Mosaicplasty in Osteochondritis Dissecans of Femoral Condyles about 8 cases
Introduction: Osteochondritis dissecans of the femoral condyles is a subchondral bone necrosis, rare, more or less extended. The osteochondral fragmentation that results from it is responsible for very invalid pain and joint dysfunction. The aim of this work is to evaluate the clinical, radiological and evolutionary aspects of patients operated for osteochondritis dissecans of the femoral condyles by the technique of mosaicplasty at Order of Malta’s Hospital Center in Dakar CHOM. Patients and method: This is a retrospective, single-center study over a period of 67 months, involving 8 patients (6 men and 2 women). The average age was 25 years and the average BMI 22.93. Standard radiography has been performed in all our patients. 2 patients had MRI and 1 patientdid a CT. The collected data were the time of care, the IKDC score, the ICRS score and the Hughston / SFA score. The following characteristics of the lesion - the surface and the location - were also studied. Intraoperatively, the number and diameter of the pads, the location of the donor site and the associated operative procedures were recorded. At last follow-up, patients were assessed according to the Hughston functional and radiological scores, and IKDC. All the patients were immobilized for 6 weeks and benefited from the re-education sessions. Results: At an average follow-up of 36.5 months, the subjective results of the patients were very satisfactory in 62.5% of the cases and the clinical results according to the IKDC were excellent. Healing of osteochondral lesions was achieved in all our patients and 75% were in stage IV according to the radiological Hughston score.
Introduction
Osteochondritis dissecans of the femoral condyles is a subchondral bone necrosis, the osteochondral fragmentation that results from it is at the origin of very disabling pain and articular dysfunction. It is a very rare affection, whose exact etiology is unknown. It is certainly multi-factorial, mechanical and vascular factors being in the foreground. It is arthrogenic when healing has not been achieved [1]. We resort to surgery for osteochondral lesions reparation through bone grafting and osteosynthesis. When the fragment is detached or impossible to fix, you caneither leave the osteocartilaginous defect in the state or try to fill it. Many techniques are possible: mosaicplasty, chondrocyte transplant, allograft which have not yet proven their longevity. Mosaicplasty involves removing osteochondral grafts at a donor site and transferring them to the osteochondral defect. It has many theoretical advantages: respect of the radius of curvature of the articular surface, integration of the cancellous bone part of the graft that merges with the recipient cancellous bed and integration of the transplanted cartilage with the adjacent hyaline cartilage via fibrocartilage forming between the different grafts from the sub-chondral subsoil [2, 3]. The purpose of our work was to evaluate the clinical, radiological and evolutionary aspects of patients operated for osteochondritis dissecans femoral condyles by mosaicplasty technique at orderof Malta’s Hospital Centerin Dakar.
Patients and Method
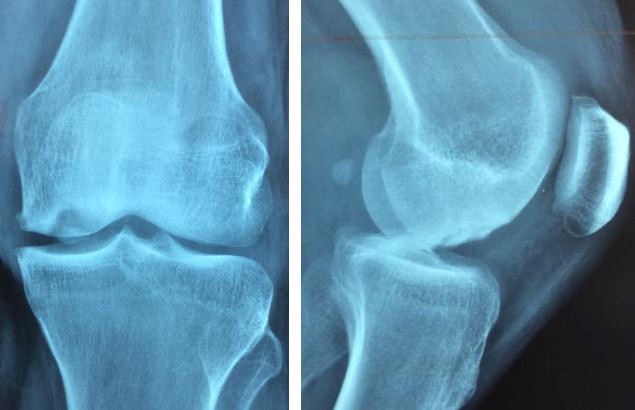
This is a single-center retrospective study with consecutive recruitment on a continuous series of eight patients from different professions (6 men and 2 women) all of them operated on by senior surgeons between January 2011 and July 2016. The average age was 25 years (16 years old - 36 years old). Mean BMI was 22.93 kg / m2 (20.2-25.95). The concept of trauma was found in 2 patients, one patient had 3 sessions of corticosteroid infiltration in his antecedents. The average duration of evolution was 2.5 years (1 month - 5 years); while the average duration of care was 75.9 days (14 - 200 days). All patients had pre- and postoperative medical imaging reports using standard radiography (Figure 1). Two patients also had MRI (Figure 2) and one patient had a CT scan. The collected data was: the IKDC score [4], the ICRS score [5] and the Hughston score modified by the SFA [6]. The following characteristics of the lesion were also studied: the surface, the appearance of the Bedouelle classification [1]. The number and diameter of the pads, the location of donor sites, and the associated operative procedures reported Intraoperatively. Postoperatively, all patients were immobilized and the maximum delay to stand on both feetwas 45 days. At the follow up, the functional criteria were Hughston's score, the ICRS score and the subjective IKDC score. The radiological results were assessed according to the radiographic Hughston score [6, 7].

Surgical Technique
In order to perform the osteochondral graft, we resorted to an ancillary from Arthrex (Figure 3). First, the approach was Para patellar medial or lateral depending on the localization of the lesion with arthrotomy, knee exploration and lesion assessment (Figure 4).



The first step consists in debridement of the margins and the bottom of the lesion in order to evaluate their dimensions and depth. The next step is to drill the recipient site, then the corresponding osteocartilaginous grafts are taken from the donor site (internal and external trochlea) using a specific trephine.
The detachment of the graft is done by rotational movements (Figure 5). The insertion of the grafts is done one by one by means of a graduated mandrel through a perforated cannula, in order to control the progression and to adjust the insertion height of the grafts (Figure 6). The patient is temporarily immobilized in a removable splint for analgesic purposes. The patient will be able to stand on both feet 45 days later. Anticoagulants at a


preventive dose are prescribed during this period. Rehabilitation is started immediately in the form of joint lapping without limit of amplitude and by mobilizing the patella. Quadriceps open-chain work is not allowedin order to preserve the patellofemoral joint. The patient could resume sports activities gradually starting from the sixth month.


Results
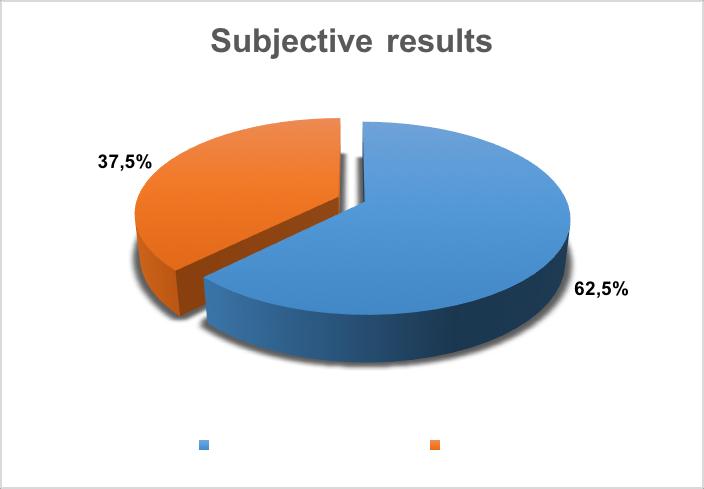
The mean follow up was 36, 5 months (6 – 67 months). Patient’ssatisfaction is represented in figure 7 below.
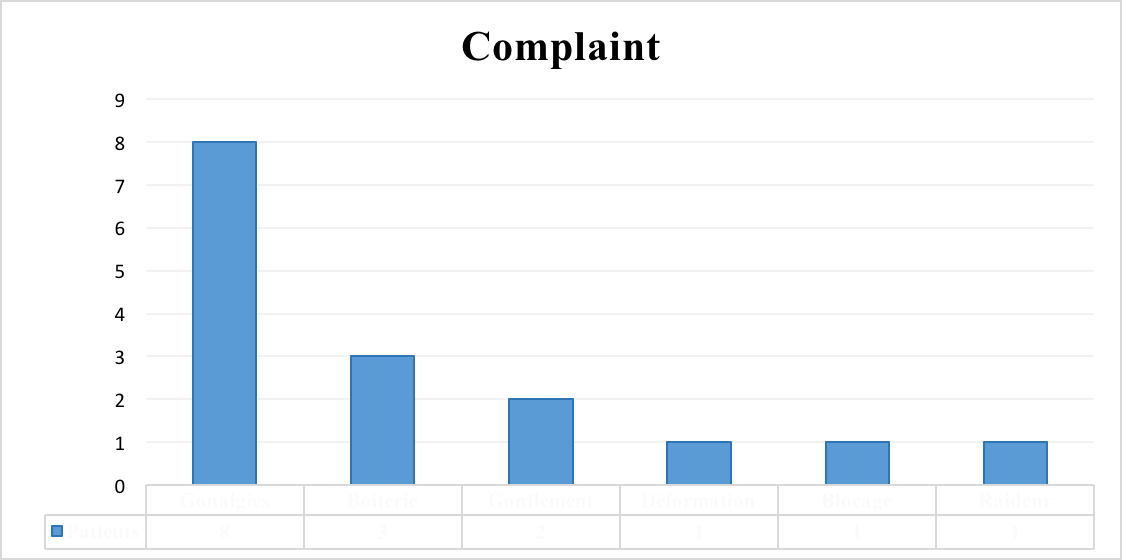
Pain was the main complaint and was found in all our patients, followed by limping and swelling resulting in a flare of hydarthrosis (Figure 8).
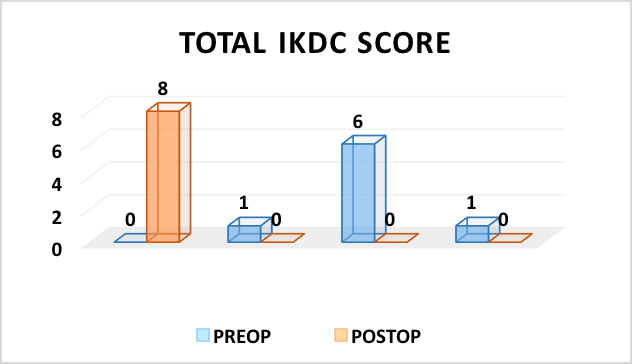
The mean subjective IKDC score (Figure 9) increased from 63 (55-70) before surgery to 96.25 (90-100) postoperatively. Figure 10 shows the evaluation of the
IKDC Score
IKDC scores before and after the intervention, which was excellent in all our patients.
Chondral lesions were found 7 times out of 8 on the medial femoral condyle and they were classified in stage Iaof Bedouelle in 37.5% (Figure 11).
BEDOUELLE'S CLASSIFCATION
Stage IV
Patients were classified predominantly Grade 3 of the ICRS score in 62.5% of cases (Figure 12). The average area of the lesions was 1.75 cm 2. Samples were taken from the lateral trochlea except in one case (medial trochlea). The size and number of pads according to the lesion size are reported in Table 1.
ICRS SCORE
The only intervention associated with mosaicplasty was a tibial osteotomy valgization.
Grade 2
25% Figure 12: Division of patients according to the ICRS score.
| Patient | Patient | Patient | Patient | Patient | Patient | Patient | Patient | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |||||||||||||||||
| Surface (square cm) | 1.52 | 1.3 | 1.8 | 1.52 | 1.68 | 3.3 | 1.2 | 1.8 | ||||||||||||||||
| Number of plots | 3 | 3 | 3 | 3 | 3 | 4 | 3 | 3 | ||||||||||||||||
| Diameter of plots (mm) | 6/8/2008 | 10 | 10 | 10/8/2008 | 10 | 20 | 10 | 10 |
Table 1: Size and number of plots according to the size of the lesion.
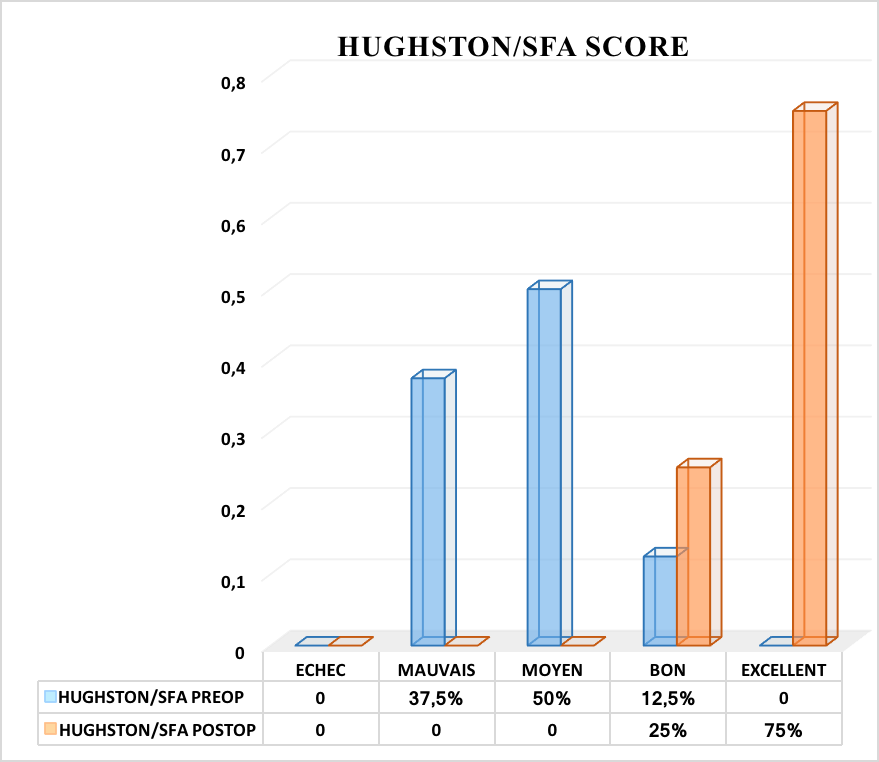
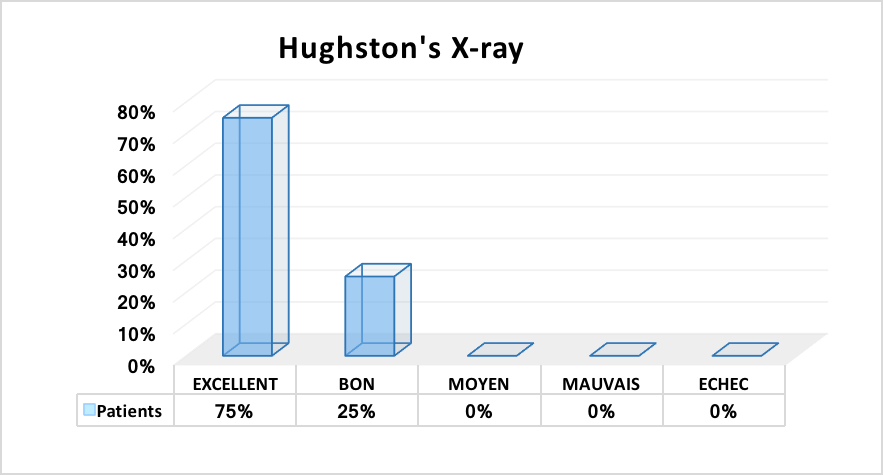
The functional Hughston score modified by the French Arthroscopy Society and the Hughston radiological score were all excellent at the follow up in 75% of cases (Figures 13 and 14).
Discussion
The subjective results, after an average follow-up of 36.5 months, showed that our patients were very satisfied with the final functional result, notably improvement of pain and complete recovery of knee mobility in 62.5% of cases. These results are comparable to those of Breda [8] and Marcacci [9] which found respectively 60% and 65.2%; while Ollat [10] and Solheim [11], had higher results 81.8% and 77%. Mean IKDC scores were excellent at follow-up, from 63 preoperatively to 95.62 postoperatively. Results which are slightly higher than those of found in the literature, Lazar [6], Lefort [7] and Ollat [10] found respectively 75, 56; 86 and 76.4. Our excellent 75% postoperative Hughston / SFA functional score remained superior to Ollat [10], who found 22% of excellent results out of 142 patients but his results are inferior to those of Lazar [6], who found 84% of excellent result out of 53 patients,. MRI is the examination of choice in the follow-up of osteointegration of osteochondral grafts. It allows appreciating in the first months, the consolidation of the deep graft and the scaring on the surface [12, 13]. Due to lack of resources, we were unable to perform MRIs for a better assessment of the osteointegration of the grafts. Thus in our series, standard radiography allowed us to appreciate this osteointegration. The healing of osteochondral lesions with a normal radiological image was obtained in all our patients with 75% excellent results at stage IV of the Hughston radiological score. Our results are identical to those of Lazar [6]. 87% of the lesions were located on the medial femoral condyle. Ollat [10] and Lefort [7], found respectively 75 and 70%, while Solheim [11, 14], in his two works found 58 and 60%. This difference could be explained by the fact that, not only the size of their sample was larger, but also by the diversity of location of chondral lesions on the knee in the same study. The lesions were classified Bedouelle stage III in 37% of the patients. These results are similar tothose of Lefort [7], which found 31% stage III and 38% stage IV in his work.
Osteochondral lesions were classified as Grade 3 according to the morphological classification of the ICRS in 63% of cases. Results which are similar tothose found in the literature. Lazar [6], Marcacci [9], found respectively 56% and 62% of Grade 3, while Ollat [10], found 73% of Grade 4.
The size of the defects was between 1.5 - 2 cm2 in 62.5%. The average surface was 1.75 cm 2 (1.08 and 3.3). Results slightly lower compared to data in the literature (Table 2).
| Average square cm2 surface | Square cm2 extremes | |||||
|---|---|---|---|---|---|---|
| Ollat [10] | 2.29 | 0.3 – 12.25 | ||||
| Lefort [7] | 2.44 | 0.34 – 8 | ||||
| Solheim [11] | 3 | 1 – 5 | ||||
| Marcacci [9] | 2.1 | 1.8 – 2.5 | ||||
| Christel [15] | 4.6 | 1 – 12 | ||||
| Our Series | 1.75 | 1.08 – 3.3 |
Table 2: comparison of the size of lesions.
These results are only partially comparable to ours because of the differences in the selection of patients with a much larger sample in these authors. In our series, the average number of plots used was 3 and the average diameter was 11.5 mm. Our results are similar tothose of Ollat, Solheim and Lefort [7, 10, 11]. Our subjective results (62.5%) are inferior to those of Lefort [7] who used the techniques of perforations, fixation by pins or screws, removal of the osteochondral fragment, transplantation of autologous chondrocytes ina multi centric series but ours, are superior to those of Dubrana [16], who used the micro fracture technique. On the other hand on the functional field, we have a better IKDC score (95.62) (Table 3). These results are explained by our reduced sample and our limited follow ups. These findings testify the accuracy of mosaicplasty compared to other techniques.
| Mean follow up | Subjective Results | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of cases | IKDC | |||||||||||
| (year) | (%) | |||||||||||
| Perforation [7] | 84 | 5.5 | 80 | 90 | ||||||||
| Fixation [7] | 95 | 5 | 67 | 68 | ||||||||
| Ablation of fragment [7] | 276 | 4.7 | 70 | 79.8 | ||||||||
| Autologouschondrocytes graft [7] | 25 | 4.7 | 96 | 82 | ||||||||
| Mosaicplasty [7] | 98 | 3 | 87 | 86 | ||||||||
| Microfractures [17] | 29 | 3 | 49 | - | ||||||||
| Our series | 8 | 3 | 62.5 | 95.62 |
Table 3: Comparison with other techniques.
Conclusion
Mosaicplasty, or mosaic osteochondral graft, is a surgical technique in the treatment of osteochondral loss. Overall, the subjective results of our patients were very satisfactory in 62.5% of cases, with a disappearance of pain and a complete recovery of knee mobility. The IKDC score was excellent postoperatively with an average value of 95.62. The Hughston / SFA functional score was excellent in 75% of cases. Scarring of the chondral lesions and the radiography were all normal at the follow-up with 75% excellent results at stage 4 of the Hughston radiological score.
References
-
Moyen B, Laptoiu D, Lefort G, Lerat JL (2006) Ostéochondrite disséquante des condyles fémoraux. EMC-Appareil locomoteur, Paris.
-
Ollat D, Lebel B, Thaunat M, Jones D, Mainard L, et al. (2011) Greffes ostéochondrales en mosaïque du genou : Résultats à moyens termes de la série multicentrique de la SFA. Rev Chir Orthop Traumatol 975: S389-S396.
-
Hangody L, Kish G, Karpati Z, Eberhard R (1997) Osteochondral Plugs: Autogenous osteochondral Mosaïcplasty for the treatment of focal chondral and osteochondral articular defects. Oper Tech Orthop 7(4): 312-322.
-
Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M et al. (2001) Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 29(5): 600- 613.
-
Slauterbeck JR, Kousa P, Clifton BC, Naud S, Tourville TW, et al. (2009) Geographic mapping of meniscus and cartilage lesions associated with anterior cruciate ligament injuries. J Bone Joint Surg Am 91: 2094- 2103.
-
Lazar AM, Larbaoui MK (2014) Prise en charge des lésions chondrales et ostéochondrales dans le service de chirurgie orthopédique « B ». Hôpital central de l’armée HCA. 21e congrès de la SACOT.
-
Lefort G, Moyen B, Beaufils P, De Billy B, Breda R, et al. (2006) L’ostéochondrite disséquante des condyles fémoraux : analyses de 892 cas. Rev Chir Orthop Traumatol 92 (2): S97-S141.
-
Breda R, Marchaland JP, Ollat D, Versier G (2009) Résultats à moyen terme du traitement des ostéochondrites disséquantes du condyle fémoral par mosaïcplastie. À propos de 12 cas 82e Réunion annuelle de la SO.F.C.O.T 209.
-
Marcacci M, Kon E, Zaffagnini S, Iacono F, Neri MP, et al. (2005) Multiple osteochondral arthroscopy grafting (Mosaïcplasty) for cartilage defect of the knee: prospective study results at 2 – years follow-up. J Arthroscopy Rel Surg 21(4): 462-470.
-
Ollat D, Lebel B, Thaunat M, Jones D, Mainard L, et al. (2011) Greffes ostéochondrales en mosaïque du genou : Résultats à moyens termes de la série multicentrique de la SFA. Rev Chir Orthop Traumatol 975: S389-S396.
-
Solheim E, Hegna J, Oyen J, Austgulen OK (2010) Osteohondral autografting (mosaïcplasty) in articular cartilage defects in the knee: results at 5 to 9 years. Knee 17: 84-87.
-
Cognault J, Seurat O, Chaussard C, Ionescu S, Saragaglia D (2015) Reprise de sport après autogreffe ostéochondrale en mosaïque des condyles fémoraux : 25 cas à 9 ans de recul moyen. Rev Chir Orthop traumatol 101: 215-220.
-
Robert H (2011) Restauration cartilagineuse du genou par le procédé de mosaïque plastie. Rev Chir Orthop Traumatol 97: 519-430.
-
Solheim E, Hegna J, Oyen J, Harlem T, Strand T (2013) Results at 10 to 14 years after osteochondral autografting (mosaïcplasty) in articular cartilage defects in the knee. Knee 20: 287-290_._
-
Christel P, Versier G, Landreau Ph, Djian P (1998) Les greffes ostéochondrales selon la technique de la mosaïcplasty. Maitrise-Orthop 76: 1-13.
-
Dubrana F, Mayer C, Casin C, Thaunat M, Ollat D, et al. (2010) Traitement des pertes de substances cartilagineuses du genou. Symposium SFA décembre.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results