a comparative study with and without calcium phosphate. J Kor Musculoskelet Transplant Soc 10(2): 97-102.
-
Wei BF, Ge XH (2011) Treatment of osteonecrosis of the femoral head with core decompression and bone grafting. Hip Int J Clin Exp Res Hip Pathol Ther 21(2): 206.
-
Zulfikar M patel, Kalpesh A Mehta, Shavial S Dalal, Kaushal R Patel. (2015) Comparison of core decompression with autologous PRP infusion v/s core decompression alone in treatment of AVN hip. J of Indian Orthop Rheumatology Association. July- December;1(1): 32-34.
-
Pedzisz P, Zgoda M, Kocon H, Benke G, Gorecki A (2010) Treatment of solitary bone cysts with allogenic bone graft and platelet-rich plasma. A preliminary report. Acta orthop Belgica 76: 374-379.
-
Dallari D, Savarino L, Stagni C , Cenni E, Cenacchi A, et al. (2007) Enhanced tibial osteotomy healing with use of bone grafts supplemented with platelet gel or platelet gel and bone marrow stromal cells. J Bone Surg 89(11): 2413-2420.
-
Stevenson S, Horowitz M (1992) The response to bone allografts. J Bone Joint Surg 74(6): 939-950.
-
Ranly DM, Lohmann CH, Andreacchio D, Boyan BD, Schwartz Z (2007) Platelet-rich plasma inhibits demineralized bone matrix-induced bone formation in nude mice. J Bone Joint Surg Am 89(1): 139-147.
-
Arpornmaeklong P, Kochel M, Depprich R, Kubler NR, Wurzler KK (2004) Influence of platelet-rich plasma (PRP) on osteogenic differentiation of rat bone marrow stromal cells. An in vitro study. Int J Oral Maxillofac Surg 33(1): 60-70.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results