Minimally Invasive Surgery for Anterior Pubic Rami Fractures Under Fluoro-Navigation Using the Medtronic O Arm System and Calcium Phosphate for Internal Fixation
Introduction: The incidence of anterior pubic rami fractures in elderly female patients over the age of 65 has been reported to be 64 %. Osteoporosis plays a role with these fractures, as they are caused by minimal low energy injuries from a fall. Indications for internal fixation of anterior pelvic ring are controversial because of the etiology being low energy trauma and the location being a non-weight bearing surface. In contrast to conventional open pelvic surgery, percutaneous screw fixation has gained popularity in the treatment of pelvic fractures, mainly because of minimal soft tissue damage, less operative blood loss, early surgical intervention, and comfortable mobilization of the patient. The use of calcium phosphate as a form of internal fixation further advances the advantages of minimally invasive surgery for internal fixation with less morbidity by the use of screw fixation. The incorporation of fluoro-navigation is a new surgical technique in orthopedic trauma surgery. (Figure 1) This study is to report our clinical results of fluoro-navigation surgery in anterior pelvic pubic rami fractures using calcium phosphate as the fixation of choice. This is the first report of this method of treatment using a new combination of visualization and internal fixation. Materials and Methods: From April 2018 to December 2019, 30 patients with anterior pubic rami fractures were treated with percutaneous cannulated calcium phosphate delivery under Medtronic O arm (fluoro-navigation) control. There were 5 male and 25 females, with a mean age of 84.6 years (range 80-104) for females and mean age of 90 years (84 – 99) for the 5 males. According to the AO and Orthopedic Trauma Association classification, all were considered lateral compression types of fractures. All patients were operated on when their general medical condition stabilized after emergency management and admission. The pain score on admission was reported as 10/10 in all cases. Plain standard pelvic x-rays were obtained on admission as well as CT scans of the pelvis. All the anterior pubic rami fractures were fixed using percutaneous delivery of calcium phosphate with the Zimmer trocar system by one senior surgeon. The Medtronics O arm fluoro-navigation was used in all cases. The surgeon was familiar with the navigation system and had much experience in the computer-assisted percutaneous placement of the trocars. Results: A total of 30 patients were treated with this new combination of surgical treatment of anterior pubic rami fractures. No screws were inserted or found to be necessary for fracture treatment. Each case used 2 trocars from the kits supplied from Zimmer. One end delivery trocar was directed to the inferior pubic ramus fracture and the second which was a side delivery trocar was used for the superior pubic ramus fracture. A total of 10 cc of calcium phosphate was used in each case, 5 cc per trocar. The position of the trocars were placed using the fluoro-navigation control of the O arm. Once the trocars were properly placed the calcium phosphate was delivered and viewed under flouro control and then again viewed with the spin sequence using the Medtronics O arm. Total patient time in the operating room was 56 minutes; Total surgery time was 26 minutes. Anesthesia in most cases was MAC or light sedation with local skin infiltration using 1% lidocaine. Blood loss during the operation was considered very minimal with derma bond used to cover the percutaneous sites as well as a small band-aid. No superficial or deep infections occurred. No patient sustained recognized neurologic, vascular, or urologic injury because of the percutaneous pubic rami fixation with calcium phosphate. Extravasation of the calcium phosphate from the fracture’s sites did not pose any sequelae with soft tissue injury or with fracture healing. All patients were encouraged to get out of bed and weight bear according to comfort on post-op day 1. All fractures united at the last follow-up. Conclusions: This study presented for the first time two new techniques for the operative treatment of pubic rami fractures of the pelvis. The delivery of calcium phosphate for fracture fixation of pubic rami fractures has been found to be safe, minimally invasive, providing pain relief and stability permitting early mobilization. The addition of intra-operative fluoronavigation technique makes the fracture treatment an accurate, and rapid method for the treatment of pubic rami fractures. Consistency of the operative procedure and teaching are mandatory for the success of this procedure. The learning curve for most orthopedists should be very short. The outcomes have been shown to benefit patient mobilization, decrease morbidity and decrease hospital stay.
Introduction
The pubic rami are important structures of the anterior pelvis with major muscle attachment sites for the lower extremities and the abdomen. Internal fixation of fractures of the pubic rami can stabilize the pelvic ring and enhance early mobility and weight bearing [1]. Pubic rami fractures represent 7% of all osteoporosis related fractures in people greater than 50 years of age in the United States. These fractures account for 5% of the total cost burden [2]. Pubic rami fractures occur in patients greater than 65 years of age after a low-energy fall. These fractures are common in elderly females [3, 4] (Figure 1).
One study by Kannus, found many pelvic fractures have an osteoporotic origin and their study noted that 64% of all pelvic fractures are osteoporotic. Their study found that in patients over the age of 60 the percentage of osteoporosis as a cause of these fractures increased to 94% [5].
A study, by the Mayo Clinic, by Melton reported on the incidence of pelvic fractures over a 10-year period (1968- 1977)[6]. Their study found that for men aged 55-74, the incidence of low energy pelvic fractures was 7/100,000 person years. The rate increased to 63.9/100,000 in men of 75 years and older. The rate increased to 220.3/100,000 person years when older than 85.
Indications for internal fixation of pubic rami fractures are controversial. Non-operative treatment including bed rest and mobilization according to comfort has been the standard of management [7]. Percutaneous screw fixation is gaining popularity in the treatment of pelvic and acetabular fractures mainly because of minimal soft tissue damage, less operative blood loss, early surgical intervention and comfortable mobilization of the patient [8, 9, 10]. A previously published report demonstrated the successful use of calcium phosphate as the internal fixation product of choice [11]. C-arm fluoroscopy was used during surgery, as reported with percutaneous screws, achieving good accuracy and avoiding neural or vascular injury.
This technique requires a working knowledge of pelvic anatomy by an experienced surgeon. Fluoroscopy provides one image at a time allowing the confirmation of trocar, guide wire or screw placement. There is extension of surgical time with prolong radiation exposure for both the patient and the surgical team. The advent of calcium phosphate for fracture fixation plus the use of the Medtronics O arm (fluoro- navigation) for trocar placement has greatly expanded the indications for pubic rami fracture fixation [12, 13, 14, 15]. Screws are no longer necessary for fixation and do not need to be removed.
This report offers a new option for surgical fixation of pubic rami fractures using percutaneous placement of calcium phosphate using fluoro-navigation. The patient’s image data gives real-time guidance in numerous image planes during the surgery. This study is the first to investigate surgical results of fluoro-navigated surgery in anterior pubic rami fractures using calcium phosphate internal fixation.
Materials and Methods
From April 2018 to December 2019, 30 patients with anterior pubic rami fractures were treated with the Medtronics O arm (fluoro-navigation system) using calcium phosphate fixation. Patients were included in this study if they had displaced, nondisplaced or a minimally displaced closed, anterior pubic rami fractures. General patient data, plus preinjury status, were recorded at admission.
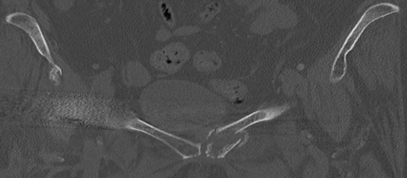
There were 5 men and 25 women, with a mean age of 84.6 years for the females (range 80-104) and average age for the males of 90 years (range 84-99). According to the Young and Burgess classification, all fractures were classified as lateral compression [16, 17]. All patients reported pain as being 10/10 on presentation to the emergency department. Routine AP pelvic films were obtained as well as a pelvic CT scan on admission (Figure 2).
The diagnosis of superior and inferior pubic rami fractures was made from these studies. Preoperative planning was conducted according to the fracture type and soft tissue condition, No patient was excluded, and all were taken to the operating room when their overall medical condition stabilized. All the pubic rami fractures were fixed with calcium phosphate by one surgeon (JMR). Familiarity with the navigation system and the use of calcium phosphate facilitated the timely completion of the procedure.
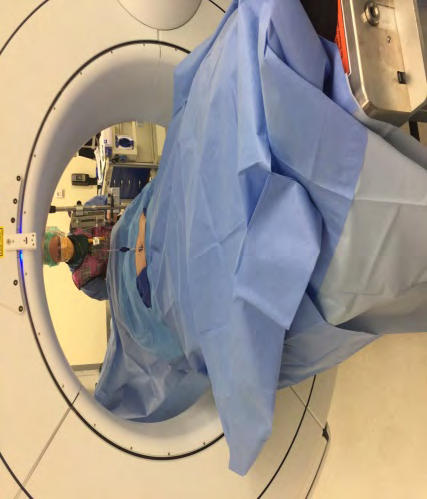
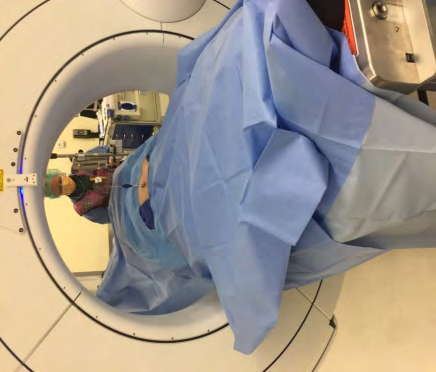
The surgical position was supine on the special radiology table. The O arm was positioned over the patient and centered over the rami fractures (Figure 3). Both side of the anterior pelvis were visualized. Positioning of the patient and the equipment was important for a successful navigational operation. The surgeon was positioned on the right side of the patient and in most cases distal to the O arm position. AP, inlet, and outlet images were collected for the surgery. The O arm in all cases was tilted cephalad to caudad in the fluoroscopy position to help with trocar placement. The spin sequence to check trocar placement within the fractured rami confirmed accurate positioning. No reduction of the fractures was necessary and the fractures were filled with calcium phosphate. Extravasation was noted of the calcium phosphate into surrounding soft tissue which indicated adequate filling of the fracture site.
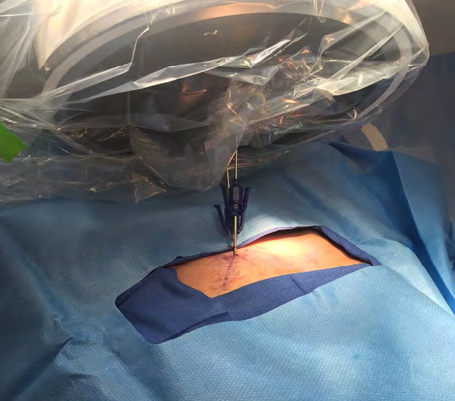
The skin was stabbed, skin and soft tissue were depressed over the superior surface of the pubic symphysis and the trocar sleeve was then inserted into the bone surface. This was done by hand and no drill system was necessary as the bone was osteoporotic. (Figure 4) Multiplanar images were presented, and the trocars could be redirected as needed. The total operating room time was recorded and the total surgical time from surgical start to surgery finish.



Results
A total of 60 trocars were inserted, two trocars per patient. An end delivery trocar was used to access the inferior pubic ramus fracture, and a side delivery trocar for the superior pubic ramus fracture. (Figure 5) 5 cc of calcium phosphate was delivered to each fracture site through the accurately placed trocars under flouro-navigated control. (Figure 6) The average surgical time was 26 minutes for the entire procedure with total OR time averaging 56 minutes. The surgery was minimally invasive with bleeding recorded as minimal No superficial or deep infections were reported as a post-operative complication. No patient sustained a recognized neurologic, vascular, or urologic injury as a result of the percutaneous pubic rami fracture fixation. Extravasation into the surrounding soft tissue did not pose any surgical sequelae post-operatively. (Figure 7) Extravasation was viewed as adequate fracture filling. All the fractures showed union at one year post surgery.
Discussion
Studies have shown 30% of the load of the upper body is transferred to the hips through the anterior pelvic ring [18]. In order to improve stability and prognosis for this area, the pubic rami fractures must be fixed. Closed reduction with percutaneous fixation of nondisplaced or minimally displaced fractures of the anterior pelvic ring is gaining popularity. Minimally invasive procedures of the pelvis, reduce exposure-related hazards and decrease soft tissue disruption. Because of the complex three-dimensional (3D) of the pelvis and the proximity to neurovascular structures, the percutaneous pubic rami fracture fixation is demanding and requires the surgeon to have detailed anatomic knowledge and extensive surgical experience. Navigation surgery aims to replay surgical action performed on a computer monitor in real time [19]. This technique was first used in neurosurgery in 1986 [20, 21]. Now it is widely used in orthopedic operations especially pelvic trauma [22].
With the navigation technique in our surgery, the average surgical time was 26 minutes total per procedure compared to 23.3 minutes per screw placement. The results of this report compared well with the screw placement series The incision was basically 2 small percutaneous sticks. Far less then what is needed for screw placement Surgical post- operative sequelae was nonexistent as no patient sustained a recognized neurologic, vascular, or urologic injury. This proved that the combined technique using calcium phosphate for pubic rami fracture fixation with fluoro-navigation technique was a safe and accurate approach. With the aid of the combined technique of calcium phosphate fixation for pubic rami fractures and flouro-navigation, surgeons can shorten their learning curve for pelvic surgery.
Fluoro -navigation surgery for orthopedic trauma is still at the early clinical stage, this study recommends that nondisplaced or minimally displaced fractures of the pubic rami can be easily fixed with minimally invasive surgery under fluoro-navigation. Our study lacked a control group so we cannot directly compare the clinical results with the conventional percutaneous screw fixation technique. Using calcium phosphate fixation with the O arm (fluoro-navigation technique) could become a safe, accurate, and rapid method for the treatment of anterior pelvic ring fractures involving the pubic rami. Widespread use of calcium phosphate fracture fixation along with the integrated use of the O arm (fluoro-navigation) offers capability to improve patient care.
Conclusions
This study presented for the first time two new techniques for the operative treatment of pubic rami fractures of the pelvis. The delivery of calcium phosphate for fracture fixation of pubic rami fractures has been found to be safe, minimally invasive, providing pain relief and stability permitting early mobilization. The addition of intra- operative fluoro-navigation technique makes the fracture treatment an accurate and rapid method for the treatment of pubic rami fractures. Consistency of the operative technique and teaching are mandatory for the success of this procedure. The learning curve for most orthopedists should be very short. The outcomes have been shown to benefit patient mobilization, decrease morbidity and decrease hospital stay. References
1. Simonian PT, Routt ML, Jr, Harrington RM, Tencer AF (1994) Internal fixation of the unstable anterior pelvic ring: A biomechanical comparison of standard plating techniques and the retrograde medullary superior pubic ramus screw. J Orthop Trauma 8(6): 476-482.
2. Burge R, Dawson-Hughes B, Solomon DH, John B Wong, Alison King, et al. (2006) Incidence and economic burden of Osteoporosis-related Fractures in the United States. 2005-20025. Jone Minor Res 22(3): 465-475.
3. Taillandier J, Langue F, Alemanni, Elodie Taillandier- Heriche (2003) Mortality and functional outcomes of pelvic insufficiency fractures in older patients. Joint Bone Spine 70(4): 287-289.
4. Breuil V, Roux CH, Testa J, Christine A, Madleen C, et al. (2008) Outcomes of osteoporotic pelvic fractures:f 5 An underestimated severity. Survey of 60 cases. Joint Bone Spine 75(5): 585-588.
5. Kannus PP, Palvanen MM, Niemi SS, J Parkkari, M Järvinen (2000) Epidemiology of osteoporotic pelvic fractures in elderly people in Finland: sharp increase in 1979- 1997 and alarming projections for the new millennium. Osteoporosis Int 11(5): 443-448.
6. Melton LJ, Sampson JM, Morrey BF, D M Ilstrup (1981) Epidemiologic features of pelvic fractures. Clin Orthop Relat Res 155: 43-47.
7. Dunn AW, Morris HD (1968) Fractures and dislocations of the pelvis. J Bone Joint Surg Am 50: 1639-1648.
8. Routt ML, Jr, Kregor PJ, Simonian PT, Mayo KA (1995) Early results of percutaneous iliosacral screws placed with the patient in the supine position. J Orthop Trauma 9(3): 207-214.
9. Hong G, Cong-Feng L, Cheng-Fang H, Chang-Qing Z, Bing- Fang Z (2010) Percutaneous screw fixation of acetabular fractures with 2D fluoroscopy-based computerized navigation. Arch Orthop Trauma Surg 130(9): 1177- 1183.
10. Lin YC, Chen CH, Huang HT, Chen JC, Huang PJ, et al. (2008) Percutaneous antegrade screwing for anterior column fracture of acetabulum with fluoroscopic-based computerized navigation. Arch Orthop Trauma Surg 128(2): 223-226.
11. Ray JM (2020) Calcium Phosphate Treatment for Acute Pubic Rami Fractures of the Pelvis: A new approach to Surgical Internal Fixation. J trauma and Treatment 9(1): 1-5.
12. Soles GL, Ferguson TA (2012) Fragility fractures of the pelvis. Cur Rev Musculoskeletal Med 5(3): 222-228.
13. Park S-H, Tofighi A, Wang X, Michael Strunk, Thomas Ricketts, et al. (2011) Calcium phosphate combination biomaterials as human mesenchymal stem cell delivery vehicles for bone repair. J Biomed Mater Res 97(2): 235- 244.
14. Sharkey PF, Cohen SB, Leinberry CF, Javad Parvizi (2012) Subchondral bone marrow lesions associated with knee osteoarthritis. Am J Orthop 41(9): 413-417.
15. Miller JR, Dunn KW (2015) Subchondroplasty of the ankle: a novel technique. Foot Ankle Online J 8(1): 1-7.
16. Young JW, Burgess AR, Brumback RJ, A Poka (1986) Pelvic Fractures: value of plain radiography in early assessment and management. Radiology 160(2): 445- 451.
17. Dalal S, Burgess A, Seigel J, Young JW, Brumback RJ, et.al. (1989) Pelvic fractures in multiple trauma: Classification by mechanism is key to pattern organ injury, resuscitative requirements, and outcome. J Trauma. 29(7): 981-1000.
18. Keating JF, Werier J, Blachut P, Broekhuyse H, Meek RN, et al. (1999) Early fixation of the vertically unstable pelvis: The role of iliosacral screw fixation of the posterior lesion. J Orthop Trauma 13: 107–113.
19. Nolte LP, Beutler T (2004) Basic principles of CAOS. Injury 35(1): S.
20. Tian ZM (2001) Clinical evaluation of neouronavigation and frameless stereotaxy in minimally invasive neourosurgery. Chin Med J 81(17): 1028-1029.
21. Nolte LP, Visarius H, Arm E, Langlotz F, Schwarzenbach O, et al. (1995) Computer-aided fixation of spinal implants. J Image Guid Surg 1(2): 88-93.
22. Xu P, Wang H, Liu ZY, Mu WD, Xu SH, et al. (2013) An evaluation of three-dimensional image-guided technologies in percutaneous pelvic and acetabular lag screw placement. J Surg Res 185(1): 338-346.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results