Low Incidence of Secondary Hemorrhage after Single Level Lumbar Decompression
Secondary hemorrhage is a complication which can develop after spine surgery. To prevent progressive neurological deficit caused by an expanding hematoma, drains are inserted to build an outflow for the trickling blood. Minimally invasive spine surgery reduces local tissue damage and associated complications. In a prospective follow up study 882 patients receiving lumbar single level decompression surgery were assessed for a postoperative hemorrhage. Patients undergoing single level decompression for degenerative spinal stenosis and / or lumbar disk herniation were included. Three out of 882 patients (0.34%) developed a secondary hemorrhage with the indication for revision surgery. Second surgery was done on the same day in one case and after 5 and 8 days in the two other patients, respectively. In all patients persisting sciatic pain was the main indication. Increasing neurological deficit was observed in one patient immediately after surgery. Secondary hemorrhage is a rare complication after minimally invasive lumbar spine surgery. Even without inserting any drainage system the rate for compression related neurological deficit is very low.
Introduction
Lumbar decompression is one of the most frequent operations for spinal pathology. The main indication for decompression is spinal stenosis or a disk herniation. Nowadays this procedure is performed through minimally invasive procedures using an operative microscope or an endoscope. Due to these minimally invasive methods the complication rate in general has reduced in comparison to older open approaches [1]. After laminectomy a local hematoma is often observed -, but in most cases it is clinical not apparent [2]. These small hematomas don’t need any additional treatment. The rate of advanced intraoperative bleeding is estimated at 5.5% and depends on the experience of the surgeon [3]. After surgery, an expanding secondary hemorrhage can develop over hours or sometimes over days. Even though the risk is very low this expanding hematoma can cause progressive neurological deficit through compression of nerve roots or the Cauda Equina [4]. The rate for postoperative hematoma which has to be evacuated to improve the clinical symptoms is very low, at 0.4% [4]. In certain situations at the end of surgery drains are inserted into the operative field to build an outflow for the trickling blood. Minimally invasive spine surgery is thought to reduce local tissue damage and bleeding. The microscopic or endoscopic view allows the local identification and closure of damaged vessels. Nevertheless many spine surgeons insert local drains to minimize the risk of a compressive secondary hemorrhage. The aim of this study was to clarify the incidence of clinically relevant secondary hemorrhages after single level lumbar spine decompression and to find subgroups with increased risk for such complications.
Patients and Methods
In a prospective follow-up study, 882 patients receiving lumbar single level microsurgical decompression were monitored for postoperative hemorrhage from June 2009 to 2011. Only patients with single level decompression for degenerative spinal stenosis or lumbar disc herniation were included in the study. Patients requiring additional stabilization were excluded. The analysis included concomitant diseases, pre-operative anticoagulation and intra-operative blood loss. For clinical evaluation, pre and postoperative VAS and degree of paresis (JANDA classification) were used. Patients were evaluated for the first time in the anesthetic recovery room immediately after the operation and 2 and 4 days after surgery, respectively. No single patient received a postoperative drain after the intervention.
Results
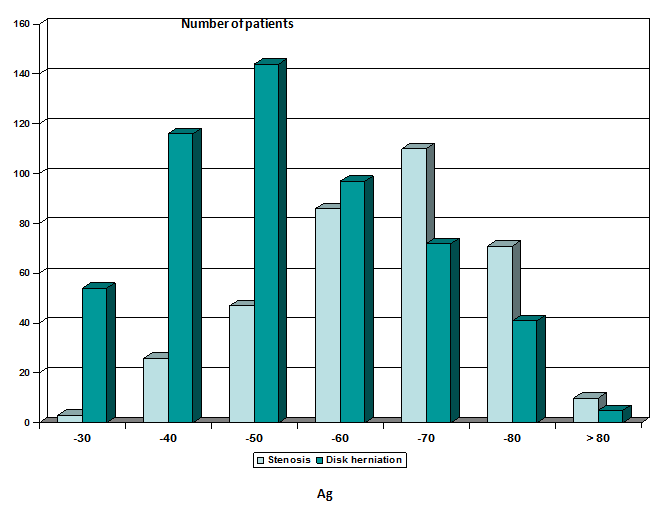
In 528 patients the indication for spine surgery was a one level disc herniation. 351 patients had spinal stenosis. As expected we saw a higher age in patients suffering from spinal stenosis compared to those with a lumbar disc herniation (Figure 1).
Out of 882 patients 52% were female and 48% were male respectively. From these patients 317 had a BMI of more than 30 (61% male, 39% female) (Table 1). Preoperatively 132 patients received anticoagulation treatment. Most of these patients received low dose aspirin therapy (92%).
| Peripheral artery disease | 17 |
| Coronary heart disease | 39 |
| Diabetes mellitus | 19 |
| Obesity (BMI > 30) | 317 |
| Neurodegenerative Disorders | 5 |
| Preoperative anticoagulation | 132 |
Table 1: Concomitant Diseases.
Table 1: Concomitant Diseases. These patients stopped the medication 7 days before surgery. Eight percent of the anticoagulation patients received Cumarine. In these patients the treatment was changed to low molecular heparin injections. For surgical intervention to proceed, the Quick´s value had to increase to 80%. To analyse the intraoperative situation we measured the duration of the surgery and the amount of blood loss during the procedure. Additionally any sudden intraoperative change of systolic blood pressure was recorded. From this we defined two groups: 0 = no sudden increase, 1 = sudden increase. The critical value was determined as an increase of the systolic blood pressure of 30% or more in less than 5 minutes (Table 2).
| Stenosis | Disc herniation | |
|---|---|---|
| Duration of surgery | 48 +/- 20 minutes | 35 +/- 12 minutes |
| Blood loss | 62 +/- 40 ml | 35 +/- 20 ml |
| Sudden increase of blood pressure | 17 | 29 |
| VAS back preoperative | 5 +/- 3.2 | 4.6 +/- 2.7 |
| VAS back postoperative * | 4.2 +/- 1.3 | 5.2 +/- 1.9 |
| VAS leg preoperative | 4.1 +/- 3.2 | 6.4 +/- 2.8 |
| VAS leg postoperative * | 2.4 +/- 0.9 | 0.8 +/- 1.1 |
Table 2: Intraoperative Evaluation.
Table 2: Intraoperative Evaluation. *Anesthetic recovery room Three out of 882 patients (0.34%) developed a secondary hemorrhage with the indication for revision surgery. Two patients were treated for disc herniation, one patient for spinal stenosis. Second surgery was done on the same day in one case after removal of a disc herniation. Still in the anesthetic recovery room after the surgery the patient suffered from severe low back pain (VAS 8.3). These values were higher in comparison to the mean values of the entire group. Radicular pain persisted in the same intensity as preoperatively. One hour after surgery the patient showed increasing neurological deficit. As a result of these symptoms revision surgery was performed within two hours of the first operation. A local hematoma was removed. The two remaining patients had second surgery at 5 and 8 days after the first intervention. Also here significant low back pain persisted. Both patients showed VAS values for low back pain (VAS 5.2 and 4.7) as well as leg pain (VAS 6.9 and 5.8) which were ranked in the upper pain scale compared to the entire study group. In both patients the main indication for the delayed revision surgery was persisting sciatic pain (Tab. 3). In these two patients a control MRI was done before second surgery.
signs Case 1 +++ + + + -
| Case 1 | Case 2 | Case 3 | |
| Surgery for disc herniation | + | - | + |
| Surgery for spinal stenosis | - | + | - |
| PAD | - | - | - |
| CHD | - | - | - |
| Diabetes mellitus | - | + | - |
| Obesity (BMI > 30) | 32 | 37,4 | 33.3 |
| Neurodegenerative Disorders | - | - | - |
| Preoperative anticoagulation | - | - | - |
| Duration of surgery | 31 min | 52 min | 38 min |
| Blood loss | 15ml | 32ml | 20 ml |
| Changes in blood pressure | - | - | - |
Table 3: Factors Influencing Secondary Hemorrhage.
Discussion
If other reasons related to the surgical procedure, e.g. intraoperative damage of nerve roots, have been excluded, an epidural hematoma should be suspected, if a new postoperative neurological deficit occurs immediately after the procedure. According to several studies the overall complication rate in minimally invasive lumbar decompression surgery is 4% [5]. Focusing on postoperative secondary hemorrhage this rate is even smaller with 0.4% [6, 7]. In most of the studies postoperative hemorrhage is defined as a complication if some neurological deficit occurs. Remaining or increased postoperative pain due to secondary hemorrhage is included only in some assessments. Therefore a secondary hemorrhage rate of 0.34%, which was measured in our study, is very low. Even without any local drainage after surgery this rate was below the amount published in the literature. Looking for predictors which are connected with a secondary hemorrhage, only a BMI of more than 30 was found in all three cases. Given the increasing number of obese people in the patient population it will become difficult to use this as an exclusion factor for surgery. Low back pain only or local recovery pain is very common after surgical intervention. Most patients complain about this pain immediately after the procedure. If patients do not show an additional neurological deficit, the diagnosis of a secondary hemorrhage may become more difficult in those patients. Our results showed that pain intensity rated in the upper third of the VAS scale is an indicator for a secondary hemorrhage. In those cases the patients should be monitored closely in the anesthesia recovery room. If a progressive impairment is observed, revision surgery should be performed immediately. For all other cases where pain improvement is delayed or does not occur after decompression an MRI control is recommended [8, 9].
Conclusion
Secondary hemorrhage is a rare complication after minimally invasive lumbar spine surgery. Even without inserting any drainage system the incidence of compression related neurological deficit is very low. These results suggest that lumbar drainage after single level decompression is no longer necessary. Significant back pain or radicular pain after decompression surgery raises the suspicion of a remaining compression. If the patient complains of severe pain immediately after surgery an urgent revision should be considered.
References
-
Wildförster U (1991) Intraoperative Komplikationen während lumbaler Bandscheibenoperationen. Neurochirurgia 34: 53-56.
-
Kotilainen E, Alanen A, Erkintalo M, Helenius H, Valtonen S (1994) Postoperative hematomas after successful lumbar microdiscectomy or percutaneous nucleotomy: a magnetig resonance imaging study. Surg Neurol 41: 98-105.
-
Haglund MM, Moore AJ, Marsh H, Uttley D (1995) Outcome after repeat lumbar microdiscectomy. British Journal of Neurosurgery 9: 487-495.
-
Kou J, Fischgrund J, Biddinger A, Herkowitz H (2002) Risk factors for spinal epidural hematoma after spinal surgery. Spine 27: 1670-1673. _5._ Davis RA (1994) A long-term outcome analysis of 984 surgically treated herniated lumbar discs. J Neurosurg 80: 415-421
-
Scavarda D, Peruzzi P, Bazin A, Scherpereel B, Gomis, P, et al. (1997) Postoperative spinal extradural hematomas. 14 cases. Neurochirurgie 43: 220-227.
-
Uribe J, Moza K, Jimenez O, Green B, Levi AD (2003) Delayed postoperative spinal epidural hematomas. Spine J 3(2): 125-129. _8._ Boukobza M, Guichard JP, Boissonet M, George B, Reizine D, et al. (1994) Spinal epidural haematoma: report of 11 cases and review of the literature. Neurorad 36(6): 456-459.
-
Janda V (1983) Muscle Function Testing. Butterworths, London, pp 29.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results