Low Intensity Pulsed Ultrasound (LIPUS) for Orthopaedic Trauma: A Pilot Study
Introduction: The incidence of non-union is 5% for all fractures. Non-operative biophysical modes to stimulate osteogenesis and fracture healing have explored electrical, laser and ultrasound modalities to varying degrees of success over the past few decades. Methods: This pilot study was undertaken at a District general hospital (DGH) in a publicly funded healthcare delivery system to assess the benefits and report the healing rate/success with use of Low intensity pulsed ultrasound (LIPUS) ExoGen device in delayed and non-unions of closed appendicular skeletal fractures. A standard device that delivered acoustic radiation at an operating frequency of 1.5 MHz with a temporal average power of 30 mW/cm2 and self-administered by the patient for 20mins/day for 250 sessions was used. Results: 11 adult patients enrolled into the study were followed-up until the end of their treatment and seven of them had clinical plus radiological union with excellent outcomes. The mean age of patients was 54.9years (range: 26 to 71y). The mean follow-up duration was 18.5months (range: 10.0 to 24.5m). The mean duration from sustaining the fracture to application of ExoGen to hasten osteosynthesis was 4.1months (range: 1.0 to 9.0m). Two patients warranted revision surgery to achieve fracture union. Of the remaining two patients, one with fibrous non-union was coping satisfactorily whilst a salvage procedure was proposed for another. Discussion: LIPUS was used as an ‘Alternative’ to surgery (and revision surgery) in all but one patient where it was used as an adjunct with surgery. There were no complications with its use and the healing rate was 63.6% (7/11 patients). There was an estimated cost savings of at least £10,000 in this small cohort of patients. Smoking status, high velocity trauma, advancing age or gender did not influence the outcomes.
Introduction
The global incidence of delayed union (DU) and non- unions (NU) reported in published literature is 5 – 10% [1]. They constitute a significant case-load/work burden to busy trauma units and are associated with high economic costs with reduced quality of life (QoL) [2]. Optimal healing and fracture union is influenced by several factors: i) Host profile (i.e. patient characteristics with co-morbidities); ii) Nature of injury (i.e. Open vs. Closed and Low vs. High velocity trauma etc...); and iii) Surgeon (i.e. operative execution with use of bone grafts vs. minimally invasive strategies etc...). Revision surgery is undertaken to achieve fracture healing and is fraught with complications. Alternative non-operative modalities to facilitate osteosynthesis explored over the past few decades are; i) Electrical stimulation; ii) Low lever laser therapy LLLT) and iii) Low intensity pulsed ultrasound (LIPUS) [3, 4, 5]. Other semi-interventional strategies reported in literature include: i) Bone marrow aspirate (BMA) and ii) Bone morphogenetic protein (BMP) injections to the fracture site [6, 7]. Injections into fracture site carry a risk of introducing infection and BMA carries a risk of donor site morbidity [8]. Local allergic reaction and hypersensitivity response to BMP is well known in published literature [9, 10]. A prohibitive cost with additional risk of causing potential infection has made BMP less attractive and not the first preferred mode of treatment choice for DU and NU. A recent systematic review reporting the results of LIPUS vs. LLLT found better results with LIPUS in both animal models and clinical studies involving patients [11].
LIPUS has been in vogue since late 1980s and has a proven safety profile without any reported complications/ adverse events. It was approved by the United States Food and Drug Administration(US-FDA) for DU and NU in 1994 [12]. The United Kingdom equivalent of US-FDA, the National institute of clinical excellence (NICE) has recommended its use in clinical settings as an experimental project approved by local clinical governance (CG) committee for managing challenging DU and NU [13]. Their approval was based on six published studies that included one randomized controlled trial (RCT), four systematic reviews and one cohort study. NICE recommends application of low intensity non-focused acoustic radiation of 1.5 MHz with pulse width of 0.2ms and repetition rate of 1KHz delivering an average intensity of 30mW/cm2 SATA (spatial average–temporal average).
The present study was undertaken at our District general hospital (DGH) as a pilot project with due CG approval to report our experience with use of LIPUS using a commercially available ExoGen device (Bioventus, Durham– North Carolina; USA) in a small cohort of patients who were recruited following an informed consent and followed-up till the end of their clinical care.
Our objectives were to report:
- The healing rate (HR) i.e. success with ExoGen in all closed appendicular skeletal fractures (i.e. both upper and lower extremities) where its use was felt to be desirable.
- Any adverse events/complications during the course of treatment.
Methods
The study included all adult patients (i.e. skeletally mature and age of ≥25years) with closed appendicular skeletal fractures treated over two years who exhibited signs of delayed healing and non-unions as determined by the treating Consultant Orthopaedic Surgeon given the patient’s unique co-morbidities profile, personal habits and fracture pattern configuration. We enrolled patients prospectively into this pilot study guided by inclusion vs. exclusion criteria as enumerated in Table 1. Informed consent was taken in all patients after providing them with patient information leaflets and explaining the uncertain nature/mechanism of achieving osteosynthesis with LIPUS and full disclosure of existing quality/evidence of published research. Participation was purely voluntary and refusal to be treated by LIPUS did not influence the clinical care/ongoing treatment re: fracture management in any of the patients.
| Inclusion | Exclusion |
|---|---|
| Skeletally mature adults aged ≥25years | Skeletally immature patients aged ≤25years |
| Upper and lower extremity fractures | Axial skeletal & infected fractures |
| Closed fractures | Open fractures |
| Fractures were >30days from date of injury | Fractures were ≤30days from date of injury |
| Inter-fragmentary fracture gap of ≤10mm | Inter-fragmentary fracture gap of >10mm |
| Nutritional and age related metabolic bone disorders (i.e. Vitamin D insufficiency and Osteopenia/Osteoporosis). | Metabolic bone disorders (other than nutritional and due to ageing). |
Table 1: Inclusion and exclusion criteria for our pilot study.
Whilst we identified 12 patients, one patient changed residence/moved out of our geographic area and was lost for follow-up. The final analysis and outcomes reported here is based on 11 patients. There is no consensus in published literature Re: the duration to call a fracture as ‘Delayed union’ and ‘Non-union’. Suffices to say that most agree that any fracture that hasn’t showed signs of healing/consolidation in a reasonable time and is unlikely to unite without some form of intervention (not necessarily operative) is labeled as Non- union. Similarly any fracture that hasn’t showed progressive signs of radiological healing expected over a course of 3 to 6 months to be labeled as Delayed union.
The Medical Physics department of our institute

procured the commercially available ExoGen equipment from the manufacturer. A standard device that provided 20mins/ day of pre-determined recommended acoustic radiation over 250 sessions was used in all patients. The treatment duration was extended in few patients (n=3) guided by clinical response and individual requirements. This included continued administration of same acoustic radiation in ≥325 instances to support osteosynthesis. The Standard ExoGen equipment used in our pilot study is illustrated in Figure 1. Support from the manufacturing company representative was available at all times during the course of the study. One nurse was trained/educated by the manufacturer to apply the ExoGen and deal with all patient queries.
All patients were followed-up till the end of the study and had one of the three outcomes:
- Clinical and radiological healing with pain-free status and bridging trabeculae plus sound consolidation at the fracture site in 3 out of 4 cortices on plain radiographs taken in orthogonal planes (i.e. AP and Lateral views).
- Non-union despite use of ExoGen warranting revision surgery and follow-up thereof until bony healing after operative intervention.
- Non-union despite use of ExoGen wherein the patient either: i) Declined further treatment or ii) Attempts at osteosynthesis was abandoned and salvage procedure was recommended. All patients were seen in the fracture clinic at serial intervals by orthopaedic surgeon and ExoGen trained nurse to monitor compliance with its use. Relevant imaging studies were obtained at each visit and Computed tomography (CT) scans were requested where necessary to aid in clinical management and optimize care.
Results
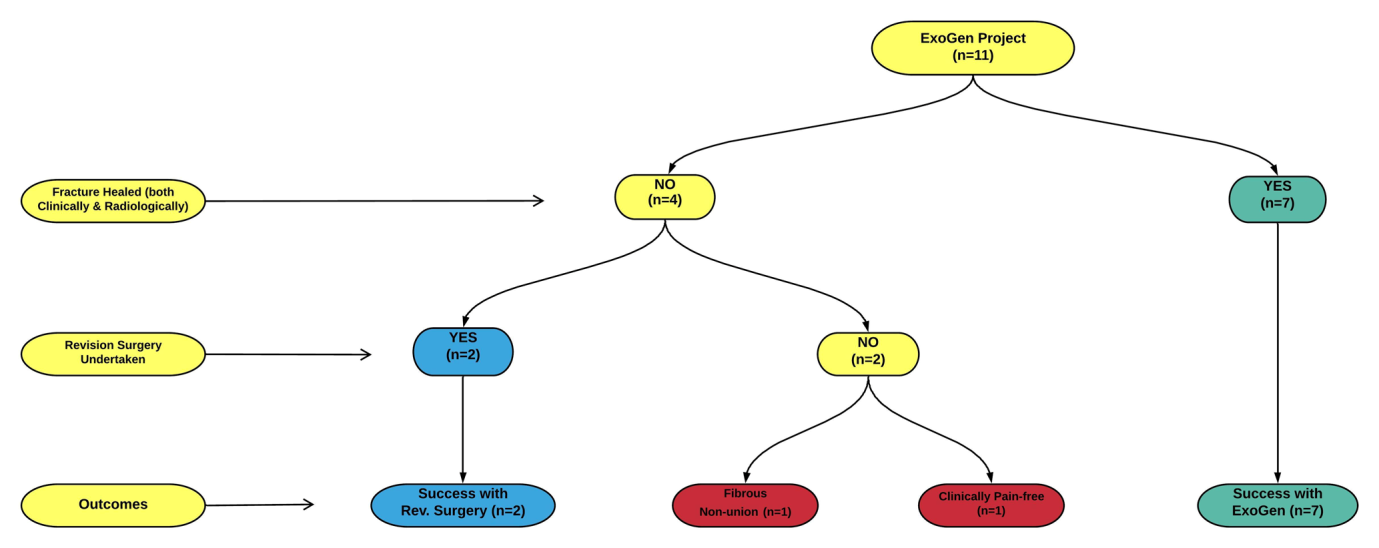
This pilot study included four male and seven female patients whose mean age was 54.9years (range: 26–71y). The mean duration of follow-up was 18.5months range; 10.0- 24.5m). The bones were ExoGen was applied were; Humerus (3); Radius (1); Femur (1); Tibia + Fibula diaphysis (1) and Pilon fractures (5). The mean duration from sustaining the fracture to application of ExoGen treatment was 4.1months (range; 1.0-9.0m). Standard ExoGen with 250 session delivery of acoustic radiation was used in eight whilst extended ExoGen for 325 - 375 sessions was used in three patients. The compliance rate was ≥90% in all patients and there were no complications/adverse events observed in any of them. LIPUS was used as an adjunct with surgery in one patient with Pilon fracture. ExoGen was successful in eliminating the need for any operative intervention in seven patients thus yielding a healing rate (HR) of 63.6%. The treatment course of all patients and their final outcomes is illustrated in the form of a flowchart in Figure 2. Two patients needed revision surgery to aid with fracture osteosynthesis that included diaphyseal fractures of: i) Humerus (needing re-fixation) and ii) Tibia + Fibula (needing implant removal and re-fixation). An illustrative example of ExoGen application for a forearm fracture is shown in Figure 3.

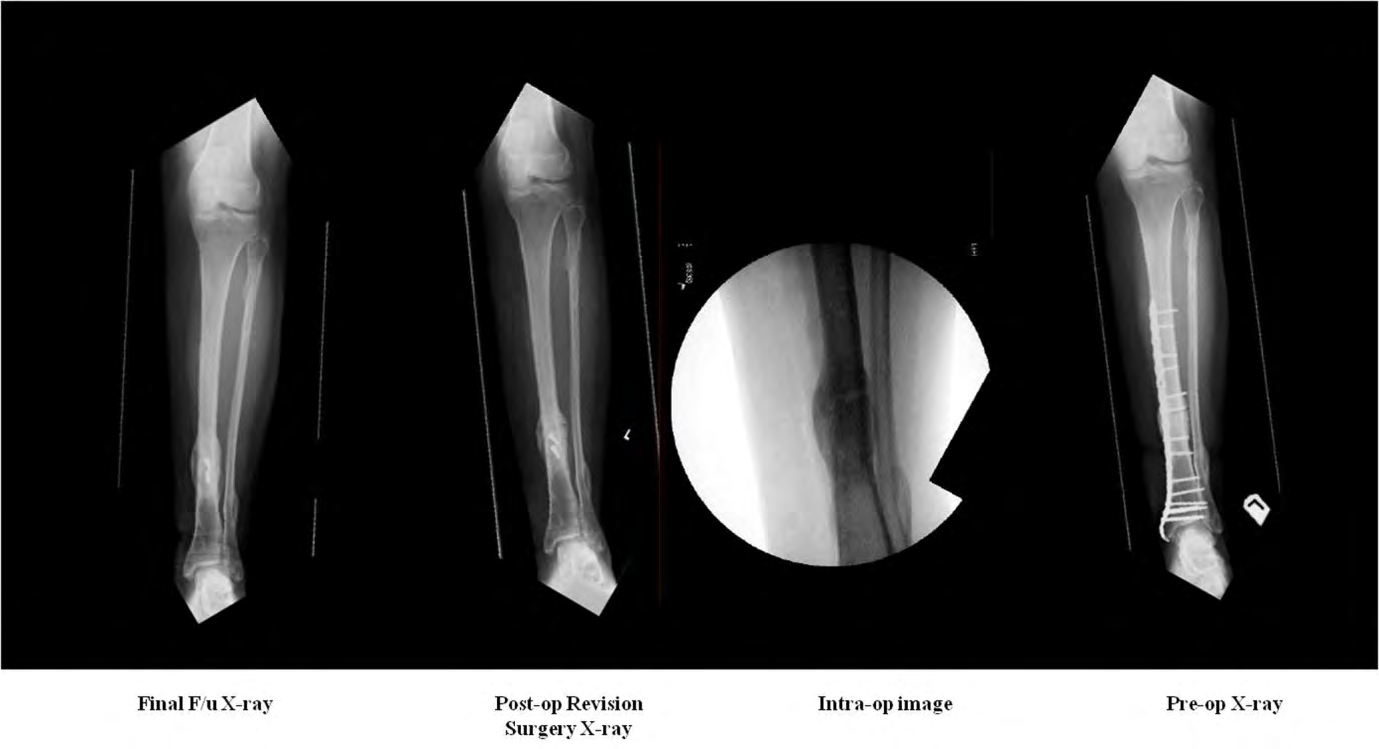
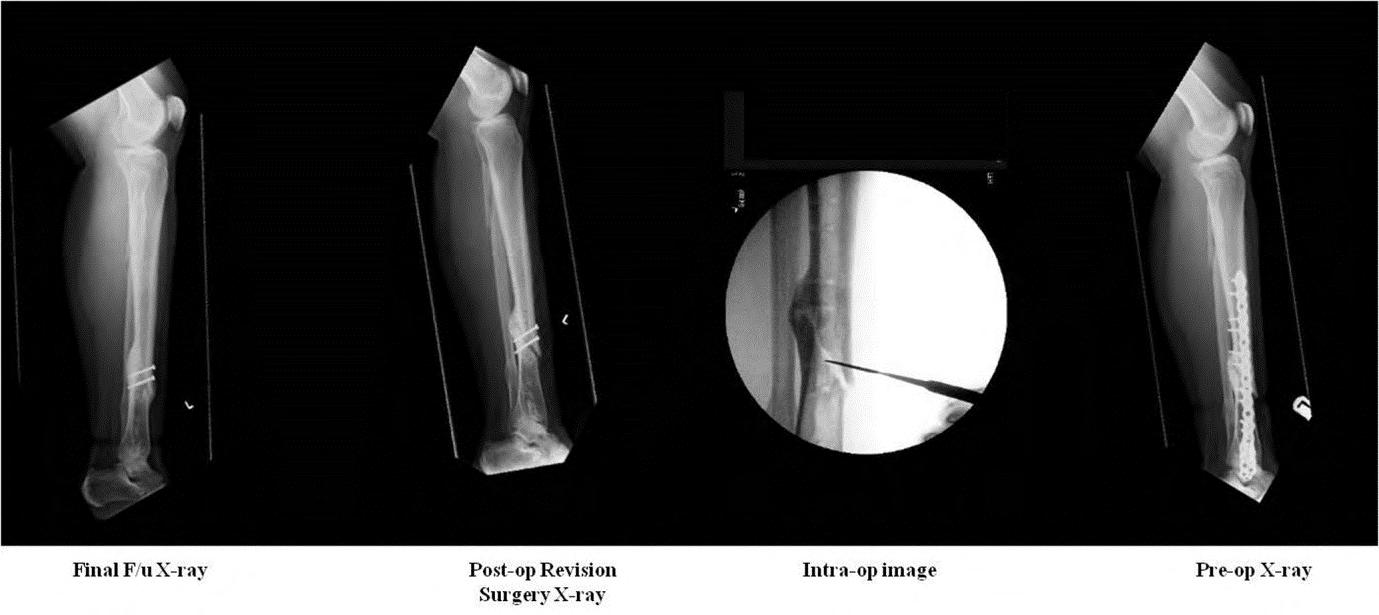
An index case of humeral diaphyseal fracture that was successfully treated by ExoGen application at 6months for delayed union with excellent union/re-modelling at final follow-up of 18months in a 71y/F having no co-morbidities is illustrated in Figure 4. An index case of ExoGen failure for a hypertrophic non-union of Tibial diaphyseal fracture that was initially treated by a locking plate fixation in a 46/F who was a smoker and had Vitamin D insufficiency is illustrated in Figure 5. This individual eventually needed a revision surgery and underwent implant removal, debridement of fracture site and two lag screws fixation. Fracture healing was achieved at one year post-revision surgery. Key radiographs of this patient are illustrated in Figure 6 respectively.


| No | Age | Sex | Diagnosis | Mechanism | Co-morbidities | Smoking | Date of Injury | Treatment | Date of Surgery | ExoGen Module | CT Done | Comments | Result |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 71 | F | Left Proximal 1/3rd humeral diaphyseal #re. | Simple fall (Low Velocity) | RA (on MTX), DVT, Osteoporosis, B/L TKR, Rt. THR. | No | 17-07-2017 | Non- operative management in brace for 6mo | n/a | 250 | No | Failed - Fibrous Union accepted in Mar 2019 & Discharged. | Failed |
| 2 | 47 | M | Right Middle 1/3rd humeral diaphyseal #re | RTA @ 50mph (High Velocity) | Ex-smoker (6y ago) | 25-02-2018 | ORIF followed by Revision Surgery | 20/03/2018 & 13/11/2019 | 250 | Yes 08/03/2020 | Hypertrophic non- union and Re-plated in Nov 2019 and #re healed by Sept 2020 | Failed | |
| 3 | 71 | F | Left Middle 1/3rd humeral diaphyseal #re | Tripped over dog (Low Velocity) | No | 22-09-2018 | Non- operative | n/a | 250 | No | Excellent healing with Re-modelling. | Healed | |
| 4 | 26 | M | Right Mid- shaft Radius fracture. | Vigorous Rugby tackle (High velocity) | No | 19-07-2018 | ORIF | 22-07-2018 | 250 | No | Asymptomatic with excellent outcome. | Healed | |
| 5 | 61 | F | Distal third Left Femoral spiral diaphyseal #re | Tripped over doorstep (Low velocity) | Mild COPD, Osteopenia | Ex-smoker (7y ago) | 25-09-2018 | ORIF | 27/09/2018 (Locking Plate). | 250 | Yes 15/08/2020 | Non-union on CT and planned to do Exchange Nailing. Fracture united in Sept. 2020 while waiting for surgery. | Healed |
| 6 | 48 | F | Right Tibia Comminuted distal-third #re | Leg injury: Wheelchair hit wall (Low velocity) | Congenital kyphoscoliosis, Spina bifida and hydrocephalus (shunt), Vit-D insufficiency. | No | 22-11-2017 | Non- operative n Cast and moonboot | n/a | 250 | No | Healed (clinical and x-ray assessment). Has minimal ambulation (transfer from chair to bed). | Healed |
| 7 | 46 | F | Comminuted Left distal 1/3 Tibia + Fibula fracture. | Simple fall while dancing (Low Velocity) | Alcohol abuse, Smoking, Vit-D insufficiency and mild Asthma | Yes (10-20/ day) | 25-02-2018 | ORIF | 26/02/2018 & 17/09/2019. | Extended Use (>325) | Yes 27/08/2020 | Hypertrophic non- union and Implant removal + 2 Lag screws done. #re healed now. | Failed |
| 8 | 66 | F | Left Ankle Pilon fracture. | Simple fall indoors (Low Velocity). | MS + Spastic paraparesis, B/L Nephrectomy for Chronic Pyelonephritis (on Dialysis). | No | 25-11-2017 | MUA & Non- operative treatment. | 2/12/2017 | 250 | No | Also sustained Right Bi-malleolar ankle fracture (Rxed in BK Pop cast and healed in June 2018). | Healed |
| 9 | 47 | M | Right Ankle Pilon fracture. | Simple fall from stepladder (Low Velocity) | Mild Asthma | No | 24-05-2018 | 24/5/2018 & 4/6/2018 | Ex-Fix followed by Screw fixn & ICBG. | 250 | No | Developed PE (CTPA proven @ 16th Post- op day). Early use of ExoGen at 1mo post- op as an Adjunct to Surgery | Healed |
| 10 | 63 | M | Left Ankle Pilon fracture with skin blisters. | Simple fall from stepladder (Low Velocity) | Chronic back pain with previous spinal fusion. | No | 12/12/2018 | 14/12/2018 (Removed at 8mo) | Ex-Fix application & ORIF Abandoned. | Extended Use (>375). | No | Satisfactory healing at one year and discharged | Healed |
| 11 | 58 | F | Right Ankle Pilon fracture. | Simple fall from stepladder (Low Velocity) | Mild COPD, Asthma & Vit-D insufficiency. | Yes (5-10/ day) | 19-09-2018 | 20/09/2018 & 01/10/2018. | Ex-Fix followed by ORIF (antero- lateral plating). | Extended Use (>340). | No | Non-union on plain x-rays & Ankle drifting into Valgus. Patient pain-free & Ankle arthrodesis proposed | Non- union on X-rays |
Table 2: Patient demographics and their salient characteristics during the treatment course.
Two patients had failure of fracture healing at the end of study. These included: 1) 71/F with humeral diaphyseal fracture suffering from Rheumatoid Arthritis who had fibrous non-union and was relatively pain-free. Given her functional needs and guided by her symptoms, this was accepted and she had learnt/coped to live with it; 2) 58/F with Pilon fracture managed surgically by Plating. Despite extended use of ExoGen for >340 sessions, there was non- union with ankle valgus mal-alignment. A salvage operation in the form of ankle arthrodesis was recommended at the end of the study. There were no atrophic or infective non- unions in our series though one patient with a Pilon fracture had superficial infection that was managed by antibiotics and regular dressing changes. ExoGen was used as an ‘Adjunct’ to surgery in one patient (at one month) who was re-admitted on 16th post-operative day with pulmonary embolism that was proven by Computed tomography pulmonary angiography (CTPA). ExoGen was used as an ‘Alternative’ in all other patients in this case series. A summary of patient demographics with their morbidity profile and salient information is represented in Table 2. Being a pilot project with small sample and purely an observational study, no statistical analysis was possible/required.
Discussion
We undertook a pilot study approved by CG committee in a publicly funded healthcare delivery system at a DGH to report the healing rate with use of LIPUS in appendicular skeletal fractures sustained in adult population over two calendar years (i.e. 2017 and 2018). A commercially available ExoGen device that delivered acoustic radiation over the fracture site at recommended settings. A window was cut out in patients who wore casts to apply the transducer at the site of maximum tenderness to deliver ultrasound pressure waves. The mechanism by which ultrasound causes bone healing is fascinating and subject to extensive basic science research over the past few decades [12, 14, 15, 16]. High intensity focused ultrasound (at ≥300 mW/cm2) has a role in cancer therapy and was observed to cause thermal damage, mucosal burns and growth plate destruction [17]. Hence we recruited only skeletally mature patients (i.e. ≥25years) for our pilot study. The ExoGen administers LIPUS at ≤30 mW/cm2 SATA intensity with a power of 117mW via an un-focused ultrasound transducer having an active area of 3.88 cm2 applied over the fracture site/area of maximal tenderness. It has an attractive safety profile with no reported adverse events/complications in published literature.
The mechanism of action by which LIPUS facilitates fracture healing/bony union as reported by basic science research studies are: • Increased expression of bone morphogenetic protein (BMP) 2, 4 and 6 with activation of osteoblasts.
- Up-regulation of Cyclo-oxygenase2 (COX2) enzyme that facilitated Prostaglandins synthesis.
- The micro-mechanical stresses delivered by ultrasound pressure waves causes nano motion at the fracture site that stimulated bone healing by improving the mechanical properties of the Callus.
- The heat generated in tissues (<10oC) that absorbed the ultrasound energy caused enzymatic changes that dissolved collagen.
- Activation of canonical Wnt signalling pathway influenced the osteoblastic MG-63 cells to lay bone.
- Up-regulation of Vascualar endothelial growth factor (VEGF) and inhibition of RANK Ligand mediated Osteoclast resorption.
- By down regulating Osteoprotegerin (OPG) as high serum levels of OPG were found in atrophic non-union fractures.
In-summary by LIPUS, the mechanical signals are converted into biochemical response that produces bioactive molecules promoting fracture healing. The deepest bone that can be influenced by application of LIPUS is Femur (average of 11.8cms from skin surface). The therapeutic efficacy of LIPUS at ≥12cms is not known / reported to the best of our knowledge.
The first ever clinical use of LIPUS for osteosynthesis was reported by Xavier and Duarte in 1983 [5, 18]. They treated 28 patients and reported success with a HR of 70% (20/28). Heckmann, et al. published first ever Randomized controlled trial (i.e. RCT a Level of Evidence [LoE] I study) reporting outcomes with its use in treating Tibial diaphyseal closed and Grade I open fractures that paved the way for US- FDA approval in 1994 [19]. 67 patients were randomized to receive Placebo vs. LIPUS (comprising of 34 vs. 33 individuals respectively) and there was a statistically significant difference in time to healing (114 ± 10.4 vs. 86 ± 5.8 days) with p=0.0001. There were no complications or adverse events thus making a foray of this novel technology in clinical use. In a pilot study of 14 patients, Hemery, et al. reported a HR of 79% (11/14 fracture consolidation) [20]. Co-existent infection or type of non-union (i.e. Atrophic vs. Hypertrophic) did not influence the outcomes. Roussignol, et al. treated 59 patients with ExoGen as a part of pilot project over five years (2004-08) [21]. They observed a 6month consolidation/ fracture HR of 88% (52/59 healed successfully). Patient characteristics like age, smoking status, and site of fracture or gender did not influence the outcomes.
More recently within past couple of years, two studies have been published from the United Kingdom reporting the HR and outcomes with use of ExoGen for Foot and Ankle surgeries [22, 23]. Mirza, et al. had a success in 12/18 patients with a HR of 67% and their healing rate was similar to ours at 63.3% [22]. Majeed, et al. had a cohort of 47 patients who were divided into three groups: i) Fractures; ii) Elective procedures – iia) Hindfoot procedures and iib) Forefoot and mid-foot procedures [23]. They reported a HR of 78.7% (37/47 patients healed). Only one hypertrophic non-union vs. nine atrophic non-unions fractures had failed to unite. Their series had 10 patients with Tibia + Fibula, Pilon and Ankle fractures and the HR in these sub-groups of patients was not reported. Leighton, et al. undertook a systematic review with Meta-analysis from a set of 13 published studies that reported outcomes in 1,441 DU and NU managed by LIPUS which remains to this day one of the most comprehensive meta-analysis published in English language [24]. The overall HR for un-infected non-unions was 80% and was comparable that union rates achieved by surgical intervention. The observed HR for long bones was best for Tibia + Fibula at 86%. The HR for other long bones were: i) Humerus (74.05); Radius + Ulna ((77.5%) and Femur (80.4%). LIPUS was particularly effective in elderly/ frail patients with several co-morbidities who were high-risk surgical candidates. LIPUS worked especially worked very well in i) Hypertrophic non-unions and ii) Time from surgery to ExoGen application interval of <6months. The sub-group that benefited the most from LIPUS was in Delayed union cases that had ExoGen application between 3-6months of fracture. Few studies have reported the role of LIPUS as an adjunct along with surgery. Interpretation of its efficacy in such scenarios is difficult owing to the bias with operative intervention.
Cost-effectiveness and economic modelling studies are increasingly emphasized in Orthopaedics esp. over the past decade. LIPUS has emerged as a clear winner in this domain and was at least 60% more cost-effective and eliminated of all complications associated with operative intervention. Several studies have reported savings with LIPUS in both North America and Europe. Key studies summarizing the cost gains made by using LIPUS is illustrated in Table 3 [21, 23, 25].
| No | Author | Country | LIPUS | Surgery | Comments |
|---|---|---|---|---|---|
| 1 | Rossigul, et al. [21] | France | € 1,772 | ≥€4,480 | Potential savings of €2,000 – €6,800 per patient. LIPUS was at least 60% cost-effective. |
| 2 | Majeed, et al. [23] | U.K | £2,300 | £3,611 to £6,370 | Potential savings of £1,300 – 3,000 per patient. LIPUS was at least 50% cost-effective. |
| 3 | Heckmann, et al. [25] | USA | $2,590 | $20,575 | Potential savings of at least $13,000 - 15,000 per Tibial fracture resulting in projected savings of $14.6m per 1,000 patients. |
Table 3: Summary of Cost-analysis studies with ExoGen and potential savings made with its use.
Finally our study is not without limitations. Being a small sample size involving only 12 recruited patients with one lost for follow-up (n=11), no meaningful statistics could be undertaken. Suffices to say that our HR of 63.6% is encouraging and comparable to published studies observed by other independent researchers. We did not collect any outcome measures and relied on patient reported visual analog scale (VAS) pain score along with clinical assessment of tenderness, abnormal bony crepitus and plain radiographs to assess union. Given a busy fracture clinic setting and skeletal workforce, our department doesn’t have a Research co-ordinator/assistant to collect such research related patient related outcome measures. CT scans were not done to confirm union in our seven patients as it would have warranted a separate Research ethics committee (REC) approval given the risks of irradiation. REC would have never approved for CT scans as the plain radiographs were reported by Consultant Radiologists to have achieved satisfactory fracture union/consolidation. However CT scans were done in three patients to either confirm non-union or to aid in planning with revision surgery.
Conclusion
We report our experience with use of LIPUS in delayed and non-union of long bone closed fractures in a case series involving 11 adult patients with a mean follow-up of 18.5months as a part of a Pilot study. Our healing rate of 63.6% was comparable to the HR of published literature and there were no complications with its use. Revision surgery was avoided in at least three patients (diaphyseal fractures of i) Radius; ii) Femur and iii) Pilon fracture) resulting in an estimate cost savings of at least £10,000 (i.e. Ten thousand pounds sterling). The results are encouraging and this pilot study has given us an enormous insight into creating a robust prospective database with refined/stringent inclusion vs. exclusion criteria. These findings have justified continued use of ExoGen for un-infected DU and NU in our clinical practice.
References
-
Zura R, Xiong Z, Einhorn T, Watson JT, Robert FO, et al. (2016) Epidemiology of Fracture Nonunion in 18 Human Bones. JAMA Surg 151(11): e162775.
-
Hak DJ, Fitzpatrick D, Bishop JA, Marsh JL, Susanne T, et al. (2014) Delayed union and nonunions: Epidemiology, clinical issues, and financial aspects. Injury 45(2): S3-S7.
-
Mollon B, da Silva V, Busse JW, Einhorn TA, Mohit B (2008) Electrical Stimulation for Long-Bone Fracture- Healing: A Meta-Analysis of Randomized Controlled Trials. J Bone Joint Sirg Am 90(11): 2322-2330.
-
Chang WD, Wu JH, Wang HJ, Jiang JA (2014) Therapeutic Outcomes of Low-Level Laser Therapy for Closed Bone Fracture in the Human Wrist and Hand. Photomed Laser Surg 32(4): 212-218.
-
Xavier CAM (1983) Stimulation of bone callus by ultrasound, clinical application. Rev Brasileira Ortop 18: 73-80.
-
Goel A, Sangwan SS, Siwach RC, Ali AM (2005) Percutaneous bone marrow grafting for the treatment of tibial non-union. Injury 36(1): 203-206.
-
Lissenberg TSN, de Gorter DJJ, Sier CFM, Schipper IB (2011) Use and efficacy of bone morphogenetic proteins in fracture healing. Int Orthop 35(9): 1271-1280.
-
Hernigou P, Desroches A, Queinnec S, Flouzat LCH, Alexandre P, et al. (2014) Morbidity of graft harvesting versus bone marrow aspiration in cell regenerative therapy. Int Orthop 38(9): 1855-1860.
-
James AW, LaChaud G, Shen J, Asatrian G, et al. (2016) A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng Part B Rev 22(4): 284-297.
-
Nguyen V, Meyers CA, Yan N, Agarwal S, Levi B, et al. (2017) BMP-2-induced bone formation and neural inflammation. J Orthop 14(2): 252-256.
-
Bayat M, Virdi A, Jalalifirouzkouhi R, Rezaei F (2018) Comparison of effects of LLLT and LIPUS on fracture healing in animal models & patients: Systematic review. Prog Biophys Mol Biol 132: 3-22.
-
Zura R, Mehta S, Rocca GJD, Jones J, Grant SR (2015) A cohort study of 4,190 patients treated with low-intensity pulsed ultrasound (LIPUS): findings in the elderly versus all patients. BMC Musculoskelet Disord 16: 45.
-
NICE (2018) Low-intensity plused ultrasound to promote healing of fresh fractures at high risk of non- healing: Interventinoal procedure guidance (IPG 622).
-
Olkku A, Leskinen JJ, Lammi MJ, Hynynen K, Anitta M (2010) Ultrasound-induced activation of Wnt signaling in human MG-63 osteoblastic cells. Bone 47(2): 320-330.
-
Pounder NM, Harrison AJ (2008) Low intensity pulsed ultrasound for fracture healing: A review of the clinical evidence and the associated biological mechanism of action. Ultrasonics 48(4) 330-338.
-
Harrison A, Lin S, Pounder N, Mikuni TY (2016) Mode & mechanism of low intensity pulsed ultrasound (LIPUS) in fracture repair. Ultrasonics 70: 45-52.
-
Haar ter G (2001) High Intensity Ultrasound. Seminars in Laparoscopic Surgery 8(1): 77-89.
-
Duarte LR (1983) The stimulation of bone growth by ultrasound. Arch Orthop Trauma Surg 101(3): 153-159.
-
Heckman JD, Ryaby JP, McCabe J, Frey JJ, Kilcoyne RF (1994) Acceleration of tibial fracture-healing by non- invasive, low-intensity pulsed ultrasound. J Bone Joint Surg Am 76(1): 26-34.
-
Hemery X, Ohl X, Saddiki R, Barresi L, Dehoux E (2011) Low-intensity pulsed ultrasound for non-union treatment: a 14-case series evaluation. Orthop Traumatol Surg Res 97(1): 51-57.
-
Roussignol X, Currey C, Duparc F, Dujardin F (2012) Indications and results for the Exogen ultrasound system in the management of non-union: a 59-case pilot study. Orthop Traumatol Surg Res 98(2): 206-213.
-
Mirza YH, Teoh KH, Golding D, Wong JF, Yogesh N (2019) Is there a role for low intensity pulsed ultrasound (LIPUS) in delayed or nonunion following arthrodesis in foot and ankle surgery?. Foot Ankle Surg 25(6): 842-848.
-
Majeed H, Karim T, Davenport J, Karski M, Robert S, et al (2020) Clinical and patient-reported outcomes following Low Intensity Pulsed Ultrasound (LIPUS, Exogen) for established post-traumatic and post-surgical nonunion in the foot and ankle. Foot Ankle Surg 26(4): 405-411.
-
Leighton R, Watson JT, Giannoudis P, Papakostidis C, Harrison A, et al. (2017) Healing of fracture nonunions treated with low-intensity pulsed ultrasound (LIPUS): A systematic review and meta-analysis. Injury 48(7): 1339-1347.
-
Heckman JD, Sarasohn KJ (1997) The economics of treating tibia fractures. The cost of delayed unions. Bulletin Hosp Jt Dis 56(1): 63-72.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results