Total Hip Arthroplasty in Patient with Sickled Cell Trait Ss: The Cases of 14 Patients
Osteo-articular complications of sickle cell disease are multiple but mostly dominated by epiphyseal aseptic necrosis. Conservative at the beginning, the surgical treatment becomes radical in the last stage with the performance of a total hip arthroplasty (THA). We report the case of total hip arthroplastyin a patient with sickle cell traitSSat Ordre de Malte Hospital (CHOM) in Dakar, focusing on the peri-operative complications encountered in this particular case in order to prevent them or to treat them if necessary. This is a retrospective, mono-centric study including 15 total hip arthroplasty (THA) performed in 14 SS sickle cell patients over a 66-month period. The postero-lateral Moore mini open approach was used exclusively. The clinical evaluation was based on the Aubigné Postel-Merle (PMA) and Harris (HHS) scores and the radiographic score on the Ficat and Arlet classification. The corticodiaphyseal index as well as the Noble flare index channel made it possible to appreciate the medullary congestion and the shape of the femur. All together, THA in Sickle Cell Disease represented 7.57% of all hip prosthetic activity during the period. The average age of patients (10 women and 4 men) was 29.06 years (18-50). The overall functional result was good and very good in 77% of cases. We observed 4 femoral fissures, an early vesicular lithiasis infection with psoas syndrome and acetabular loosening in the same patient and one death at 5 days postoperatively.
Introduction
Sickle cell disease is the most common hemoglobinopathies throughout the world [1, 2, 3]. Aseptic necrosis of the femoral head is considered to be the cell death of the various components of the bone (bone tissue, bone marrow) if there is no infectious cause. It represents the most common orthopedic complication of sickle cell disease [4, 5]. The surgical treatment is conservative or non-prosthetic at stages I, II or III of Ficat and Arlet; otherwise it becomes radical in the last stage with the performance of a THA [6, 7]. The variegated bone of sickle cell disease is liable to infections, to per and postoperative mechanical complications and to those related to anesthesia [6]. The performance of such surgery in very young patients is risky therefore; African surgeons should take it into account. The purpose of this work is to report our experience of THA in an adult sickle cell by focusing on the perioperative complications met on this particular ground, in order to propose recommendations.
Material and Methods
This is a retrospective study, single-centric bi operators (2 senior operators) with consecutive recruitment conducted between January 2011 and June 2016 at CHOM / Dakar. Included was all patients with sickle cell trait SS operated on for an THA during the period. Seven patients were excluded, including 6 with sickle cell trait AS and one with Sickle Cell Disease with post traumatic necrosis (transcervical fracture treated with DHS plate screw and presenting a secondary necrosis 5 years later). The series thus includes 14 adults with sickle cell disease including one case of bilateral THA. The patients’ average age was 29.06 years (18-50). The average body mass index (BMI) was 19.14 kg/m² (15.06-29.39). The left hip was affected in 6 cases, the right one in 2 cases and the involvement was bilateral, more severe on the left hip in 6 patients. The average surgical time was 17 months (21 days - 43.5 months). The Moore mini open posterolateral approach was used in all patients. Uncemented THA was used exclusively. The average hemoglobin level of our patients went from 8.59 g / 100 ml before the procedure to 8.03g / 100ml on day 2 postoperatively. Five patients were transfused with an average of 1.3 red blood cells. According to the classification of Ficat and Arlet, 9 hips were at stage IV and 6 at stage III. Both the image intensifier and small diameter rigid reamers were used. Preoperative and anesthetic planning was performed in all patients. Perioperative complications were noted. The postoperative care protocol was clinical (pain management, antibiotherapy, anticoagulant), biological (blood count postoperative control, Day 1 and Day2) and radiological (control X-ray on D1, D21, Month 2, Month 3, Month 6, year 1 then every year). Patients were assessed with a mean follow-up of 2.5 years (10-66 months). For the clinical evaluation we used PMA and HHS ratings.
Results
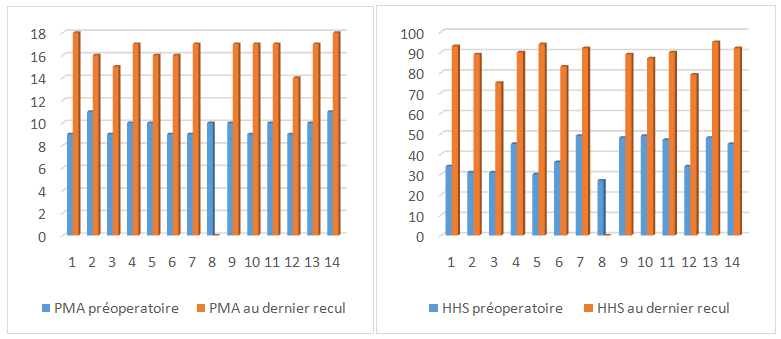
92% of the patients were satisfied with the results of the surgery against 8% of dissatisfaction. According to the PMA rating, we obtained 77% good and very good results and 15% excellent results. The medullar canal of our patients was overall reduced by necrosis with an average corticodiaphyseal index of 1.39 (0.5-5.6) (N = 0.48 ± 0.09). According to Noble's classification [8], 10 patients had a standard shape femur and 3 had a champagne flute-like femur. The mean PMA and HHS scores increased respectively from 9.64 (9-11) to 16.35 (15 -18) before the surgery and from 39.78 (30- 49) to 87.35 (75 - 95) at the last follow-up. These results are shown in Table 1 and Figure 1.
| Studied factors | Results |
|---|---|
| Average Age | 29,06 |
| Average IMC | 19,14 |
| Average intervention time (years) | 2,5 |
| Preoperative PMA | 9,64 |
| Postoperative PMA | 16,35 |
| Preoperative HHS | 39,78 |
| Postoperative HHS | 87,35 |
| Corticodiaphyseal Index | 1,39 |
Table 1: Representation of the different results.
Six (6) complications were found
- 4 femoral fissures according to the Barlas classification [9] (2 sitting on the calcar and 2 with an extension towards the subtrochanteric region) stabilized by strapping with deferred support. The other 2 cracks did not require any additional gesture.
- 1 death at day 5 postoperative in a disseminated intravascular coagulation table in a patient who had already received aTHA.
- Early infection on a gallbladder stone with psoas syndrome and signs of acetabular detachment in the same patient The infection was cured by surgical lavage and dual antibiotic therapy: Imipenem 500 mg twice daily in mini
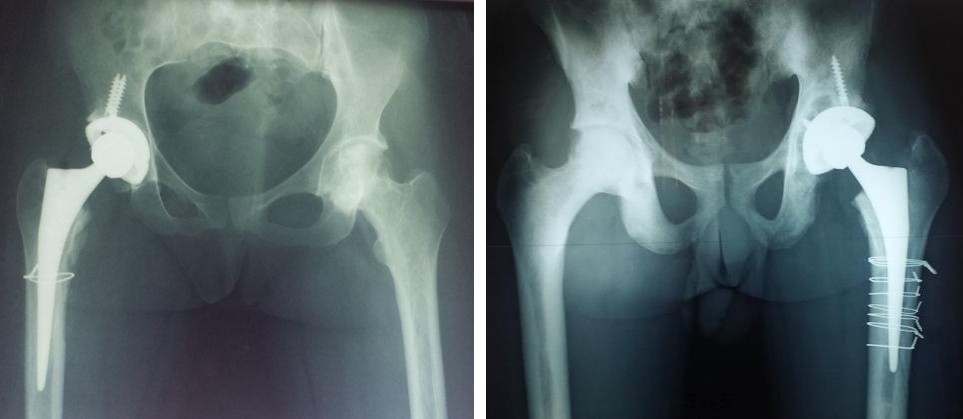
infusion and phenicole (500 mg three times daily) for 30 days. Laparoscopic cholecystectomy was performed on post-THA. These complications are summarized in Table 2 and Figure 2.
| Complications | Type | Number | |
|---|---|---|---|
| Early infection on a gallbladder stone with psoas syndrome and signs of acetabular detachment in the same patient | Peroperative | femoral Fissures | 4 |
| Early infection on a gallbladder stone with psoas syndrome and signs of acetabular detachment in the same patient | Postoperative | Early Infection Psoas Syndrome Unipolar loosening | 1 |
| Early infection on a gallbladder stone with psoas syndrome and signs of acetabular detachment in the same patient | Postoperative | 5-day postoperativedeaths | 1 |
Table 2: Observed complications.
Discussion
The purpose of this work was to report the experience of THA in Sickle Cell Disease by focusing mainly on complications. THA was bilateral in one of our patients while 26% of SENE’s patients were operated on both hip sides. The involvement of both hips is common in case of sickle cell disease [10, 11]. The young age of our patients, 29.06 years on average (18-50) corresponds to most series of the literature. Homawoo found that in Togo, necrosis occurred in very young patients between the ages of 15 and 30 [12]. The 244 sickle cell patients in whom Hernigoua performed 312 THA had a mean age of 32 years [6]. All our patients were at stages III and IV at the time of the intervention. Although for some authors, surgical treatment of stage III must still be conservative [7], all agree that arthroplasty remains the only surgical treatment to be implemented in stage IV, where the collapse of the femoral head and the clinical repercussion become too much important [13, 14, 15, 16]. The average corticodiaphyseal index of our patients was high: 1.39 (0.5 - 5.6) (N = 0.48 ± 0.09). The phenomenon of "bone within bone" in sickle cell disease is responsible for the obstruction of the diaphyseal shaft. The medullary canal is significantly reduced by endosteal bone production and apposition, which radiologically results in an increase of the corticodiaphyseal index [17, 18]. The majority of our patients were underweight (6 patients) or had a normal weight range (7 patients) according to WHO criteria. In fact, sickle cell patients often have a low BMI and a low fat mass because of the hypercatabolism associated with the disease [19]. The determination of the flare index channel makes it possible to define the shape of the baffle and foretells the difficulties that can be encountered intra-operatively.
These incidents are increased in funnel-shaped femurs or in champagne flutes [20, 21]. Four of our patients who had intra-operative cracks are in this register. Sickle cell hip surgery is a real challenge for the surgeon [22, 23]. Per and postoperative complications in sickle cell surgery are common in all series [11, 23]. In prosthetic surgery, these complications arise as much from the anatomical changes generated by hip osteoarthritis and surgery as from the field. SENE [11] found 4 perforations of the back of the acetabulum and 8% of fractures and loosening. Rouvillain studied the complications of THA in sickle cell necrosis on 36 THA implanted in 30 homozygous sickle cell patients. He found in addition to medical complications (acute pulmonary syndrome, hemolytic crises with 4 patients sent in intensive care), 2 intra-operative fractures of the femur, a peri-prosthetic fracture, 8 loosening including 4 septic, a superficial infection, 5 patients reported, one death in post operative and another 5 months postoperatively [23].





For the latter, modifications of the femoral shaft must be evaluated preoperatively and careful planning is necessary with the availability of small femoral stems. Several authors agree that medullary crowding by post- necrotic endosteal bone apposition makes medullary access difficult and increases the risk of miscarriage and intraoperative fractures, and SY [16] points out that these difficulties make it necessary to resort to the cautious bore under image intensification using rigid reamers of diameter 8 or 6 and to have a wide range of implants. Anemia is chronic in sickle cell patients because of constant haemolysis. Transfusions are related to blood loss during prosthetic surgery in relation to chronic medullary hyperplasia secondary to anemia and difficulties in preparation of the acetabulum and femoral shaft [24, 25].
Conclusion
Sickle cell osteonecrosis remains unquestionably serious because it deteriorates patients' life quality. In the last stage, THA remains the best surgical treatment most likely to bring relief and comfort to patients. A rigorous planning and multidisciplinary care is required when dealing with young patients. It can involve many complications related to either surgical or related to the sickle cell disease and patients should be informed about it. The operation difficulties on this particular field require a cautious boring of the femoral shaft under image intensifier. It is also necessary to have rigid reamers small diameter cannulated or not and a wide range of implants.
References
-
Pierre A, Bernard AG (2016) Hémoglobinoses : actualités 2016, Médecine Trop. Diplôme Médecine Trop. Pays L’Océan Indien.
-
Andrianne Y, Lamoureux J, Quinin J, Clemens M (1983) La hanche drépanocytaire et son traitement chirurgical, Rev Chir Orthopédique 61-68.
-
Arlet J, Ficat R (1990) Diagnostic et traitement d’une coxopathie chronique, Encycl Méd Chir Appar Locomoteur 5-25.
-
Catonné Y, Mukasa MM, Rouvillain JL, Ribeyre D, others, (2004) Manifestations ostéo-articulaires de la drépanocytose. Maîtrise Orthopédique 135.
-
Hernigou P, Daltro G, Sobrinho UB, Sberge F (2010) Manifestations ostéoarticulaires de la drépanocytose, Gaz. Médica Bahia 80(3): 74-79.
-
Hernigou P, Poignard A, Manicom O, Mukisi Mukasa M, PTH dans la nécrose drépanocytaire, Rev Chir Orthopédique Réparatrice Appar Mot S231-S327.
-
Ndoye G (2012) Traitement non prothétique de l’ostéonécrose de la tête fémorale chez le drépanocytaire (à propos de 12 cas - revue de la litterature). UCAD.
-
Noble PC, Alexander JW, Lindahl LJ, Yew DT, Granberry WM (1988) The anatomical basis of femoral component design (235): 148-65.
-
Barlas KJ, Ajmi QS, Bagga TK, Howell FR, Roberts JA, et al. (2008) Association of intra-operative metaphyseal fractures with prosthesis size during hemiarthroplasty of the hip. J Orthop Surg 16(1): 30- 34.
-
Ilyas I, Moreau P, (2002) Simultaneous bilateral total hip arthroplasty in sickle cell disease. J Arthroplasty 17(4): 441-445.
-
Sène M, Ndiaye A, Mbaye E, Niang CD, Faye M (2009) Arthroplastie totale de hanche dans l’ostéonécrose aseptique du drépanocytaire au Sénégal : série de 48 prothèses. Médecine Trop. 69 573-576.
-
Homawoo K, Bissang K, Songne B, Ayite A (1991) Drepanocytose et osteo-necrose de la tete femorale. medecine afr Noire 38(7): 511-517
-
Acurio MT, Friedman RJ (1992) Hip arthroplasty in patients with sickle-cell haemoglobinopathy. J Bone Jt Surg 74: 367-371.
-
Clarke HJ, Jinnah RH, Brooker AF, Michaelson JD (1989) Total replacement of the hip for avascular necrosis in sickle cell disease, J Bone Joint Surg Br 71(3): 465-470.
-
Mont MA, Marulanda GA, Jones LC, Saleh KJ, Gordon N, et al. (2006) Systematic analysis of classification systems for osteonecrosis of the femoral head, J Bone Jt Surg 88(3): 16-26.
-
Sy MH, Toure-Fall A, Diop-Sall N, Dangou JM, Laye SI (2000) Drépanocytose associée à une fluorose osseuse. Rev Rhum 67: 548-551.
-
Bernard J, Laval-Jeantet M (1962) Le rapport cortico diaphysaire tibial pendant la croissance. Arch Francaise Pédiatrie 19: 805-817.
-
Serra T (2011) Repères et mesures utiles en imagerie ostéo-articulaire. Elsevier Masson, Issy-les- Moulineaux,
-
OMS (2011) Organisation Mondiale de la Santé, Drépanocytose : une stratégie pour la région africaine de l’OMS.
-
Umer M, Sepah YJ, Khan A, Wazir A, Ahmed M, et al. (2010) Morphology of the proximal femur in a Pakistani population, J Orthop Surg 18(3): 279-281.
-
Noble PC, Alexander JW, Lindahl LJ, Yew DT, William GM, et al. (1988) The Anatomic Basis of Femoral Component Design. Clin Orthop 235: 148-165.
-
La PTH dans l’ONA TF post-drépanocytaire.pdf.
-
Rouvillain JL, Ouldamar AK, Ribeyre D (2016) Complications des PTH dans la nécrose de hanche drépanocytaire. Journ Orthopédie OM.
-
Habibi A, Godeau B, Galacteros F (2007) Drépanocytose et réanimation. Réanimation 16: 310- 317.
-
Habibi A, Arlet JB, Stankovic K, Gellen-Dautremer J, Ribeil JA, et al. (2015) Recommandations françaises de prise en charge de la drépanocytose de l’adulte : actualisation. Recomm Fr Prise En Charge Drépanocytose Adulte Actual 36: 5S3-5S84.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results