The "Horse Saddle" Sign: A New Ultrasound Sign for Osteoarthritis
Objective: To assess the sensitivity and specificity of the “horse saddle” sign in the diagnosis of osteoarthritis Methods: An exploratory clinical comparative cross-sectional study where an ultrasound of the hands and comparative radiographs in PA view were performed on patients with osteoarthritis, inflammatory arthritis and healthy patients seen in the Rheumatology clinic of the Vall de Hebron Hospital. Age, sex and time of evolution of the disease were collected as clinical variables. The MCP, PIP and DIP joints from the second to the fifth finger of both hands were viewed with grayscale in longitudinal and transverse plane of both the dorsal and palmar face, assessing for osteophytes, synovitis and the horse saddle sign. Results: A total of 38 patients with osteoarthritis, 20 patients with inflammatory arthritis (8 psoriatic, 9 RA, 1 LES, 1 PMR and 1 Sjogren) and 2 healthy patients were assessed. It was found that the horse saddle sign had a sensitivity of 66.7% and specificity of 86.4% in osteoarthritis showing a p-value of 0.052 by means of the chi-square test. 87% of patients with the horse saddle sign had osteoarthritis and only in 2 patients with RA and in the patient with LES. Conclusion: The horse saddle sign is an ultrasound sign with good sensitivity and specificity for the diagnosis of hand osteoarthritis comparable to other classic ultrasound signs such as osteophytes and synovitis.
Introduction
Musculoskeletal ultrasound (US) is an imaging technique that has more and more acceptance for diagnosis and monitoring in rheumatic diseases given its increasing availability in hospital centers and its safety. In osteoarthritis there are numerous studies on the usefulness of ultrasound, and it has been accepted as a great tool for the diagnosis and even for the assessment of inflammatory changes in the disease [1, 2, 3, 4, 5, 6]. The changes that are seen mainly in osteoarthritis and help in its diagnosis are synovial hypertrophy, effusion, osteophytes and joint cartilage involvement [7]. It has been demonstrated by ultrasound that osteophytes, the classic lesion of the disease, can be seen earlier than with plain x-rays [8].
Other studies have described that the most specific ultrasound signs of osteoarthritis are damage in articular cartilage and osteophytes [9], just as another study demonstrated osteophytes as the most predominant lesion [10]. It is also stated that the absence of Doppler in synovitis and the absence of erosions are more related to osteoarthritis.
Another finding that is also associated with osteoarthritis valuable by ultrasound is the presence of synovial cysts at the edge of the joint [7]. However, these findings, although sensitive, may be not very specific since they are also observed in inflammatory arthritis and erosive osteoarthritis [7]. It has been demonstrated by magnetic resonance imaging that pathology can even be seen in the collateral ligaments of the fingers due to osteoarthritis [11]. However, this has not yet been adequately studied by ultrasound, probably due to the difficulty that exists to visualize these anatomical structures through this technique.
Throughout our clinical practice in osteoarthritis of the hands, we have seen, over repeated examinations, a bone morphological change not previously described in the literature we have described as the “horse-saddle” sign. This sign that we have not found specifically described in the literature reviewed to date is considered to be useful for the diagnosis and therefore the objective of the study is to demonstrate the specificity and sensitivity in the diagnosis of osteoarthritis and thus see its reliability in the diagnosis of the very common disease that is osteoarthritis.
Materials and Methods
We designed a transversal, comparative exploratory study on a cohort of patients with hand osteoarthritis, inflammatory arthritis and healthy controls. All patients with hand osteoarthritis needed to fit in the ACR hand osteoarthritis diagnostic criteria. All subjects were obtained from the rheumatology clinic at Valld’ Hebron Hospital in Barcelona, Spain from January 2018 to March 2020. All patients needed to be above 18 years of age and be capable of understanding and signing informed consent before begin study procedures. Data were collected and codified to protect data confidentiality. Patients with secondary osteoarthritis due to inflammatory diseases and those with hand surgery done in the past were excluded. After signing informed consent and assigned a study code, the subjects were seen in one visit to collect clinical data. Age, sex, time the disease was diagnosed and disease diagnosis were recorded as variables. All patients needed to have a comparative anteroposterior view x-ray of the hands in the recent year, and if they did not have it, they were taken one for the study. The study received authorization from the Hospital’s ethics committee with reference number PR (AG) 69/2019.
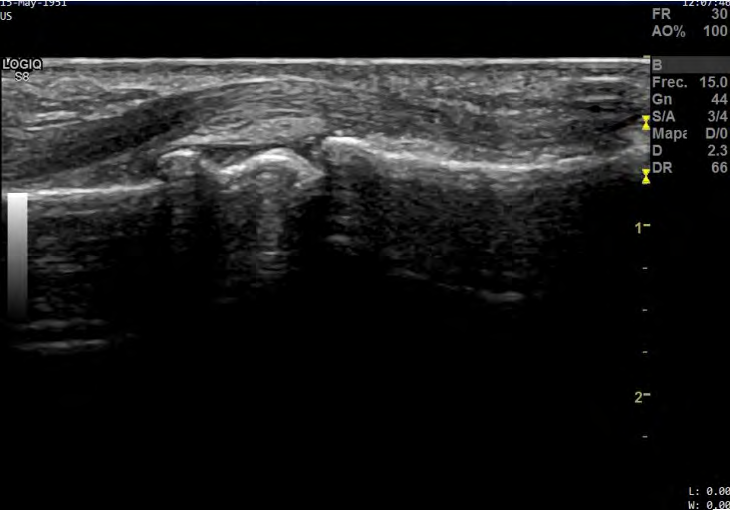
The ultrasound study was done by an expert rheumatologist in musculoskeletal ultrasound that was blinded to clinical data, x-rays and patient’s diagnosis. The joints studied by grey scale ultrasonography were the metatarsophalangeal, proximal interphalangeal and distal interphalangeal of the second, third, fourth and fifth fingers of both hands. We chose the above mentioned joints because these are the joints we have seen most affected by the “horse- saddle” sign in our usual clinical practice. Ultrasound scan was done both longitudinal and transverse plane from both the dorsal and palmar side of the hand. For the purpose of the study only the presence of osteophytes, synovitis and the “horse-saddle” sign were recorded. The “horse-saddle” sign it is a bone extension in the head of the phalanx of the finger joints that causes a deformity that we have called a “horse-saddle” and is typically located in the proximal and distal interphalangeal joints of the fingers. This sign can be seen in the longitudinal exploration of the palm of the hand by grayscale ultrasound (Figure 1). All ultrasound screenings were done with a General Electric Logiq S8 R3 machine and a linear 8-13 MHz probe Gray scale and power Doppler settings (medium dynamic range, medium persistence, medium frame rate, low wall filter, 0.8Hz pulse repetition frequency) were identical throughout the examinations. Room temperature was stable and kept at 25°C with average lighting.
For statistical analysis, first a descriptive analysis of each of the variables is presented by means of frequencies and percentages. The chi-square test is shown that in the case of measurements at different points it would be expected that they had a p value of less than 5%. Secondly, an analysis is made of the diagnostic measures sensitivity, specificity and positive and negative predictive values, as well as the likelihood ratios. For each measure, the 95% confidence interval is calculated. The analyzes have been carried out with Stata 15.1.
Results
A total of 52 patients were recruited for the study being 30 patients classified with primary osteoarthritis, 20 patients classified with inflammatory arthritis and 2 patients classified as healthy subjects. The average age of the patients recruited was 59.82 years and the average years with diagnosis were 8.36 years. A total of 37 patients were female and 15 patients were male of the 20 patients with inflammatory arthritis 9 patients had rheumatoid arthritis,
8 patients had psoriatic arthritis, 1 patient had systemic lupus erythematosus (SLE), 1 patient had Sjogren Syndrome and 1 patient had polymyalgia rheumatica (PMR). The descriptive statistical analysis of the variables by means of frequencies and percentages is shown in Table 1. We found that the “horse-saddle” sign had a calculated sensitivity of 66.7% and specificity of 86.5% for the diagnosis of primary osteoarthritis with a p value of 0.052. The percentage of false negatives was calculated as 33.3% and the false positives were calculated as 13.64%. The positive predictive value was calculated as 86.96% and the negative predictive value was calculated as 65.52%. In general, 87% of patients with osteoarthritis had a “horse-saddle” sign and only 2 patients with rheumatoid arthritis and the one patient with SLE had it as we can see in Table 2 describing the relationship of “horse-saddle” sign by diagnosis.
- Variable
- Osteoarthritis
- Total p-value
- No
- Yes
- Sex1
- Male
- 7 (46.67%)
- 8 (53.33%)
- 15 (100%)
- 0.68542
- Female
- 15 (40.54%)
- 22 (59.46%)
- 37 (100%)
- 22
- 30
- 52
- Age3
- 65.10 (10.26)
- 59.83 (13.67)
- 0.0007
- 52.64 ( 14.63)
- 52.00(42.00;58.00)
- 66.50(56.00;70.00)
- 57.50(51.50;70.00)
- 0.00224
- Synovitis1
- No
- 17 (54.84%)
- 14 (45.16%)
- 31 (100%)
- 0.02632
- Yes
- 5 (23.81%)
- 16 (76.19%)
- 21 (100%)
- Osteophytes1
- No
- 10 (100%)
- 0 (0%)
- 10 (100%)
- < .00015
- Yes
- 12 (28.57%)
- 30 (71.43%)
- 42 (100%)
- “Horse-saddle” Sign1
- No
- 19 (65.52%)
- 10 (34.48%)
- 29 (100%)
- 0.00012
- Yes
- 3 (13.04%)
- 20 (86.96%)
- 23 (100%)
- Osteoarthritis X-ray1
- No
- 21 (100%)
- 0 (0%)
- 21 (100%)
- <0.00012
- Yes
- 1 (3.23%)
- 30 (96.77%)
- 31 (100%)
Table 1: Descriptive Analysis of the Patients Findings.
- 1: n (percentage row), 2: Chi-squared test, 3: N, 4: t-test / U Mann-Whitney test, 5: Fisher’s exact test
- MCP: Metacarpophalangeal joint; PIP: Proximal Interphalangeal joint; DIP: Distal Interphalangeal joint; RH: Right hand; LH: Left hand.
- Variable
- Diagnosis
- Total p-value
- Healthy
- OA
- RA
- PsA
- SLE
- PMR
- SS
- No
- 2
- 10
- 7
- 8
- 0 (0%)
- 1
- 1 (100%)
- 29
- 0.0004 2
- -100%
- -33.33%
- -77.78%
- -100%
- -100%
- -55.77%
- “Horse-
- Saddle”
- Sign1
- Yes
- 0 (0%)
- 20
- 2
- 0 (0%)
- 1 (100%)
- 0 (0%)
- 0 (0%)
- 23
- -66.67%
- -22.22%
- -44.23%
Table 2: Descriptive Analysis of the “Horse-Saddle” Sign According to Diagnosis.
The sensitivity for synovitis in osteoarthritis was calculated as 53.33% and the specificity was calculated as 77.2% with a p value of 0.039. The percentage of false negatives was calculated as 46.67% and the false positives were calculated as 22.7%. The positive predictive value was calculated as 76.19% and the negative predictive value was calculated as 54.84%. As expected, there was a low frequency of synovitis in osteoarthritis patients being the most affected joint the 2nd DIP of the right hand seen in 7 patients.
The sensitivity for osteophytes in osteoarthritis was calculated as 100% and the specificity was calculated as 45.45% with a p value of 0.001. The percentage of false negatives was calculated as 0% and the false positives were calculated as 54.55%. The positive predictive value was calculated as 71.43% and the negative predictive value was calculated as 100%. Of notice we have also found a high frequency of osteophytes localized in PIP and DIP joints of both hands being present in an average of 84.8% and 83.5% of patients, respectively. There was also a high frequency of osteophytes in the 2nd MCP joint of the left hand being present in 85.7% of patients with osteoarthritis.
Discussion
The “horse-saddle” sign is a form of bone proliferation that differs significantly from a common osteophyte seen using high-frequency ultrasound. We appreciated this special morphology in routine examinations and decided to propose a research project to clarify if this sign could help us in the diagnosis of osteoarthritis. As we can see, from the results obtained in our study, the “horse-saddle” sign is a reliable ultrasonographic sign for the diagnosis of primary osteoarthritis with a good sensitivity and specificity. It can be compared with other classic signs like osteophytes, synovitis and even a superior sensitivity and specificity compared with conventional osteophytes. Our study is the first identifying and evaluating this sign.
Sometimes it can be difficult to distinguish between an inflammatory arthritis like rheumatoid arthritis from osteoarthritis in ultrasound imaging. Therefore, finding more options that can help us discriminate between inflammatory and degenerative rheumatic diseases can simplify our daily clinical practice. A study done by Vlychou and colleagues found that many patients with osteoarthritis can also show the presence of synovitis, erosions and Doppler signal which are classic signs suggestive of inflammatory pathology [12]. Not much have been explored in ultrasonographic signs of osteoarthritis apart from osteophytes and mostly has focused in developing scoring system rather than specific signs. Kunkel et al for example explored an ultrasonographic index in which they discriminated osteoarthritis from rheumatoid arthritis by focusing on predominance of osteophytes, absence of erosions, absence of doppler signal and synovitis that does not surpass >2mm over the diaphysis but as such not an specific ultrasound sign to discriminate both diseases [13]. An ultrasound based diagnostic index was explored under the idea that if there activity index can help to value disease activity a diagnostic index can also be designed to separate inflammatory from degenerative pathology and as such achieve a sort of “ultrasonographic diagnostic criteria”. Kunkel and colleagues belief that establishing an ultrasonographic diagnostic criterion to separate inflammatory from degenerative pathology is vital for daily clinical practice [13]. We belief that the “horse-saddle” sign can be a special osteophyte deformity specific to primary hand osteoarthritis making it a frequent sign that can be seen in osteoarthritis patients. Not much attention has been given to if there are specific types of osteophytes that could be specific to osteoarthritis. Most recent work has been focused more in classifying osteophytes by size, as we can see in projects by an OMERACT working group and Hammer HB, et al. [14]; Mathiessen A, et al. [15]. As some studies have done to evaluate the osteophytes in other imaging modalities like tomography and conventional radiography we can also do studies using ultrasonography that can help to evaluate the type of osteophyte seen in degenerative pathology [16, 17]. Some aspects can be considered for future studies, the frequency of the sign in secondary forms of osteoarthritis which we did not analyzed in our study to not interfere with the analysis of the sign in primary osteoarthritis; as well as analyze a period in time in which the “horse-saddle” sign can be more sensitive in diagnosis following patients with early signs and diagnosis of osteoarthritis and following their progression through a specific time period.
A possible weakness of our study is sample size. Many could consider our sample small in size, yet we included enough patients to obtain a representative sample that could give us enough statistical significance. As controls we also used many different inflammatory pathologies and it can be mentioned that a more uniform inflammatory arthritis control can make a better comparison with other pathologies in the value of the “horse-saddle” sign in the differential diagnosis of osteoarthritis. This gives us further study ideas that can help to explore the validity of the “horse-saddle” sign in degenerative disease.
Overall, we believe the “horse-saddle” sign is a reliable sign that can help us in the diagnosis of primary osteoarthritis and differentiating it from other common hand rheumatic diseases. We propose this ultrasonographic sign as a tool to help diagnosis in patients with suspicion of osteoarthritis disease.
References
-
Iagnocco A, Naredo E (2012) Osteoarthritis: research update and clinical applications. Rheumatology (Oxford) 51(S 7): 2-5.
-
Guinsburg M, Ventura-Ríos L, Bernal A, Hernández-Díaz C, Pineda C (2013)[Usefulness, validity, and reliability of ultrasound in the diagnosis of osteoarthritis: a critical review of the literature]. Gac Med Mex 149(5): 509-520.
-
Iagnocco A (2010) Imaging the joint in osteoarthritis: a place for ultrasound? Best Pract Res Clin Rheumatol 24(1): 27-38.
-
Keen HI, Conaghan PG (2009) Usefulness of Ultrasound in Osteoarthritis. Rheum Dis Clin North Am 35(3): 503- 519.
-
Okano T, Mamoto K, Di Carlo M, Salaffi F (2019) Clinical utility and potential of ultrasound in osteoarthritis. La radiologia medica 124: 1101-1111.
-
Amorese-O’Connell L, Gutierrez M, Reginato AM (2015) General Applications of Ultrasound in Rheumatology Practice. Fed Pract 32(S12): 8S-20S.
-
Iagnococo A, Palombi GV (2016) Role of ultrasound in osteoarthritis. J Clin Rheumatol 28(7): 301-306.
-
Keen HI, Wakefield RJ, Grainger AJ, Hensor EMA, Emery P, et al. (2008) An ultrasonographic study of osteoarthritis of the hand: Synovitis and its relationship to structural pathology and symptoms. Arthritis Rheum 59(12): 1756-1763.
-
Ventra Rios L (2010) Musculoskeletal Ultrasound Manual. Panamerican Medical Publishing House.
-
Abraham AM, Pearce MS, Mann KD, Francis RM, Birrell F (2014) Population prevalence of ultrasound features of osteoarthritis in the hand, knee and hip at age 63 years: The Newcastle thousand families birth cohort. BMC Musculoskelet Disord 15(1): 162.
-
Tan AL, Toumi H, Benjamin M, Grainger AJ, Tanner SF, et al. (2006) Combined high-resolution magnetic resonance imaging and histological examination to explore the role of ligaments and tendons in the phenotypic expression of early hand osteoarthritis. Ann Rheum Dis 65(10): 1267-1272.
-
Vlychou M, Koutroumpas A, Malizos K, Sakkas LI (2009) Ultrasonographic evidence of inflammation is frequent in hands of patients with erosive osteoarthritis. Osteoarthritis Cartilage 17(10): 1283-1287.
-
Kunkel G, Cannon GW, Clegg DO (2012) Combined Structural and Synovial Assessment for Improved Ultrasound Discrimination of Rheumatoid, Osteoarthritic, and Normal Joints: A Pilot Study. Open Rheumatol J 6(1): 199-206.
-
Hammer HB, Iagnocco A, Mathiessen A, Filippucci E, Gandjbakhch F, et al. (2016) Global ultrasound assessment of structural lesions in osteoarthritis: a reliability study by the OMERACT ultrasonography group on scoring cartilage and osteophytes in finger joints. Annals of the Rheumatic Diseases 75(2): 402-407.
-
Mathiessen A, Haugen IK, Slatkowsky-Christensen B, Boyesen P, Kvien TK, et al. (2013) Ultrasonographic assessment of osteophytes in 127 patients with hand osteoarthritis: Exploring reliability and associations with MRI, radiographs and clinical joint findings. Ann Rheum Dis 72(1): 51-56.
-
Finzel S, Sahinbegovic E, Kocijan R, Engelke K, Englbrecht M, et al. (2014) Inflammatory Bone Spur Formation in Psoriatic Arthritis Is Different From Bone Spur Formation in Hand Osteoarthritis. Arthritis Rheumatol 66(11): 2968-2975.
-
Buckland-Wright JC, MacFarlane DG, Lynch JA (1991) Osteophytes in the osteoarthritic hand: Their incidence, size, distribution and progression. Ann Rheum Dis 50(9): 627-630.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results