Ankylosing Pelvitrochanteric Heterotopic Ossification in a Patient with Spinal Tuberculosis
Heterotopic ossification (HO) is defined as the presence of lamellar bone at locations where bone normally does not exist. This syndrome is most commonly seen following neurological disorders such as traumatic brain or spinal cord injury, or following joint surgery or severe burns. Patients with neurogenic HO develop lesions around larger joints. The hip is the most common location, followed by the knees and elbows but complete ankylosis is a rare presentation. Radiation therapy, surgical resection, biphosphonates and various non-steroidal anti-inflammatory drugs (NSAIDs) have been reported and advocated as efficacious methods for management of HO. We report a case of ankylosing pelvitrochanteric HO in a patient with spinal tuberculosis (TB) treated successfully with surgical excision, postoperative radiation therapy and indomethacin.
Case Presentation
A 56-year-old paraplegic patient referred to our clinic with a significant restriction of left hip movement. The patient suffered T8–T9 hemiplegia due to TB spine 2 years ago. The patient recovered slowly with anti TB medicaton which he completed for the duration of 12 months. During the last follow up, the patient developed total ankylosis of the left hip that prevents of this basic daily activity (sitting position, perineal hygiene and etc.).
On physical examination, left hip was held in the extended position because of large hard mass extending from iliac crest down to the upper third of the thigh, causing fixation of the hip joint in the extended position. It was impossible to flex or abduct the hip joint to maintain a normal sitting posture and perform perineal cleaning.
Investigations
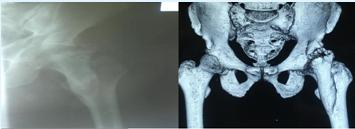
Radiographical examination revealed diffuse HO and ankylosis of the hip (Figure 1A). A CT examination showed pelvitrochanteric HO sparing the hip joint itself (Figure 1B). Bone scintigraphy showed very high incorporation around the right hip (Figure 2A, 2B).
Treatment
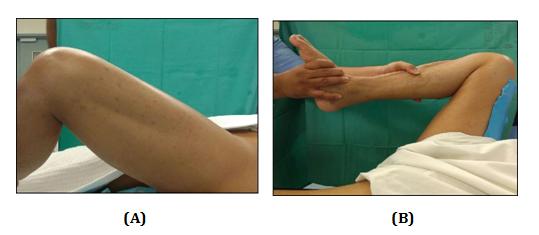
Surgical resection of HO was carried out using anterior approach. There was a clear demarcation zone between the posterior periosteum of the mass and the anterior hip joint capsule (Figure 3). The HO surrounding the lower third of the femur was not disturbed. On completion of the excision of the cephalad mass (Figure 4), we were able to flex and abduct the hip joints to 100° and 50°, respectively, on the operating table (Figure 3) [1, 2]. The total blood loss was approximately 500 ml. Postoperative hip radiographs showed clearance of the ankylosis. Prophylaxis for recurrence of HO included postoperative single-dose radiation (7 Gy) was given 24 hours post surgery and oral indomethacin at a dose of 150 mg/day. His postoperative course was uneventful without wound complications. Passive movement of the hip joint was carried out throughout the healing period. 2 weeks following surgery the patient was able to bend forward and sit with hip in flexion 90 degrees. At the final follow- up 8 months after surgery, the range of hip movements was still preserved with no sign of recurrence observed on direct radiographs.


Discussion
Heterotopic bone formation begins within 2 months after neurological injury and is usually fully developed by 2 years. Sometimes, the heterotopic bone may be massive and cause complete ankylosis of the affected joint. A limitation of the range of joint motion may have serious consequences for daily functioning of people who are already severely incapacitated because of their original lesion. Increased contractures, pressure ulcers and increasing pain further compromise the patient's capabilities [3]. Surgery is the only treatment that is capable of removing an already formed bone, but complications frequently occur such as deep venous thrombosis, infections, pressure ulcers and major blood loss. Moreover, surgical resection alone is associated with an extremely high recurrence rate. Consequently, surgical resection must always be combined with NSAID or postoperative radiation therapy. Indications for surgery include improvement of the range of motion, for example, to enable patients to sit properly, reduction of contractures, prevention of pressure ulcers and intractable pain. The optimal timing of surgery is still controversial. Usually, it is suggested to wait until complete maturation of the ectopic bone, mainly to avoid recurrences. Maturation is manifested by normalization of the scintigraphic findings and usually takes 12–18 months. There is a growing tendency to pay more attention to the patients’ neurological condition and to delay resection until he or she is maximally recovered from brain or spinal cord injury [4]. Three-phase bone scintigraphy is used for both diagnostic and therapeutic follow-up purposes, and is the most sensitive imaging modality for early detection of HO. The first two phases are indicative of hyperaemia and blood pooling, which are the precursors of an ossification process. Bone scintigraphy is usually positive after 2–4 weeks. It can also be used to assess the maturity of HO. Serial bone scans are used to monitor the metabolic activity of HO so as to determine the optimal timing for surgical resection, and to predict postoperative occurrence. Before surgery, MRI and CT are valuable to assess the relation with blood vessels and peripheral nerve structures [5]. Although early surgical excision before maturation has a high risk of recurrence, in case of complete ankylosis it may be compulsory for the patient's daily life quality. Postoperative low-dose radiotherapy and indomethacin combination is effective to prevent recurrences.
References
-
McCarthy EF, Sundaram M (2005) Heterotopic ossification: a review. Skeletal Radiol 34(10): 609- 619.
-
Garland DE, Blum CE, Waters RL (1980) Periarticular heterotopic ossification in head-injured adults. Incidence and location. J Bone Joint Surg Am 62(7): 1143-1146.
-
Vanden Bossche L, Vanderstraeten G (2005) Heterotopic ossification: a review. J Rehabil Med 37(3): 129-136.
-
Moore TJ (1993) Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 7(1): 11-4.
-
Jensen LL, Halar E, Little JW, Brooke MM (1987) Neurogenic heterotopic ossification. Am J Phys Med 66(6): 351-363.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results