A Case of Pott’s Disease under the Occipital Area
Pott's disease of the cervico-occipital hinge is an exceptional and serious condition due to the risk of bulbo-medullary compression. The authors present a case of sub-occipital tuberculosis in a 19-year-old patient with progressive and sequential tetraplegia. The MRI which guided our diagnosis showed lytic images at the top of the tooth with an abscess overhanging it and compressing the bulb. The positive diagnosis was confirmed by tuberculin intradermoreaction and Genexpert. As an emergency, we have administered a bolus of corticosteroid and then anti-tuberculous chemotherapy for 9 months. Subsequently we made a posterior lacing C1-C2. The evolution was favorable with the disappearance of the neurological disorders. This type of lesion requires an accurate diagnosis for appropriate care.
Introduction
Under occipital tuberculosis is a rare and serious condition. The diagnosis remains difficult at the beginning of the pathology. In so doing using modern imaging to guide the diagnosis and to establish appropriate therapy is important. Its prognosis is conditioned by the bulbo- medullary involvement. Surgical treatment depends on the extent of the bone and medullary lesions.
Observation
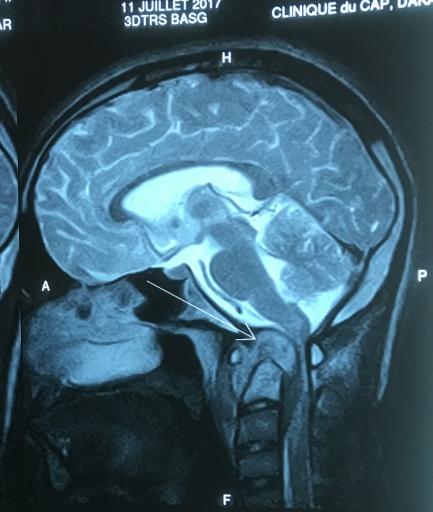
Our case concerned a19 year-old Pupil, with a progressive paralysis of the two upper limbs which started a month ago, due to a falling from a tree which had happened two months before. The examination noted a cervical contracture with motor deficit of the upper limbs without sensory injury rated ASIA B. The CT scan revealed an atlantoaxial dislocation and geodic images of the C2 tooth (Figure 1). The MRIalso revealed the same CT lesions with a painfulthickness of paravertebral soft tissue with a mass-medullary effusion and signs of myelopathic upper spinal cord injury (Figure 2).
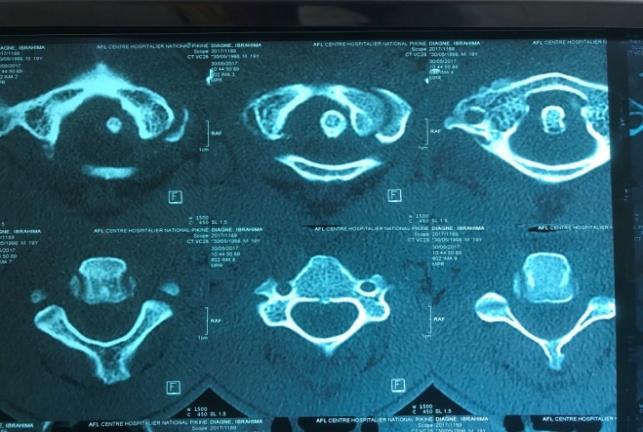
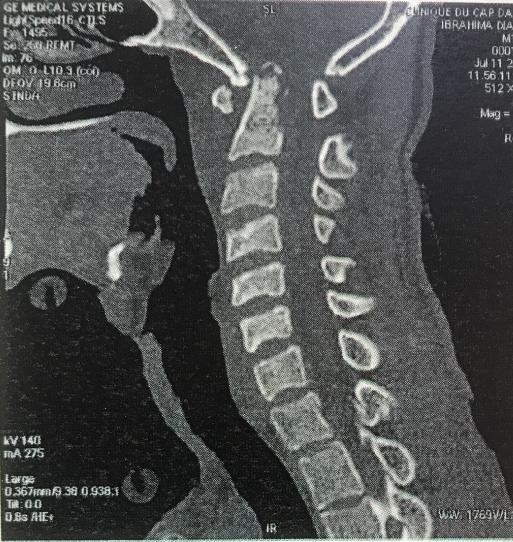
Figure 2: The MRI with a painful thickness of paravertebral soft tissue with a mass- medullary effusion and signs of myelopathic upper spinal cord injury. The biological assessment revealed an inflammatory syndrome with accelerated ESR, a positive CRP and a lymphocytosis without counting leukocytosis. HIV serology was negative with an intradermal positive at 18 mm. Gen Expert was positive in cerebrospinal fluid. The biopsy was not performed knowing that it was risky. After a 24-hour hospitalization, the patient presented, a tetraplegia associated with dyspnea and a fever of 38°3
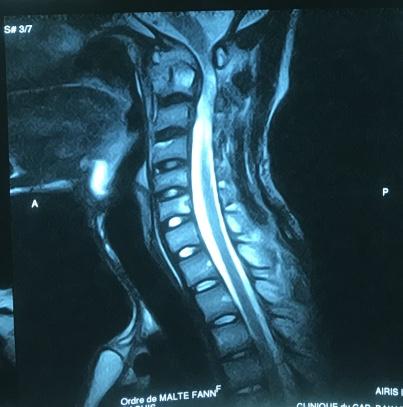
Celsius. We initiated a treatment by administering the patienta corticosteroid bolus containing parenteral Methylprednisolone 120 mg twice daily. This corticosteroid therapy was maintained with degressive doses for one month. After one week the patient totally recovered the use of his four limbs with a muscle strength rated 3 and eupnetic breathing. At the MRI, a regression of the collection and the mass effect could be noted (Figure 3).
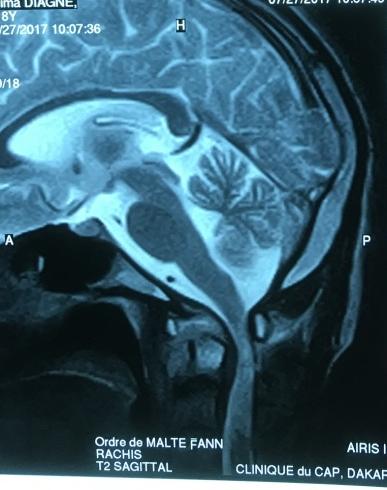

Figure 4: Posterior C1 C2fusion by surgical lacing Two weeks after a quadruple antituberculous chemotherapy (rifampicin, isoniazid, pyrazinamide and etambutol) was then initiated for three months followed by dual therapy for nine months.Because of the importance of the bone and medullary lesions, a C1 C2 lacing was performed (Figure 4) associated with a plaster cast thoracocervical immobilization. After the first phase of antibacillary treatment (2 months) the motor deficit disappeared completely.
Discussion
Despite the frequency of osteoarticular tuberculosis, sub occipital localization remains rare. It represents 1% of spinal locations [1, 2]. It canoccur in different clinical pictures. It may be an array of generally posterior cervical pain, usually asymmetrical with irradiations towards the occipital region, the ear, the upper limb [3]. This lateralization would correspond to a predominant attack of a lateral mass. . Cervical stiffness is typically found in almost 80% of cases [4]. Sometimes it is immediately a more serious picture of medullary compression at the origin of tetraparesis or a tetraplegia of rapid or insidious installation depending on the mechanism involved [4, 5, 6, 7]. The particularity of our observation consistsin the late consultation with flaccid paraplegia of the upper limbs, the localization of the inflammation which overhangs the tooth with compression of the bulb. Laparoscopy of the upper limbs remains exceptional in the sub occipital pott.
In the literature [2, 8], the neurological involvement, if any, is in the form of quadriplegia. This could be explained by a central damage to the spinal cord. According to El Abbassi [8], three physiopathological factors explain the neurological disorders. Disruption C1 C2 by rupture of the transverse ligament, the basilar impression due to the separation of the lysed lateral masses, and abscess extension. We believe that the origin of the neurological disorders is due to the inflammatory process that’s why we observe a regression of the neurological signs without decompression [8, 9, 10]; as it is the case of our patient when we initiated a medical treatment. Due to the difficulties in interpreting conventional X- rays, there is a great delay in diagnosis, which exposes the risk of spinal compression. The radiological criteria to be investigated are the increase in the thickness of the prevertebral soft tissues fromC1 to C3, the anterior sub- luxation of C1 on C2 on the profile picture, and the hyper- transparency with the possibility of settlement of a lateral mass of C1 on frontal incidences [8, 9]. Modern imaging by CT and MRI enablesto analysethe extent of the lesions. It also plays the role of a therapeutic follow-up [8, 9]. The use of CT is paramount in the search for bone sequestration, in osteolysis and in epidural and paravertebral abscesses, signs evoking tuberculosis. MRI has a sensitivity of 96% and a specificity of 92% for infectious spondylodiscitis [9]. MRI allows a better visualization of soft tissue involvement especially pre- vertebral collections and their extension. These abscesses occur in T1-weighted and T2-weighted sagittal slices as a heterogeneous signal process (T1 signal and T2 hypersignal) [2, 8]. Some TB abscesses may be T2 hyposignal. The presence of fibrin and caseum [7]. However, unlike the CT scan, MRI does not show any calcifications within abscesses. These calcifications are important because their presence is unusual in non- tuberculous abscesses [1, 2]. The confirmation of the diagnosis is made thanks to the detection of BK in the abscess, or the scanned or surgical biopsy. However, in endemic areas and where there are signs of presumption, bacteriological or histological confirmation no longer seems to be essential for startingantibacillary treatment [7]. A bundle of convergent arguments makes it possible to retain the diagnosis: the notion of contagion, the positivity of the intradermoreaction, the radiological aspect, the existence of other localizations, the positivity of the GenExpert test.
We started a corticosteroid therapy as soon as we noticed a worsening of the patient's neuro-vegetative state, which made it possible to stop its progression with a partial regression of the inflammation at MRI on day 15. Kobayashi had the same therapeutic attitude with a similar result [11]. Medical treatment may be sufficient by antituberculous chemotherapy. The need for a 6-month cervical immobilization or more remains the norm for most authors [5, 7, 12, 13, 14]. Surgical treatment by anterior or posterior arthrodesis is indicated in cases of bone destruction with instability or in case of spinal cord compression [13, 14, 15, 16]. For ourpatient posterior arthrodesis by atlantoaxial lacing was performed. Evolution is more often favorable under medical treatment. The progression of bone lesions under medical treatment is rare [8].
Conclusion
Sub-occipital tuberculosis remains exceptional, despite the frequency of osteoarticular tuberculosis in our developing countries. It exposes to serious neurological complications. CT and MRI are diagnostic tools of paramount importance when dealing with sub-occipital tuberculosis. On the other hand the diagnosis must be early, confirmed by histopathological arguments but sometimes retained by elements of presumption. The treatment is medico-surgical in case of bulbo-medullary involvement. Evolution is most often favorable.
References
-
Akhaddar A, Chakir N, El Hassani M, El Quessar A, Jiddane M, et al. (2000) Mal de Pott sous occipital. Journal of Neuroradiology 27(2): 144-149.
-
Yahyaoui S, Majdoud S, Zaghouani H, Ben Fradj H, Bakir D, et al. (2013) Une localisation exceptionnelle de la tuberculose vertébrale Mal de Pott sous- occipital. Pan African Medical Journal. 14: 163.
-
Magnet M, Thierry A, Couaillier JF, Tavernier C, Strauss J (1984) Ostéite tuberculeuse de l’atlas. À propos d’une observation. Rev Rhum Mal Ostéoartic 51: 273-275.
-
Strecken J, Boissonnet H, Manzo L, Pheline C, Dobbelaer P, et al. (1987) Mal de Pott sous-occipital. Neurochirurgie 33: 482-486.
-
Akhaddar A, Gourinda H, Gazzaz M, Elmadhi T, Elalami Z, et al. (1999) Mal de Pott sous-occipital chez l’enfant. Rev Rhum 66: 851-854.
-
Kanaan IU, Ellis M, Safi T, Al Kawi MZ, Coates R (1999) Craniocervical junction tuberculosis : a rare but dangerousdisease. Surg Neurol 51(1): 21-25.
-
Allali F, Benomar A, EL Yahyaoui M, Chkili T (2000) Mal de pott sous occipital : trois cas. Rev Rhum 67: 641-645.
-
El Abbassi Skalli A, Talaoui M, Elamraoui F, ELouardi Z, Chikhaoui N (2006) Mal de pott sous occipital : A propos d’un cas. J Radiol 87: 63-65.
-
Augier A, Zrig H, Roqueplan F, Brauner M, Dumas JL (2008) TDM et IRM de la tuberculose de la jonction crânio-vertébrale : à propos de 5 cas. J Radiol 89: 585- 589.
-
Ibahioin K, Ait Ben Ali A, Choukri M, Sami A, Achouri M, et al. (2001) Sub occipital tuberculosis: a case report. Neurochirurgie 47: 66-68.
-
Nobusuke Kobayashi, Shunji Asamoto, Hiroshi Doi, Yukio Ikeda, Kiyoshi Matusmoto, (2003) Spontaneous regression of herniated cervical disc. The Spine Journal 3(2): 171-173.
-
Vlach O, Cienciala J (1990) Tuberculosis of the upper cervical spine. Acta Chir Orthop Traumatol Cech 57: 318-321.
-
Valaskatzis E, Govender S (1996) Tuberculosis of the craniocervicaljunction : two case reports. Eur Spine J 5: 140-142.
-
Fang D, Leong JC, Harry S, Fang Y (1983) Tuberculosis of the upper cervical spine. J Bone Joint Surg 65B : 47- 50.
-
Roche PH, Malca SA, Pellet W (1993) Spondylodiscite tuberculeuse. Éléments du diagnostic et intérêt de L’IRM. À propos d’une localisation cervicale. Neurochirurgie 39: 248-253.
-
Lifeso R (1987) Atlanto-axial tuberculosis in adults. J Bone Joint Surg 69(2): 183-187.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results