Comparative MRI and Laboratory Evidence of Muscle Injury after Intramuscular Injection of Diclofenac 1 mL and 3 mL: Case Study Reports
Aim & Objectives: Intramuscular (IM) injections of 1 mL and 3 mL Diclofenac 75 mg are used in the clinic in the management of the pain. The present study was performed with the aim to evaluate muscle injury after IM injection of Diclofenac 75 mg/1 mL (Dynapar AQ®, Troikaa Pharmaceuticals Limited, India) and Diclofenac injection 75 mg/3 mL (commercially available) in subjects using Magnetic Resonance Imaging (MRI) and laboratory blood tests. Material & Methods: Two separate single arm case studies, (each comprising of a single healthy subject) were carried out after Ethics Committee approvals and CTRI Registration. Two subjects who gave written informed consent received either Diclofenac injection 75 mg/1 mL (Dynapar AQ®, Troikaa Pharmaceuticals Limited, India) OR Diclofenac injection 75 mg/3 mL (commercially available) and the muscle injury was evaluated at different time points up to 14 days. Results: In both the subjects, the intramuscular injury after the injection was reliably documented by MRI and laboratory tests. For the subject who received Diclofenac injection 75 mg/3 mL, there was significant muscle injury observed (T2- weighted magnetic resonance was increased manifold: the volume of muscle injury was 108 mL at 24 hr after injection; 137 mL at 48 hours, and progressive worsening after 48 hours, rising to 271 mL on Day 7 with subsequent normalization at Day 119). However, in the subject who received Diclofenac injection 75 mg/1 mL, muscle injury was relatively minor and reversed quickly at day 7; (T2-weighted magnetic resonance volume of muscle injury was 66 mL at 24 hr after injection, a flatter peak of 69 mL at 48 hours, declining thereafter). In the subject who received 3 mL injection, the CPK levels (Normal range: serum CPK: 39 – 308 U/L by immune assay) were highly increased (from baseline of 47 U/L to 1975 U/L in 8 hours, 1320 U/L at 48 hours, continued elevation after 48 hours: 420 U/L at 7 Days and 267 U/L on Day 119), with prolonged plateau of elevation and gradual decline over weeks indicating significant muscle injury with Diclofenac injection 75 mg/3 mL whereas, in the subjects who received diclofenac injection 75 mg/ 1 mL, there was only minor increase in CPK (from baseline of 93 U/L to 433 U/L in 24 hours) and was normalized to 95 U/L at day 7. In the subject who received Diclofenac injection 75 mg/3 mL, the IL-6 was within the upper range of normal (Normal Range: IL6 0-50 pg/mL by ELISA), and rose from a baseline of < 2 pg/mL to 37.3 pg/mL, but in the subject who received 1 mL IM Diclofenac, values stayed low throughout (<4 pg/mL). Conclusion: There was higher muscle injury following 3 mL Diclofenac intramuscular injection when compared to 1 mL Diclofenac intramuscular injection. This is the first comparative report confirming radiologic and laboratory evidence of muscle injury produced by a 1 mL and 3 mL Diclofenac injection, and opens the door for further research on muscle injury, and focuses our efforts to prevent or minimize the same.
Introduction
Injection Diclofenac sodium is effective and well tolerated in the management of pain [1]. The relief of acute pain by administration of intramuscular injections of Diclofenac is a safe and well-tolerated treatment option. It is marketed worldwide in 3 mL, 2 mL and now 1 mL injectable formulations. Adverse local reactions for diclofenac injections are reported in the medical literature [2]. Muscle injury after intramuscular injection may often be unrecognized, and the issue may be more severe than assumed. In a recent experimental study by Probst, et al. rats were intramuscularly injected Diclofenac [3]. They observed that all the animals responded with local inflammatory intolerance. Long-lasting fluid accumulation, necrotic changes and infiltration of neutrophil granulocytes in the muscle were confirmed by MRI and histopathological evaluation. The severity of inflammation was dependent on dose and the pharmaceutical formulation of the drug. In another study by Probst, et al. the intramuscular injection of Diclofenac 75 mg/2 mL unexpectedly damaged approximately 60 mL of gluteal muscle of the patient. The patient was asymptomatic, and the muscle damage was confirmed by enhancement of the T2-weighted MRI signal by manifolds in that area. Elevation of the plasma CPK activity for longer than 48 hr was also observed [4]. Local complications may commonly occur because of bacterial contamination, wrong injection technique, and wrong injection site [5], injection volume [6], type and amount of solvent used and viscosity [7]. The 3 mL formulations are recommended for deep intramuscular, generally intragluteal administration. However, the standard needles may not reach the gluteus maximus muscle in many cases, especially in obese patients [8, 9]. Other injection sites like the deltoid have been suggested and could be more suitable for these patients. Owing to the small area of the deltoid, the volume of injections that can be given at this site is commonly 1 mL or less [10, 11]. The formulation of Diclofenac injection was recently developed to provide 75 mg of Diclofenac in 1 mL that could also be administered at alternative sites including intra-deltoid.
Various BA/BE and CT studies have been reported in the literature for safety and efficacy of intramuscular injection of Diclofenac. As per literature the volume of injection is a known factor to induce muscle injury, [12] however very limited data are available to evaluate the muscle injury using MRI method after the IM Diclofenac injection. To confirm that intramuscular injection of Diclofenac 75 mg/3 mL leads to more muscle injury compared to Diclofenac injection 75 mg/1 mL in humans, we provide the clinical case report of two subjects who gave written consent to take extra blood specimens for laboratory evaluation, as well as for MRI after receiving intramuscular Diclofenac injection. This study is focused on evaluation of comparison of muscular injury and other biochemical parameters after the administration of Diclofenac injection 75 mg/3 mL and 75 mg/1 mL.
Study Design
The research comprised of a pair of prospective, open label, single arm, and single center exploratory studies. Two consenting healthy subjects were administered commercially available Diclofenac 75 mg/3 mL or Diclofenac 75 mg/1 mL (Dynapar AQ®, Troikaa Pharmaceuticals Limited) into the upper outer quadrant of the gluteus muscle. (Adhering to the safe IM injection technique – Z-track method).
Methodology
After Ethics Committee Approval (ECR/30/lnst/ GJ/2013/RR-16 and ECR/30/lnst/GJ/2013/RR-19) and Clinical Trial Registry (CTRI/2020/01/023010 and CTRI/2020/03/024099), two male subjects (one aged 36 years, bodyweight 57 kg, body height 170 cm; and the second, aged 27 years, body weight 58.5 kg, body height 178 cm) received an intragluteal injection of Diclofenac 75 mg/1 mL (Dynapar AQ®, Troikaa Pharmaceuticals Limited, India) or commercially available Diclofenac Sodium 75 mg/3mL. They participated in clinical–chemical evaluations, safety evaluations and MR imaging of the Right gluteal region (Gluteal Maximus), aimed at evaluating a potential muscle injury at the injection site. MRI in the supine position was performed using a 1.5–Tesla Esanza (Siemens) within the Radiology Department of the same Hospital by the same team of Radiology Staff. Time Points were 2, 12, 22, 32, 47, 62, 92, 122, 182, 242 min, as well as 7.5 h and 1, 2, 7 and 14 days after intramuscular administration. Blood was withdrawn from the forearm vein before and 1, 4, 8, 24 and 48 hours, Day 7 and Day 14 after administration to measure creatine kinase (CPK, by immune assay), C-reactive protein (CRP, by immunoturbidimetric assay), Procalcitonin (PCT, by electrochemiluminescence) and interleukin-6 (IL-6, by ELISA). [Normal ranges were as follows: serum CPK: 39 – 308 U/L; CRP: 0 – 5 mg/L; Procalcitonin PCT-Q: <0.5 ng/mL (low risk of severe sepsis and/ or septic shock); IL6 0-50: pg/ mL] These were tested in the Department of Biochemistry and Immunology of the same Hospital by the same team of staff.
Result
In both the subjects, the intramuscular injury after the injection was reliably documented by MRI and laboratory tests. 3D sequence of right gluteal region was taken before and after administration of injection Diclofenac sodium 75 mg/1 mL and 75 mg/3 mL. The sequential scans were taken at prescribed time format and approximate volumes of altered signal intensity at the site of injection were measured as described in Table 1. The MRI (T2-weighted magnetic resonance signal) measurement of volume of damaged muscle demonstrated that in case of Diclofenac injection 75 mg/1 mL (Dynapar AQ®) the muscle injury was relatively modest, (69 mL) by Day 2, followed by rapid recovery. However, after administration of Diclofenac injection 75 mg/3 mL, there was a rapid rise in muscle damage, maximizing to 271 mL at day 7 (Table 2, Figure 1).
| Time points* | Volume of muscle injury (cm3) | CPK (U/L) | CRP (mg/L) | PCT (ng/mL) | IL6 (pg/mL) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 mL | 3 mL | 1 mL | 3 mL | 1 mL | 3 mL | 1 mL | 3 mL | 1 mL | 3 mL | |
| Pre dose | 0 | 0 | 93 | 47 | 0.8 | 1 | 0.04 | 0.15 | 1.5 | 2 |
| 1 hr | 20 | 45 | 144 | 374 | 0.62 | 1 | 0.04 | 0.02 | 1.5 | 14 |
| 4 hr | 41 | 79 | 347 | 1441 | 0.66 | 1 | 0.04 | 0.02 | 1.5 | 19.8 |
| 8 hr | 56 | 100 | 431 | 1975 | 0.65 | 1 | 0.04 | 0.02 | 2 | 25.7 |
| 1 day | 66 | 108 | 433 | 1830 | 0.62 | 1 | 0.04 | 0.02 | 1.5 | 26.1 |
| 2 days | 69 | 137 | 348 | 1320 | 0.62 | 1 | 0.03 | 0.02 | 1.5 | 5.6 |
| 7 days | 37 | 271 | 95 | 423 | 4 | 1 | 0.05 | 0.05 | 4 | 37.3 |
| 14 days | 19 | 0$ | 65 | 267$ | 0.6 | 1.00$ | 0.034 | 0.02$ | 2 | 1.5$ |
Table 1: Representative Image of MRI evaluation of muscle injury after Diclofenac injection 75 mg/ 1 mL and 75 mg/ 3 mL (Selected
Table 1: MRI and Laboratory parameters for muscle injury vs. time after Diclofenac injection 75 mg/1 mL and 75 mg/3 mL. $ Actual results were taken on day 119 due to COVID-19 pandemic lockdown. [Normal range: serum CPK: 39 – 308 U/L by immune assay; CRP: 0 – 5 mg/L by immunoturbidimetric assay; Procalcitonin PCT-Q: <0.5 ng/mL (low risk of severe sepsis and/ or septic shock) (by electrochemiluminescence); IL6: 0-50 pg/mL by ELISA] * MRI data for selected time points are mentioned for comparison.).
The Creatinine Phosphokinase (CPK) activity, a biomarker for the muscle tissue injury, was elevated 1 h after injection of the drug and reached its maximum after 8 hours in both the cases. In case of Diclofenac injection 75 mg/1 mL (Dynapar AQ®), Creatine kinase (CPK) activity was increased from 93 U/L to 433 U/L (normal range 39-308 U/L), i.e.
raised 4.6 fold at 8 and 24 hours whereas there was ~42 fold higher increase in case of Diclofenac injection 75 mg/3 mL, i.e. from 47 U/L to 1975 U/L (Table 1, Figure 1).The rise in CPK value remained elevated 9 fold after one week, and did not normalize to baseline levels even after 119 Days.
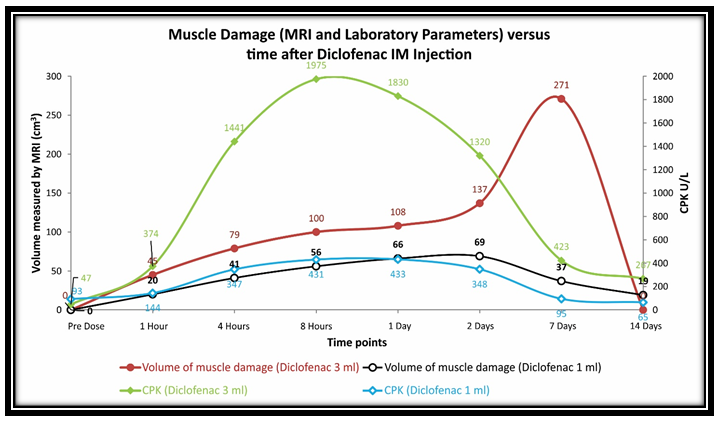
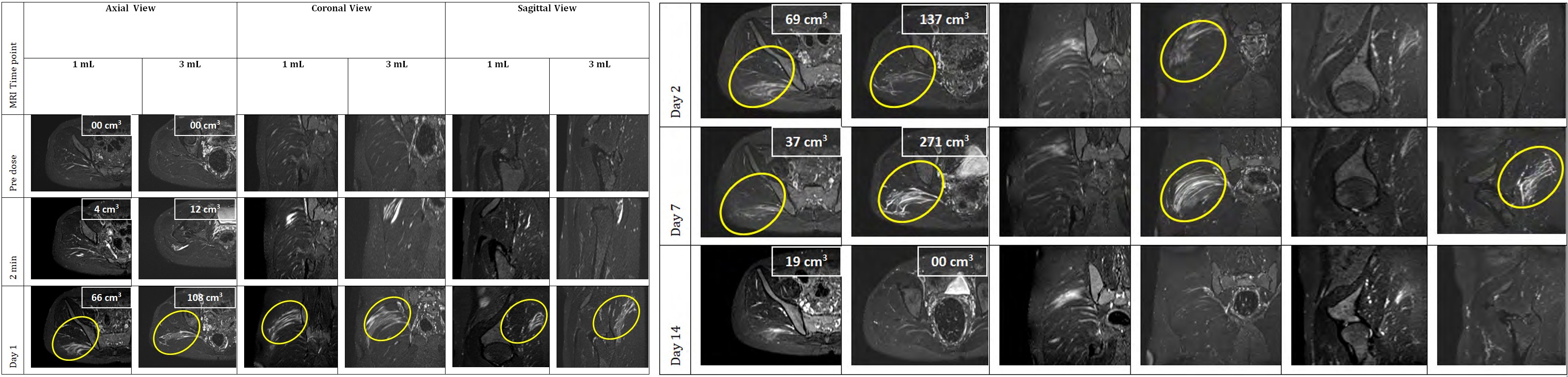
Table 2: Representative Image of MRI evaluation of muscle injury after Diclofenac injection 75 mg/ 1 mL and 75 mg/ 3 mL (Selected time points) Serum concentrations of CRP, PCT and IL6 remained within the normal range throughout the follow-up period both for Diclofenac injection 75 mg/1 mL and Diclofenac injection 75 mg/3 mL. For Diclofenac injection 75 mg/3 mL, although the IL-6 values stayed within the upper range of normal, they rose to 25.70 pg/mL at 8 hours, and 37.3 pg/ mL on day 7 from a baseline of <2 pg/mL, before reverting to baseline values on day 119 (Table 1).
Discussion
Complications with IM injection include muscle atrophy, injury to bone, cellulitis, sterile abscesses, pain, and nerve injury. In the published literature, quite a few reports of symptomatic muscle damage viz. pain on injection site has been reported with Diclofenac 75 mg/3mL intramuscular injection. In a review of 10,167 cases of 3mL Diclofenac intramuscular injection, 5.6% incidences were reported for pain at the injection site [13]. In another review of spontaneous and clinical trial reports for Diclofenac ampoules from the Novartis Global Safety Database published in the BMJ revealed 115 reports of injection site necrosis, 37 reports of injection site abscess, 11 reports of injection site reaction and 6 reports of necrotizing fasciitis [14]. Also case reports of muscle injury have been reported right from the early experience with the 3 mL injection [15, 16]. In literature for Diclofenac injection 75 mg/3 mL we found a study by Subnis, et al. where 196 patients received 1 mL diclofenac intramuscular injection, and there was no report of severe pain at the site of injection [17]. In another study by Shah, et al. in 250 patients there were no reports of moderate to severe pain at site of injection in Diclofenac 75 mg/1 mL arm [1]. In a similar study by Hardikar, et al. in 189 patients, intensity of pain at the site of injection was significantly lesser in patients treated with Diclofenac injection 75 mg/1 mL at 1 hour and 12 hours (p < 0.05) as compared to Diclofenac injection 75 mg/3 mL. This study reported good safety and tolerability of 75 mg/1 mL (Dynapar AQ®) [12]. We also asked M/s Troikaa Pharmaceuticals Limited [Marketing Authorization Holder of Dynapar AQ® (Diclofenac 75 mg/1 mL injection)] to provide us the local adverse reaction reports received in the Post-Marketing Surveillance/Periodic Safety Update Reviews (PSURs), and the company conveyed that more than 500 million doses of Dynapar AQ have been administered till now and no reports of severe pain or abscess or fasciitis at the site of injection have been reported.
Hence, there are reports of less pain and muscle injury caused by Diclofenac 1 mL injection as compared to the 3 mL Diclofenac injection. This is in line with our radiologic and laboratory finding study which reports lesser muscle damage with 1 mL diclofenac injection (Dynapar AQ®) as compared to 3 mL diclofenac injection. To the best of our knowledge this is the first report comparing radiologic and laboratory evidence of extent of muscle injury caused by a Diclofenac injection 75 mg/1 mL (Dynapar AQ®) and Diclofenac injection 75 mg/3 mL. The highest volume of muscle damage recorded by MRI after administration of Diclofenac injection 75 mg/1 mL and Diclofenac injection 75 mg/3 mL were 69 mL and 271 mL, respectively. In case of 1 mL diclofenac injection this damage was observed at day 2 followed by reduction over a week, whereas in case of 3 mL injection the muscle damage was increasing up to day 7 and reduced thereafter. Thus the progressively higher intramuscular injection volumes may be associated with a higher amount of muscle damage. In this research the CPK rise of 4.6 and ~42 fold was observed for 1mL and 3 mL diclofenac injection, respectively. In literature the CPK rise by 6 fold with 2 mL Diclofenac Injection has been reported Probst, et al. [4]. These CPK results were consistent with above MRI results indicating a direct relation between intramuscular injection volumes and the extent of muscle injury.
The duration of CPK rise is also consistent with above observations. In the subject who received Diclofenac injection 75 mg/1 mL (Dynapar AQ®), the CPK rise was modest, when compared to baseline values, and then declined to baseline values over one week. In the subject who received Diclofenac injection 75 mg/3 mL, the CPK remained elevated 9 fold after one week, and did not return to baseline levels even after 119 Days. Probst, et al. 2017 reported 6 fold elevation in Plasma creatine kinase activity within 8 h after 75 mg/2 mL diclofenac injection which returned to baseline levels after 1 week [4]. This indicates that the higher intramuscular injection volumes are associated with prolonged rise in CPK, and thus indicating a longer duration of muscle injury. The possible factors responsible for muscle damage are the amount of the injected volume, viscosity of the injected drug solution, the site of injection, and the technique of administration [7]. The lower muscle damage with Diclofenac injection 75 mg/1 mL (Dynapar AQ®) may also be attributed to judicious choice of solvent. The Diclofenac injection 75 mg/1 mL (Dynapar AQ®) has been formulated in such a way the viscosity of Diclofenac injection 75 mg/1 mL (Dynapar AQ®) is comparable to Diclofenac injection 75 mg/3 mL, even though concentration of Diclofenac in the 1 ml injection is 3 times than that in the 3 ml injection in about 1 ml injection solution [18]. In our study, more muscle injury by Diclofenac injection 75 mg/3 mL could also be attributed to differences in the formulations, higher amount of solvents present or to higher volume of injection. Usually the available 3 mL Diclofenac injection contains more amount of solvent than 1 mL injection. This way the 1 mL delivered the same amount of Diclofenac (75 mg) with lesser exposure to the solvents compared to the 3 mL injection.
Conclusion
It is commonly known that intramuscular administration of Diclofenac injection causes muscle injury, even though the injection technique is right. MRI technique along with lab parameter such as CPK was successfully used to evaluate the muscle damage caused by intramuscular dosing of 1 mL and 3 mL Diclofenac injection. Our results indicate that there was very high muscle injury following 3 mL Diclofenac intramuscular injection as compared to 1 mL Diclofenac intramuscular injection (Dynapar AQ®). This is the first comparative report confirming radiologic and laboratory evidence of muscle injury produced by a 1 mL and 3 mL Diclofenac injection. This data opens the door for further research on muscle injury caused by intramuscular injections, and enables us to focus our efforts to prevent or minimize the same.
Acknowledgements
The authors are thankful to the Nursing team, the MRI Team at Apollo Research Centre and to the volunteers for their participation in the study.
Compliance With Ethical Standards
Conflicts of Interest
All authors declare that they have no conflicts of interest. Clinical Trial Registry: CTRI/2020/01/023010 and CTRI/2020/03/024099 Ethics Committee Approval (ECR/30/lnst/GJ/2013/RR-16 and ECR/30/lnst/GJ/2013/RR-19) All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
References
-
Shah P, Subnis B, Varshney A, Pradhan C, Murthy TVSP, et al. (2011) Clinical efficacy of a novel new injectable diclofenac formulation designed for intradeltoid use in post-operative pain management. Int J Clin Pharmacol Ther 49(4): 286-290.
-
Chung C (2002) The use of Injectable Nonsteroidal Anti- Inflammatory Drugs in Local Accident & Emergency Practice. Hong Kong J Emerg Med 9(2): 65-71.
-
Probst M, Kühn JP, Scheuch E, Seidlitz A, Hadlich S, et al. (2016) Simultaneous magnetic resonance imaging and pharmacokinetic analysis of intramuscular depots. J Control Release 227: 1-12.
-
Probst M, Kühn JP, Modeß C, Scheuch E, Seidlitz A, et al. (2017) Muscle Injury After Intramuscular Administration of Diclofenac: A Case Report Supported by Magnetic Resonance Imaging. Drug Saf Case Rep 4(1): 1-7.
-
Hegan T (2002) Non steroidals, needles and negligence. Medical Protection Society casebook. Leeds: Medical Protection Society 12-13.
-
Svendsen O, Blom L (1984) Intramuscular injections and muscle damage: Effects of concentration, volume, injection speed and vehicle. Arch Toxicol Suppl 7: 472- 475.
-
Wermuth CG (2003) Chemical and Physicochemical Solutions to Formulation Problems. The Practice of Medicinal Chemistry: 2nd (Edn), Academic Press, USA, pp: 736.
-
Ojha A, Shep D, Nivsarkar M, Patel S, Jaiswal V, et al. (2009) Pharmacokinetic profile of a new formulation of injection diclofenac designed for intradeltoid use. Expert Opin Pharmacother 10(4): 517-522.
-
Shep D, Jaiswal V, Ojha A, Patel S, Nivsarkar M, et al. (2010) Pharmacokinetic profile of an intradeltoid diclofenac injection in obese Indian volunteers. J Pain Res 3: 235-240.
-
Preparing and Administering Intramuscular Injections | Protocol. https://www.jove.com/v/10261/preparing- and-administering-intramuscular-injections.
-
Hopkins U and Arias CY (2013) Large-Volume IM Injections: A Review of Best Practices. Oncology Nurse Advisor 4: 32-37.
-
Hardikar M, Bogra J, Gupta R, Maroo S, Patel K, et al. (2013) Diclofenac 75mg / 1ml intradeltoid injection for post-operative pain management in patients with BMI ≥ 25 kg / m2. Int J Res Med Sci 2: 115-120.
-
Pillans PI, Connor NO (1995) Tissue necrosis and necrotizing fasciitis after intramuscular administration of diclofenac. Ann Pharmacother 29(3): 264-266.
-
Sullivan O, Collins J (2002) Rapid Response: Intramuscular diclofenac: 25 year worldwide safety perspective is vital to consider. BMJ 325(7377): 1408.
-
Ali MT, Mathias IM (1991) Continued problems with diclofenac injections. Anaesthesia 46(12): 1089-1090.
-
Power I (1992) Muscle damage with diclofenac injections. Anaesthesia 47(5): 451.
-
Subnis BM (2010) Indian Medical Gazette - Evaluation of the Effectiveness and Safety of a New Formulation of Injection Diclofenac Dynapar AQ (75mg / ml ) in the Management of Post-operative Pain - A Pilot Study. Ind Med Gaz pp: 213-217.
-
Patel KR, Patel MR (2006) Injectable Preparations of Diclofenac and its Pharmaceutically Acceptable Salts. European Patent Specification.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results