Case Report: Idiopathic Chondrolysis of the Hip
Idiopathic chondrolysis of the hip (ICP) is a rare condition of unknown etiology duo to progressive destruction of the hyaline cartilage that covers the femoral head and acetabulum. It has insidious beginning and affects more often female adolescents. This study aimed at reporting one case of that rare disease of a 14-year-old male adolescent with idiopathic chondrolysis of the hip presented to our out -patient clinic after three months of symptoms beginning. Early diagnosis is challenging. Clinicians must be aware of this rare diagnosis, because early diagnosis may improve the patient outcome.
Owayed Ali Almutairi1*, Awdhah Abdulkareem2 and Ahmad Elarabi2
Introduction
In the literature, the description of idiopathic chondrolysis of the hip in the adolescent age group is rare, being mostly found in case reports [1]. It’s is found affecting female adolescents (80%) of Asian or African ethnicity, with the complain of hip pain and limbing and is more commonly monoarticular (60% affects the right side). Bilateral occurs in 5% of the cases [1].
Chondrolysis can occur as an apparently idiopathic event or secondary to other hip pathologies, should be considered in the differential diagnosis of the monoarticular involvement of the hip. Magnetic resonance imaging plays an important role in the diagnosis and follow-up of patient prognosis [1]. The management usually consists of analgesics, physical therapy According to the literature, remission occurs in 54% of the cases. The surgical treatment was also reported in some case reports include capsulotomy with or without psoas and/or adductor tonotopy, hip arthrodesis and arthroplasty, but the results are not promising [2].
The major indications to proceed with procedures are no pain improvement, correct deformity and achieve good hip range of motion.
In this case report we present a case of a fourteen-year- old male presented in out-patient clinic with complain of hip pain and limping for three-month duration after full investigation idiopathic chondroplasties of the hip was the final diagnosis.
Fourteen-year-old male no past medical or surgical history, No known allergy for any food or medication, No past family history of similar condition or rheumatologically diseases presenting to the outpatient clinic with complain of sudden liming and pain while walking located in left hip for three- month duration, with no other associated symptoms, pain was exacerbated with any hip movement, present at rest. There was no change in pain with time of day. No fever rash, or lymphadenopathy was present.
No history of previous trauma or history of recent infection.
O/E Patient was alert, conscious, oriented Vitally stable afebrile Temperature = 37, pulse = 73 BP= 130/60 Patient walking with a crutches for three-month duration The left lower limb was externally rotated Limited range of motion of the left lower limb= 20-70, no rotation noticed decrees knee extension Good skin condition, no tenderness no erythema no warmth on palpation at bilateral hip joints.
Other systemic examination: Chest: equal bilateral air entry no added sound Heart: S1 + S2 no added sound Abdomen: soft and lax, no tenderness, no organ-omega Nervous system: intact Patient for the three month did not receive any treatment or do any physiotherapy.
LAB investigations: all labs are within the normal range
▪
Hemoglobin= 15, urea =68, creatine =61, Na= 141, K
4.3 ▪
Blood culture: no growth after seven days’ incubation
▪
Urine culture: no growth after 24 hours’ incubation
$$ \begin{array}{l} E S R = 4 \\ W B C = 1 0. 1 X 1 0 ^ {\wedge} 9 / L \\ \end{array} $$
- CRP= 2.58
- Rheumatoid factor: normal
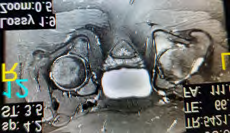
Radiological Evaluation
MRI lumbosacral spine: L3-4 & l4-5 mild diffuse disc bulge, reduce lumbar lordosis Differential diagnosis:
- Septic arthritis
- Synovitis
- Reactive arthritis
- slipped capital femoral epiphysis

After a detailed discussion with the family and the surgical orthopedic team regarding the differential diagnosis treatment options, postoperative rehabilitation, risks and complications patient was admitted to the hospital for hip joint aspiration for further evaluation.
During hospital stay: Sample Aspiration of hip joint done under general anesthesia cultures were sending to lab for further evaluation:
- Specimen A showed: 15 ml of hemorrhagic fluid from superficial lateral posterior hip joint; smear showed mainly blood cells and acute inflammatory infiltrates no malignant cells are seen
- Specimen B showed: 8ml of hemorrhagic fluid from deep posterior region of hip smear showed blood cells, lymphocytes and macrophages no malignant cells are seen cultures no growth after 5 days’ growth.
After a detailed discussion with the family and the surgical team regarding his case and more research was done diagnosis of idiopathic chondrolysis of the hip (ICP) After detailed researched the patient was managed by: Early range of motion exercise and aggressive physiotherapy done for him for two-month duration.
Follow up after two months: Pains were relived but still decrease range of motion and mild limping was found. There phase bone scan & SPECT/ CT was done for further evaluation: active bone abnormality in the left hip joint region likely secondary to osteo-arthritic changes findings are in line with the referring diagnosis of idiopathic chondrolysis. No significant photon deficit abnormality seen in any phase of the study rendering the scintigraphy possibility left hip AVN is less likely.
Patient was happy and satisfied with his progression, advices to continue physiotherapy and future evaluation in out-patient clinic after three months.
Discussion
Idiopathic chondrolysis of the hip (ICP) first described in the early 1900s as found in the literature, and was also found in in 1971 with clinical records of 9 patients aged between 9 and 16 years [2]. In 1975, Duncan1 reported five patients with the same condition and used the term “Idiopathic Chondrolysis of the Hip” to describe this phenomenon [3]. chondrolysis of the hip was initially identified in patients following slipped capital femoral epiphysis. Later, patients with no clear etiology were diagnosed, history of trauma, burns, infection, and prolonged immobilization have also been described. The onset is early in the second decade of life with approximately 6:1 female gender predominance [3] ICH usually manifests as hip pain and/or radiated pain to the knees. The diagnosis is rare but can be achieved with clinical examination (hip pain and limping) and radiographic fining (joint space narrowing; acetabular protrusion; subchondral cysts; joint erosion; pre- mature closure of the growth plate; and lateral increase of the femoral head) [1].
The magnetic resonance imaging findings of ICH included early subchondral edema, joint effusion and bone marrow edema; on the progression, focal loss of the cartilage, muscle mass loss and acetabular and femoral remodeling occur [4]. After excluding all the other differential diagnosis with normal lab investigations the final diagnosis of ICH can be concluded the course from presentation to almost remission is variable, with an acute phase lasting 6-16 months followed by a chronic stage of 3-5 years. [3]. When left untreated, the natural history of this disease often leads to complete or near-complete ankylosis of the joint.
We believe that the early diagnosis, treatment, and the rapid institution of physical therapy were important factors for successful management [5, 6, 7].
Conclusion
Idiopathic chondrolysis of the hip is a challenging diagnosis with devastating complications.
Early clinical suspicion must remain high among clinicians Ultimately, most patients experience a spontaneous resolution of pain, develop early arthritis, and often arthrodesis. Positive features that aid in the early diagnosis of ICH are the age, sex, and race of the patient presenting with hip pain and with no history of trauma or systemic illness. Early diagnosis is important, as early treatment with physical therapy can ensure the patient maintains flexibility and avoids contractures and pain relive.
References
-
Ana Paula Sakamoto, Larissa Lucati Ramos, Artur da Rocha Corrêa Fernandes, Maria Teresa Terreri (2013) Chondrolysis of the hip in an adolescent: clinical and radiological outcomes. Rev Bras Reumatol 53(2): 215- 218.
-
Shiro Hirose, Hiromi Otsuka, Takkan Morishima, Kazutaka Watanabe, Keiji Sato (2014) Idiopathic Chondrolysis in Adults Treated with Surgical Dislocation of the Hip. Ann Orthop Rheumatol 2(1): 1010.
-
Startzman AS, Hawkes T and Beterand S (2016) Juvenile Idiopathic Chondrolysis of the Hip. J Trauma Treat 5: 312.
-
Tal Laor, Alvin H Crawford (2019) Idiopathic Chondrolysis of the Hip in Children: Early MRI Findings. 192(2): 526- 531.
-
A W Hughes (1985) Idiopathic chondroplasties of the hip: a case report and review of the literature. Ann Rheum Dis 44(4): 268-272.
-
Shefali Gupta, Mahesh M (2015) Idiopathic chondrolysis of the hip. J Orthop Allied Sci 3: 68-71.
-
Jens François, Michiel Mulier (2007) Idiopathic chondrolysis of the hip A case report. Acta Orthop Belg 73: 653-657.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results