A Balance between Art and Principle in Management Complex Femur Fracture
Complex fractures of proximal and distal femur often difficult to treat. Plating of segmental femoral shaft fractures is also an option, particularly when associated with peritrochanteric fractures, but associated complications. Although technically difficult, intramedullary nailing has been recommended by several studies and has demonstrated good results. The purpose of this review was to analyse our results with the interlocked nailing of complex fractures of the femur.
Introduction
Internal fixation of complex fractures of the femur has gained widespread acceptance in the past decade as implants and technology have improved. The rationale for internal fixation is that it restores anatomical alignment and allows early mobilization of the patient and the limb. However, stable internal fixation has been difficult to achieve [1]. The use of a plate to achieve osteo-synthesis of segmental fractures necessitates a wide operative exposure and extensive stripping of soft tissue, resulting in increased loss of blood and a longer operating time. The risk of infection is increased, failure of the plate is common, and the need for primary bone graft adds additional morbidity to the procedure. Due to the high rate of complications associated with this type of fixation, most traumtologists have advocated intramedullary nailing for complex femoral fractures. Conventional closed Kuntscher nailing eliminates unsightly scarring of the thigh, minimizes disruption of the soft tissues at the site of fracture, reduces the risk of infection, and restores anatomical alignment [2].
Materials and Methods
Between January 2016 and January 2017, 21 patients who had a complex fracture of the femur who were seen at Hospital Sultanah Aminah Johor, Malaysia and treated with interlock intramedullary nailing.
Results
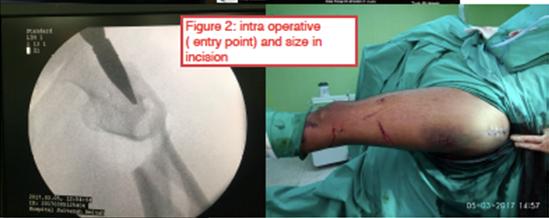
Table 1, Figures 1-3.
| Results | Value | ||||
|---|---|---|---|---|---|
| Total Case | |||||
| Subtrochanteric-Diaphyseal Intercalary Segment | 11 | ||||
| Diaphyseal-Supracondylar Intercalary Segment | 9 | ||||
| 21 | |||||
| Male/Female | 16/5 | ||||
| High Eenrgy Trauma | 18 | ||||
| Close/ Open Fracture | 18/3 | ||||
| Average Age | 37 | ||||
| Associated Injury | 47% | ||||
| Average Time To Nail | 56 Hours | ||||
| Average Operating Time | 95min | ||||
| Average Fracture Union | 28 Weeks | ||||
| Average Blood Lost | 179ml | ||||
| Closed / Open Reduction | 90%/10% | ||||
| Compilaction | |||||
| Non Union | 19% | ||||
| Delay Union | 5% | ||||
| Malunion | 32% | ||||
| Knee Stiffness | 27% | ||||
| Shorthening | 33% | ||||
| Ards Post Nail | 5% | ||||
| Average Follow-Up | 15 Months | ||||
| Average Rom | |||||
| Knee | 105 Deg | ||||
| Hip | 110deg |
Table 1: Patients treated with interlock intramedullary nailing at Hospital Sultanah Aminah Johor, Malaysia.


Discussion
Due to the high rate of complications associated with open reduction, most traumtologists have advocated intramedullary nailing for complex femoral fractures. Certain intraoperative techniques are essential, the starting hole is crucial, and care must be taken to ensure that it is within the piriformis fossa or Trochanteric entry and aligned with the long axis of the proximal femur in the AP and lateral fluoroscopic images. Several authors have discussed the theoretical risk of spinning the central fragment during reaming, thereby damaging the blood supply and delaying healing. In our experience, the strong attachment of the soft tissues along the lines as per prevents spinning in most patients. Obtaining and maintaining reduction is often difficult without an intact diaphysis to use as a template for reduction. Reduction devices commonly are required to obtain and maintain reductions. Mallets and spiked pushers, found in the pelvic reduction tray, are useful to push fragments into position.
Wiss, et al. [2] recorded that in six patients shortening of between 1.0 and 1.5 centimeters occurred. Unfortunately, when comminution exists at either fracture level, shortening cannot be prevented. From our review we noted shortening between 1.5 to 2.0cm, this degree of shortening did not prove symptomatic for any of these patients. Our malunion rate of 32% where, 11 degrees of angulation developed at the distal fracture site. None of these valgus deformities proved symptomatic. Three degrees of varus angulation were noted in one patient and 5 degrees of genurecurvatum, in another. Although these complications (minor malunion) were recorded, all were asymptomatic for the patients. Wu, et al. [3] reported varus / valgus angulation in 14 patients out of 112 unstable comminuted femoral shaft fractures. Dynamisation was performed in only nine of the 21 patients. The average time to dynamisation was 18.2 weeks. Anastopoulos G, et al. [4] reported 2 cases of delayed union out of 100 femoral shaft fractures which subsequently healed after dynamisation. Shortening after dynamisation was reported in some of these patients, in whom the comminuted femoral fracture was not sufficiently healed to resist axial loading. Non union in 4 patients (3 aseptic and 1 septic), 3 patient had exchange nail done and the fracture heal uneventfully. Another 1 case for septic non union removal of nail and antibiotic coted nail was done. Kempf and Grosse [5] reported 5 cases of non union (4 aseptic and 1 septic) in 52 patients. 4 cases of aseptic non-union healed after exchange locked Intramedullary nailing without bone grafting.
Wiss, et al. [2] have recorded that the most recent follow-up of the thirty-three patients, the average flexion of knee was 110 degrees. In our study we noted average knee ROM 105 degrees.
Conclusion
Complex fractures of proximal and distal femur often difficult to treat. Although technically difficult, intramedullary nailing has demonstrated good results with certain good intraoperative techniques.
References
-
Thoresen BU, Alho A, Ekeland A, Stromsoe KG, Folleras G, et al. (2002) Interlocking intramedullary nailing in femoral shaft fractures. A rport of forty- eight cases. JBJS 67(9): 1313-1320.
-
Wiss DA, Brien WW, Stetson WB (2007) Interlocked nailing for treatment of segmental fractures of the femur. J Bone and Joint Surg 72(5): 724-728.
-
Wu C, Chen W (2000) Healing of 56 segmental femoral shaft fractures after locked nailing. Acta orthop scand 68: 494-500.
-
Anastopoulos G, Asimakopoulos A, Exarchou E, Pantazopoulos T (1993) Closed interlocked nailing in comminuted and segmental femoral shaft fractures. J Trauma 35(5): 772-775.
-
Kempf A Grosse, Beack G (1985) Closed locked intramedullary nailing, Its application to comminuted fractures of the femur. JBJSA 67(5): 709-720.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results