Systematic Review and Meta-Analysis of Patient Reported Outcome and Return to Work after Surgical vs Non-Surgical Mid Shaft Humerus Fracture
Background: Several recent reviews demonstrate that in patients with humeral shaft fractures, surgical therapy has lesser risks of non-union, mal-union, and re-intervention than non-surgical therapy. These positive clinical outcomes of the surgical approach make it a preferable treatment option despite the risks of radial nerve palsy and additional surgery-related risk. We aimed to evaluate patients' outcomes and return to work after surgical vs. non-surgical management of shaft humeral fracture. Methods: We used databases, including PubMed, Medline, and Cochrane Register of Controlled Trials from 2010 to January 2022 to search potential randomised controlled trials (RCTs) and cohort studies comparing the patients' related outcome measures and return to work between surgical and non-surgical management of humerus fracture. Results: After carefully evaluating 1352 articles, we included three RCTs (232 patients) and one cohort study (39 patients). The surgical intervention used plate/ nail fixation, while the non-surgical intervention used splint or brace procedure to manage shaft humeral fracture. The pooled DASH effects of all three RCTs at six (M.D: -7.5 [-13.20, -1.89], P: 0.009) I2:44%) and 12 months (M.D: -1.32 [-3.82, 1.17], p:0.29, I2: 0%) were higher in patients treated surgically than in non-surgical procedures. The pooled constant Murley score at six (M.D: 7.945[2.77,13.10], P: 0.003) I2: 0%) and 12 months (M.D: 1.78 [-1.52, 5.09], P: 0.29, I2: 0%) were higher in patients who received non-surgical than surgical therapy. However, pooled analysis for patients returning to work for both groups remained inconclusive. Conclusion: Altogether, we found no significant evidence supporting the clinical benefits of surgical over non-surgical therapy. Thus, the non-surgical approach remains the preferred therapeutic choice for managing shaft humeral fractures due to its lesser side effects.
Introduction
Recent advancements in industrialization and transport facilities have increased the number of trauma cases worldwide. Humeral shaft fractures (HSF) account for 1—3% of all orthopaedic fractures in adults [1, 2]. The overall annual incidence of HSFs is 10 / 100,000. The age-specific incidence of HSF shows a bimodal distribution, with the first peak occurring in the young men in their 20s and the second peak occurring in the elderly women in their 70s. After the fifth decade of life, the incidence of HSF decreases among men and increases among women. Additionally, elderly women have seven times more risk of acquiring HSF than age-matched men [3].
Motor vehicles crash, simple falls, and sports injuries are common causes of HSF. In 2008, the HSFs accounted for approximately 60000 emergency department visits in the United States alone [4]. The traditional therapy of HSF includes the non-surgical procedure, involving functional bracing, cast, or splints. The major problem associated with non-surgical intervention is non-union, as up to 33% of HSFs treated non-surgically present with non-union [5, 6].
The advanced surgical procedures cause several complications, including radial nerve palsy and infections [7]. A randomised controlled trial (RCT) comparing surgery with functional bracing demonstrated no clinically significant differences in patient-reported outcomes. Additionally, 15% of patients with a non-union fracture in the non-operative arm had secondary [8].
However, the emphasis is changing from simply accomplishing bone union to achieving perfect axial alignment, length, and rotational stability. Surgical interventions are routinely adopted for obtaining the same outcome despite a longer duration of immobilisation than conservative treatments. The rate of operative invasive procedures for HSF has progressively increased. In support of this, Scoch, et al. reported that up to 60 % of HSF were treated surgically in the US between 2007-2011 [9].
The annual incidences of humeral shaft fracture (HSF) in the working and elderly population is 14-15 per 100,000 and 60 per 100,000, respectively. These fractures cause occupational disability among the working population. Therefore, it is critical to better understand the HSF and the outcomes of its treatment options for optimizing the functional recovery and return to work [10, 11].
Sarmiento et al. favoured conservative therapy of HSF, reporting a 97 % union rate in a cohort of 922 patients [12]. Nevertheless, recent studies have failed to replicate such a high union rate. For example, the non-surgical management of proximal and transverse HSFs have 20-50% non-union rates [7, 13, 14]. In the recent decade, intramedullary nailing or plate osteosynthesis has become the most common surgical procedure to enhance functional outcomes and prevent non-unions [9].
Open reduction paired with plate fixation demonstrates direct visualization of fracture that provides rigid fracture fixation. Thus, rigid fixation provides early mobilization of the affected extremity, reduces pain and ensures an earlier return to daily activities. Stable fracture fixation prevents osteoporosis and joint stiffness [15]. Conservative therapies are associated with intense pain and delayed mobilization, which affects function recovery and returning to normal activities. Nevertheless, limited evidence is available to compare the patient’s reported outcomes among non- surgical and surgical approaches for HSF [7, 16, 17].
This study aims to fill this gap in literature by systemically investigating the treatment options and their outcomes related to HSF. We hypothesise that patients with HSF treated with surgical intervention demonstrate an earlier return to work and better patients-related outcomes than the patients on conservative treatments.
Methodology
Design
This study compared the patient’s reported outcomes and return to work after surgical vs. non-surgical management of HSF following Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) [18].
Literature Search Strategy and Database
Two authors explored the Cochrane register of controlled trials, PubMed, and Medline database from 2010 to January 2022. We performed electronically searched across these databases to discover the potential articles using keywords and MESH terms: humerus, Shaft; humeral; Diaphysis; Surgical; Fixation; osteosynthesis; operative; plate; intramedullary; conservative; functional bracing; non-operative. We used Boolean operators and relevant keywords to find their intersection. Additionally, the searched keywords were matched based on a different database. We also manually checked the reference of eligible studies, relevant abstract and narrative reviews. The full search terms used in Pubmed were as follows: (‘‘humerus’’[MeSH Terms] OR humeral[Title]) AND (Shaft[Title/Abstract] OR diaphysis[Title/Abstract]) AND (surgical[Title/Abstract] OR fixation[Title/Abstract] OR osteosynthesis[Title/ Abstract] OR operative[Title/Abstract]) OR plate [Title/Abstract] OR intramedullary [Title/Abstract] AND (conservative[Title/ Abstract] OR functional bracing[Title/Abstract] OR non- operative[Title/Abstract)]. In the case of published abstracts of protocols, authors were contacted for preliminary results.
Study Criteria
We included only those articles that met the following study criteria: RCTs or cohort study, patients with HSF, patients above 16 years of age, both gender, direct comparison of surgical management to non-surgical management, studies assessing any patients-related outcome, including return to work, Studies with non-operative and operative techniques like plate fixation, intramedullary fixation, and external fixation. Articles search was restricted to human patients and English language.
The articles were excluded if the article met the following exclusion criteria: review articles, no full text available, editorial letter/ commentaries, non-research letter, animal studies, case reports or case series, patients with chronic fractures, pathological fractures, conference abstracts, Direct comparison of surgical techniques without a non-operative cohort.
Study Selection, Data Extraction, and Study Quality Assessment
Two authors (N.H., S.A.) independently assessed each identified article to eliminate articles that did not meet the inclusion or exclusion criteria. An independent third-party reviewer (J.A.) resolved any discrepancies. We independently performed a full-text screening if the abstract of identified articles could not demonstrate specific outcomes. We performed data extraction into a predefined data sheet using Microsoft word.
Two reviewers (N.H., S.A.) independently extracted article details like country, study period, study design, the sample size in surgical and non-surgical group, mean age, treatment modalities, Sex, AO (arbeitsgemeinschaft für osteosynthesefragen) classification, and follow up.
Outcome Measure
The primary outcome was patients reporting functional outcomes like disabilities of the arm, shoulder, and hand (DASH), Short Form-36, Constant-Murley shoulder score, pain intensity on a visual analogue scale (VAS) and return to work. We measured these outcomes at six and 12 months.
Statistical Analysis
The fixed and random effect model was used to estimate the overall effects of primary outcomes. The outcome was presented as continuous variables like means, standard deviation, mean difference, 95% confidence interval, and sample size across each group. I2 statistic determined heterogeneity level. Fixed effects model was used to estimate overall effects for low or minimal heterogeneity, while random effects for moderate and substantial heterogeneity. We used comprehensive meta-analysis (CMA) software version 3 to estimate the overall effect of primary outcomes and created a forest plot to present the outcomes (20). The pooled effect was considered as statically significant at P-value < 0.05.
Risk of Bias (ROB) Assessment
The ROB of eligible randomised controlled trials was performed using the Cochrane risk of bias tool [19], while ROB for observational cohort study was performed using the ROB in non-randomised studies of interventions (ROBINS-I) [20]. These tools evaluated the quality for the following domains: participants selection, confounding, interventional classification, missing data, deviation from intent, outcome measurement, selection of results, and overall study quality. All eligible articles were arbitrated as critical, serious, moderate, or low.
Results
Literature Search
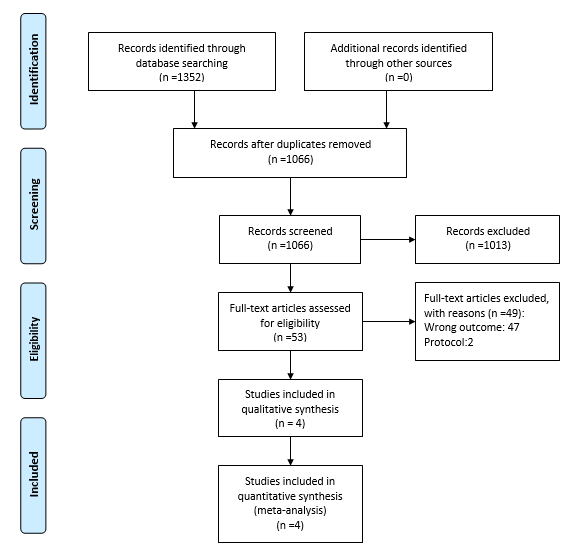
The initial electronic search yielded 1352 articles (Figure 1). A total of four articles satisfies the study criteria, including one cohort study and three RCTs [8, 21, 22, 23, 24].
Baseline Study Characteristics
Four eligible studies included 271 patients: 141 in the surgical arm and 130 in the non-surgical arm. The weighted mean age of patients was 43.25 years (Range: 21 to 71 years) with 43.5 years in the surgical arm and 43 years in the non- surgical arm. This review included 117 women patients. Table 1 describes the baseline characteristics of all the eligible studies.
| Reference Authors | Country | study period | study design | sample size (S/ NS) | Treatment modalities | Sex (F/M) | Age (mean± S.D) | AO type: A/B/C | Average follow up (month) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgical | Non- surgical | Surgical | Non- surgical | Surgical | Non- surgical | Surgical | Non- surgical | ||||||
| Kumar, et al.[23] | India | 2012- 2014 | RCT | 20/20 | plate | Splint | May-15 | 14-Jun | 38 ± 16 | 33 ± 11 | 20/0/0 | 20/0/0 | 6 |
| Matsunaga, et al.[8] | Brazil | 2012- 2015 | RCT | 58/52 | plate | Brace | 23/35 | 14/38 | 37 ± 15 | 40 ± 17 | 38/15/3 | 28/17/6 | 12 |
| Romo,et al. [24] | Finland | 2012- 2019 | RCT | 38/44 | plate | Brace | 18/20 | 20/24 | 49.6 ± 18.2 | 48.4 ± 16.2 | 34/4/0 | 36/7/01 | 12 |
| Hendy, et al. [22] | USA | 2007- 2017 | cohort study | 25/14 | Plate/ nail | Brace | 16-Sep | 07-Jul | 53.6 ± 13.8 | 51.3 ± 19.2 | 12-06- 2007 | 08-02- 2004 | 6 |
Table 1: Baseline characteristics of included studies.
The three RCTs investigated 232 patients, including 116 patients with non-surgical treatment. The weight means average years of the patients in the surgical and non- surgical group were 41.3 years (range: 22-68 years) and 41.9 years (Range: 22-71 years), respectively. All the surgical interventions used plate fixation [8, 23, 24]. As a non-surgical approach, one study used splint (27), and the other two studies used brace approach [8, 24].
The cohort observational study included 39 patients with a mean age of 52.7 years. Non-surgery includes brace approach in 14 patients, and surgical intervention either used nail or plate in 25 patients [22].
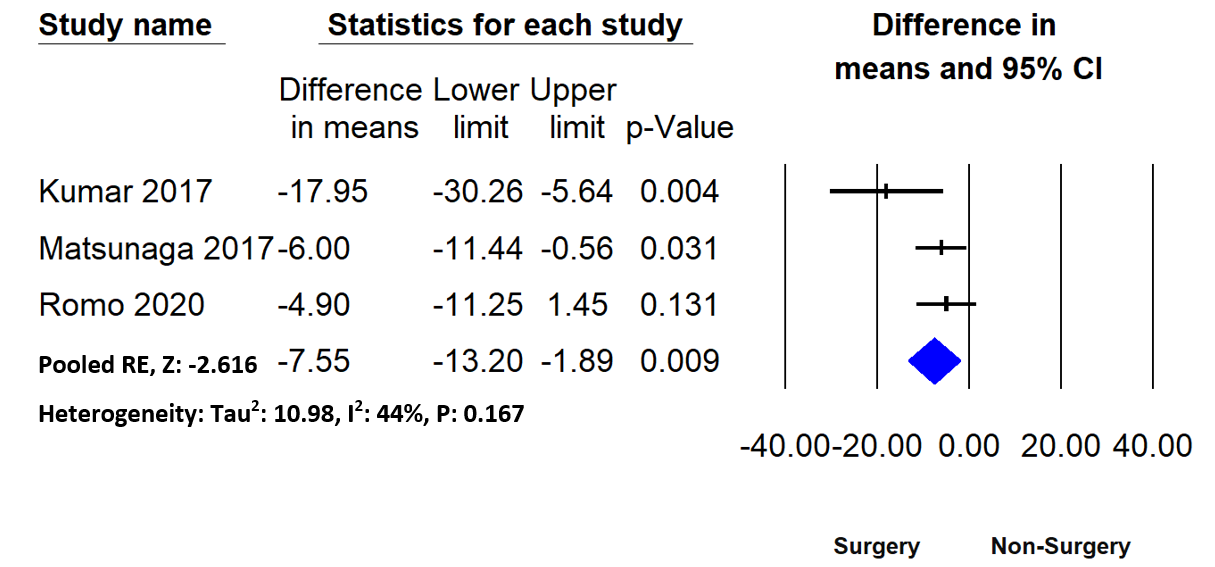
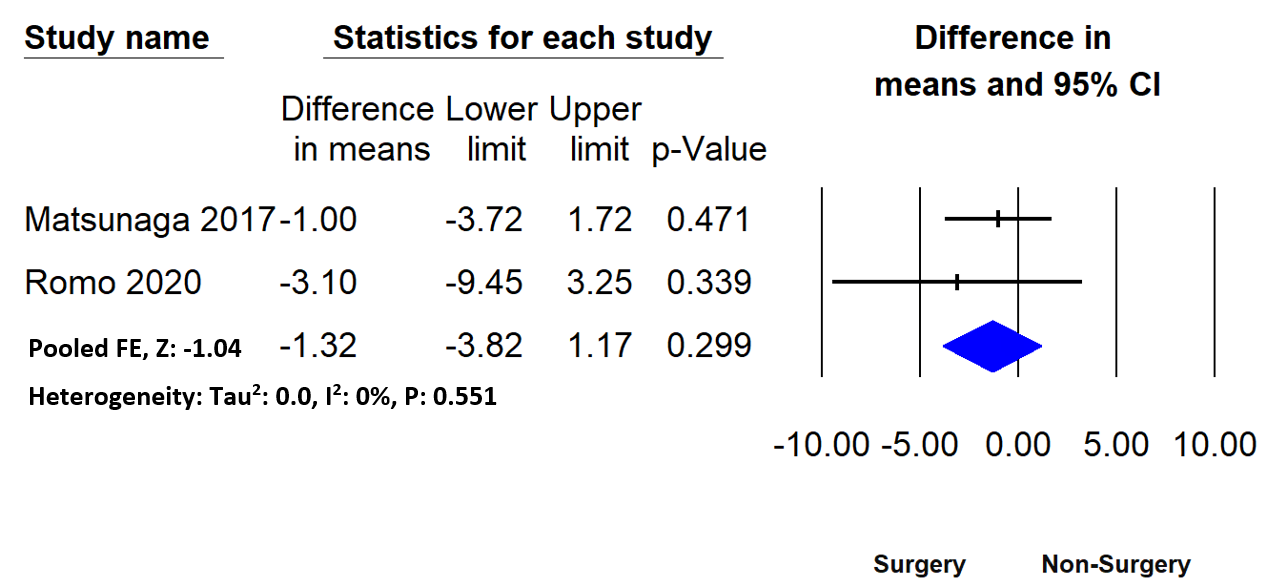
The Measure of Primary Outcomes: DASH: All the 3 RCTs measured DASH [8, 23, 24]. The overall pooled effects demonstrated that surgery was associated with a significant DASH improvement than non-surgery at six months (M.D: -7.5 [-13.20, -1.89], P: 0.009) I2:44%), (Figure 2). However, the overall DASH effects at 12 months (Figure 3) revealed no statistically significant difference between the two groups (M.D: -1.32 [-3.82, 1.17], p:0.29, I2: 0%).
Conclusion of Eligible Studies
One RCT demonstrated statistically significant DASH benefits, lesser deformity, and lower non-union rate in six months following the surgical over non-surgical intervention. However, no significant difference was observed in pain level, SF-36, and constant-Murley score between surgical and non-surgical groups [8]. Similarly, Kumar et al. reported comparable significant functional DASH benefits among participants in the surgery group than functional bracing group [23]. However, Ramo, et al. failed to report any functional benefits between surgical and non- surgical approaches [24]. Hendy, et al. reported no significant advantage of patients for earlier return to work after surgical management of HSF [22].
Meta-Analysis
Mean Constant Murley Score
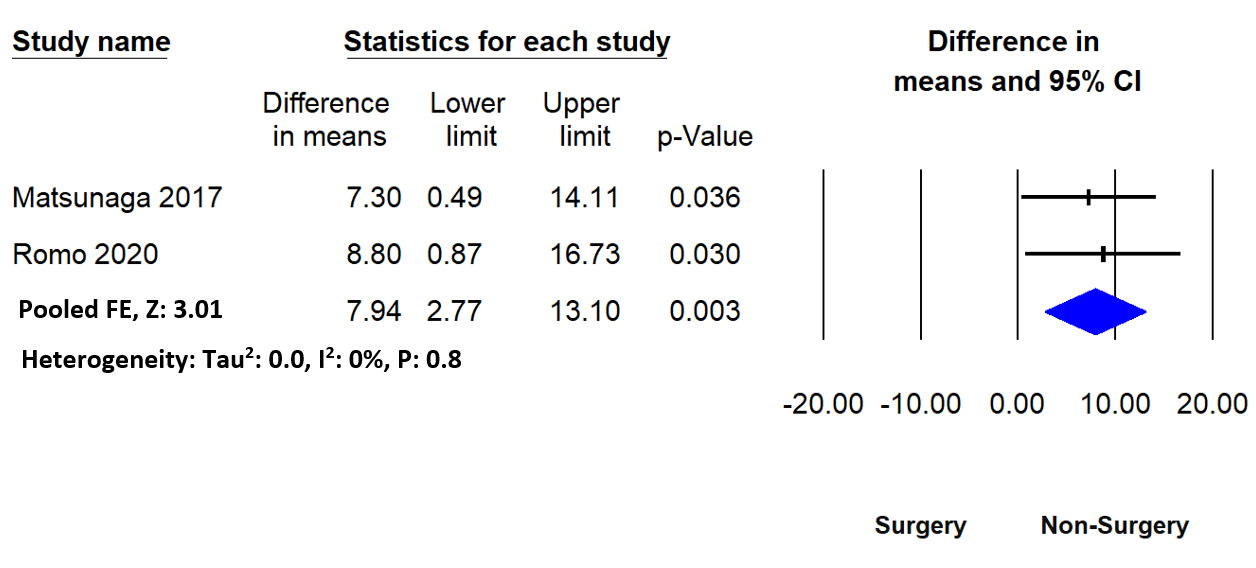
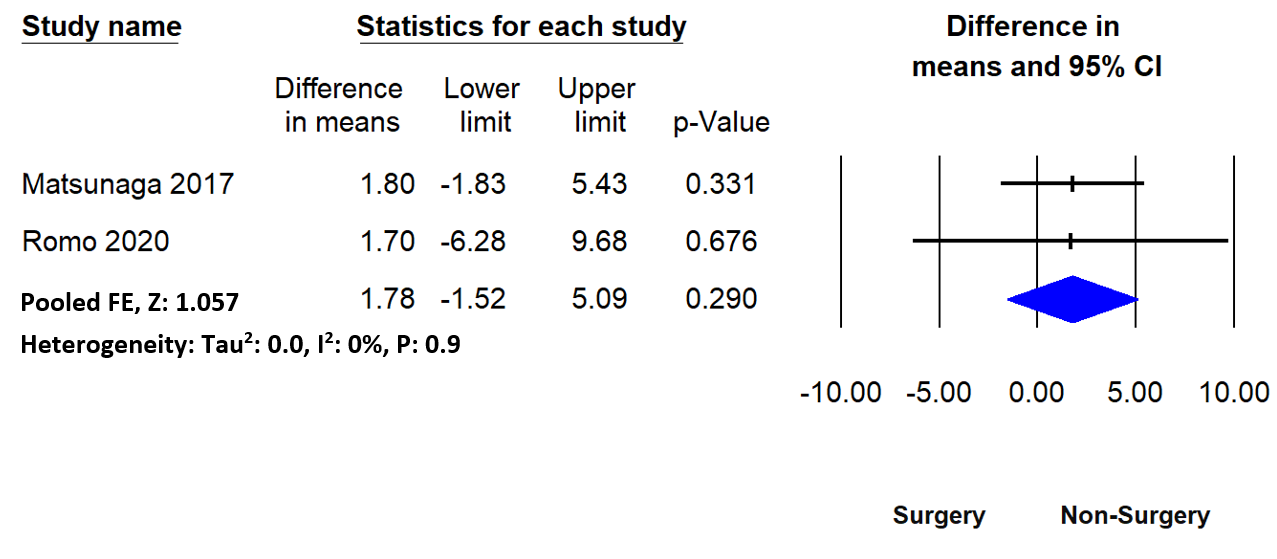
Only two RCTs assessed mean constant Murley score [8, 24]. The overall mean constant Murley score favoured non-surgical intervention over surgical therapy at six (M.D: 7.945[2.77,13.10], P: 0.003) I2: 0%) and 12 months (M.D: 1.78 [-1.52, 5.09], P: 0.29, I2: 0%), (Figures 4,5).
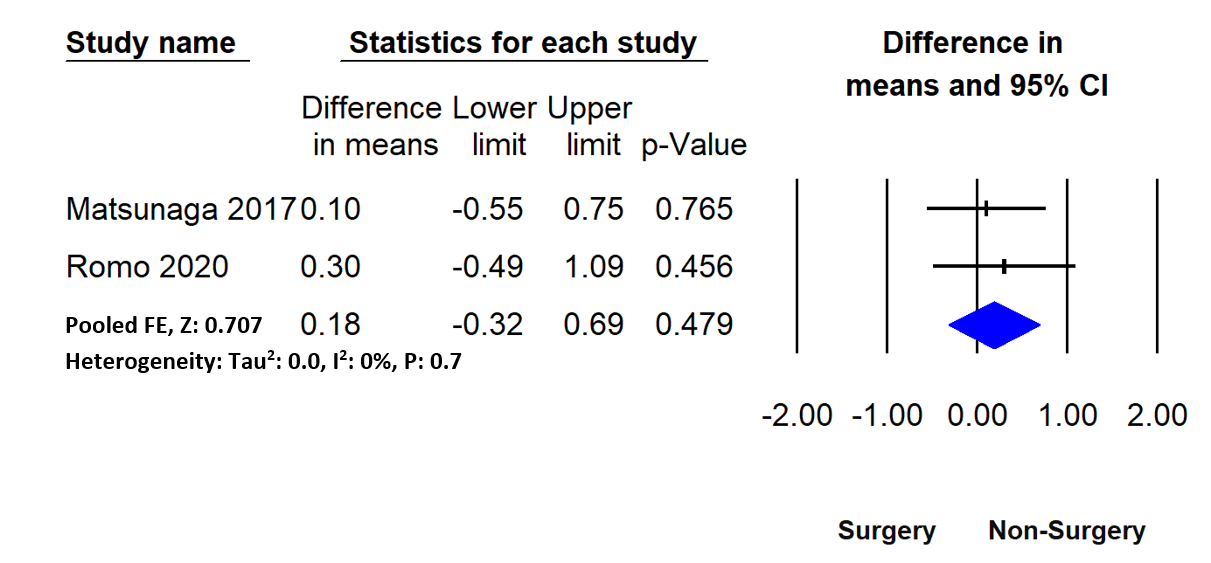
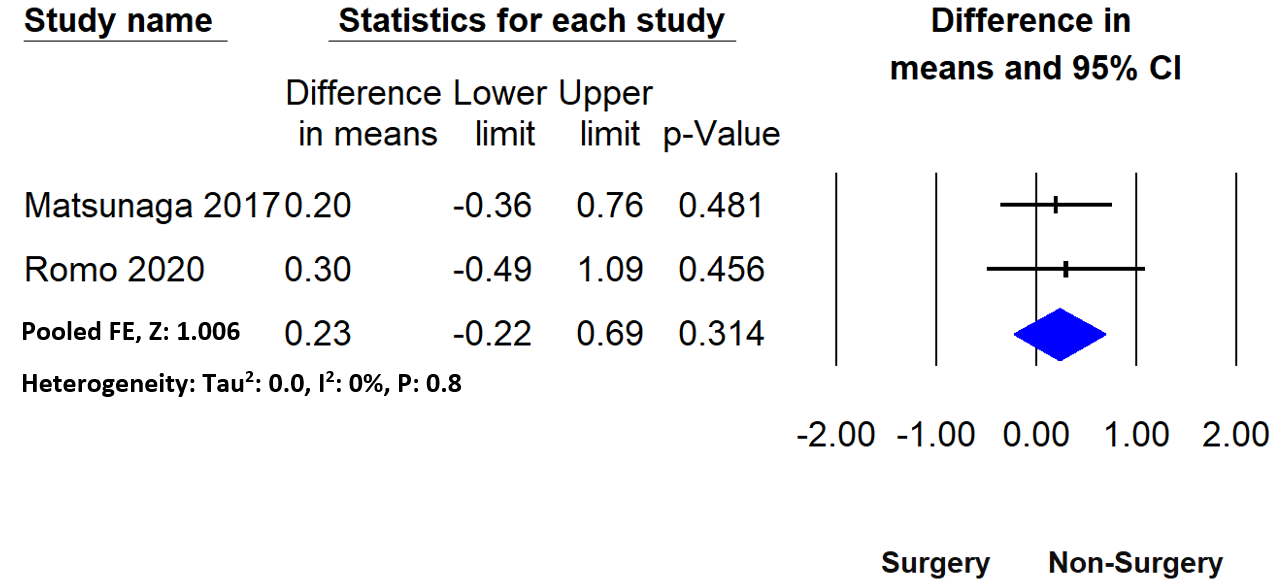
Matsunaga, et al. and Romo, et al. assessed pain intensity using the VAS scale [8, 24]. However, these studies and their pooled overall effects failed to demonstrate a statistically significant difference between surgical and non-surgical intervention at six (M.D: 0.18 [-0.32, 0.69], p: 0.479, I2:0%) and 12 months (M.D: 0.23, [-0.22, 0.69], p: 0.314, I2: 0%) (Figures 6,7).
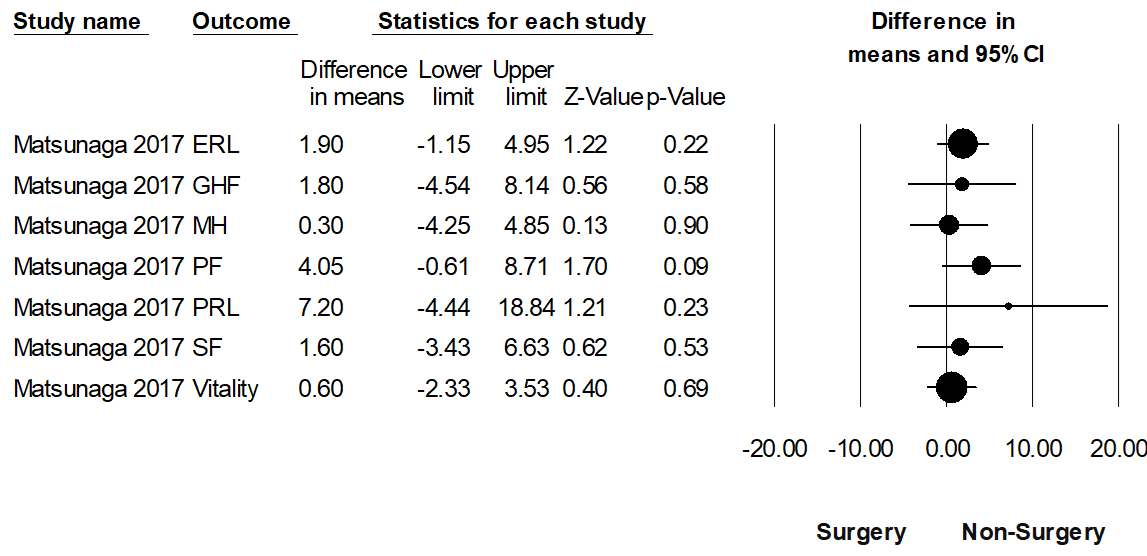
Only Matsunaga, et al. reported SF-36 related outcomes [8]. However, there was no statistical difference of SF- 36 related outcomes between surgical and non-surgical intervention, (Figure 8).
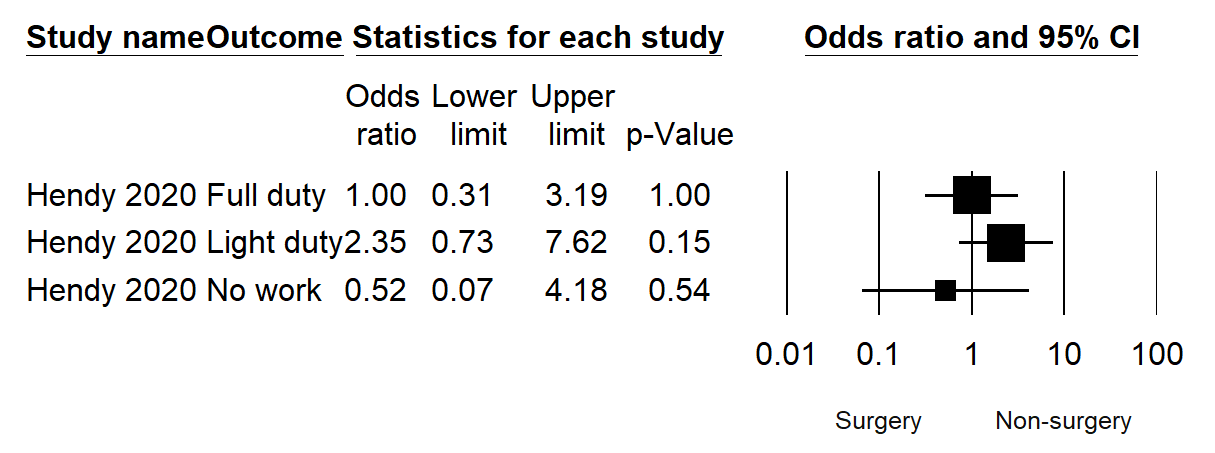
One observational study reported work-related outcomes [22]. However, among the patients with surgical vs. non-surgical treatments for HSFs, there was no significant difference in returning to work on full duty, light duty, or never returning to work (Figure 9).
Risk of Bias in the eligible studies
All 3 RCTs demonstrated low ROB across all domains (Table 2), while cohort studies had a moderate ROB (Table 3) at level 2 evidence. The cohort had a confounding bias as the choice of therapy was based on AO classification, surgeons’ preference, and patients’ pre-fracture health status. In addition, most studies had stratified their outcome based on age, gender, BMI, and fracture cause [8, 23, 24]. All RCTs had a detailed explanation of selection, randomisation of patients, and analysis methods. Nevertheless, these studies reported low value for missing data and degree of deviation from planned intervention.
| Randomisation | Deviation from planned intervention | Missing outcome data | Outcome measurement | Selection of reported outcome | |
|---|---|---|---|---|---|
| Kumar et al, 2017[23] | Low | Low | low | moderate | low |
| Matsunaga et al, 2017[8] | low | moderate | low | low | low |
| Romo et al, 2020[24] | Low | Low | low | low | low |
Table 2: Risk of bias assessment of RCT studies based on Cochrane library tool.
| Patient selection | Intervention classification | Deviation from intent intervention | Missing data | Outcome measurement | Results selection | Confounding | |
|---|---|---|---|---|---|---|---|
| Hendy et al, 2020[22] | moderate | Low | moderate | moderate | low | low | serious |
Table 3: Risk of bias assessment using ROBINS-I.
Discussion
Our study involving one cohort study and three RCTs demonstrate no significant evidence on the patient-related outcome (except DASH and mean constant Murley score at six months) and return to work between surgical and non- surgical interventions. Our meta-analysis demonstrates significantly better DASH improvement in patients managed surgically than non-surgical intervention at six months. Conversely, this study also demonstrated a better mean constant Murley score in the HSF patients with non-surgical approach than surgical procedure. This is the first meta- analysis with three RCTs and one cohort study evaluating patient-related outcomes and return to work in HSF patients managed surgically or non-surgically.
Van de Wall BJM et al. had evaluated the DASH score of two RCTs at six months [8, 23, 25]. Our finding was in converse with Van de Wall BJM et al., reporting no significant difference in DASH score between surgical and non-surgical therapy (M.D:10.7 [-0.7, 22.2], I2: 68%)[25]. Matsunaga FT, et al. reported no significant difference in VAS pain, constant Murley, or various components of SF-36 between surgical and non-surgical groups [8].
In post-operative rehabilitation, the patients with HSF treated either surgically or non-surgically were not allowed to rotate hands beyond 90° for the first six weeks following treatment. The potential benefits from the surgical intervention of HSF could be lost if both interventional groups had similar post-operative rehabilitation [8].
Therefore, future studies should measure patient- reported outcomes and allow early mobilization at the same time point independent of the type of treatment. Van Middendorp et al. reported a considerable significance of surgerical management in constant Murley score in six weeks when combined strength and range of motion. Middendorp et al., also stated surgically managed patients had earlier return to work and daily activities than non-surgical managed patients [17]. A similar outcome might be expected if we compare the HSF to the existing literature of clavicle injuries that demonstrated faster recovery in the surgical group as reported in 2 RCTs assessing clavicle injuries [26, 27].
Only one study investigated the return to work-related outcomes. Hendy et al. reported no significant difference in return to heavy or light duty between non-surgical and surgical management of workers with HSF receiving compensation [22]. Van Middendorp, et al. compared work- related outcomes in surgical and non-surgical management of 47 patients with humeral diaphysis fractures. They also reported no significant difference in return to work even at six, 12, and 52 weeks [17]. Koch, et al. found that the patients with HSF managed with a functional brace required an average of 3 months for returning to work [28]. Our study demonstrated a similar outcome as Shields et al., who reported no significant difference in return to work in clavicle fracture patients managed non-surgically vs. surgically by analysing national worker compensation [29]. Recent systematic reviews and meta-analyses demonstrate satisfactory surgical and non-surgical outcomes among patients with bone fractures. Surgical therapy revealed lesser non-union risk reintervention than non-surgical therapy of HSF. Moreover, surgical therapy has a similar radial nerve palsy rate with the additional surgery-related risk [15].
Limitations
This study has several potential limitations. This systematic review was limited to the English language and may have excluded articles published in other languages. We included cohort studies, which might have selection and recall bias. There was a significant divergence of surgical or non-surgical technique, post-rehabilitation technique, and follow-up period among different studies. These studies also demonstrated a non-uniformity in reporting fracture types, clinical and functional outcomes. Most of the studies had small sample size. Our meta-analysis assessed the patient- reported functional outcome difference between surgical and non-surgical approaches, irrespective of surgical methods (like plate, nail, or minimally invasive techniques). Also, we did not consider the degree of fracture for estimating the pooled effect size.
Conclusion
Altogether, this review supports orthopaedic surgeons who frequently consider the surgical and non-surgical approach in managing HSF. This systematic review provides a satisfactory outcome in both surgical and non-surgical groups. Patients treated for HSF by surgical management favour improved DASH outcomes than non-surgical management. However, non-surgical intervention favoured patient-related outcomes like mean constant Murley, VAS, and SF-36 over surgical intervention in treating HSF. Further, the return to work following surgical vs. non-surgical management of HSF remained inconclusive.
References
-
Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: A review. Injury 37(8): 691-697.
-
Ekholm R, Adami J, Tidermark J, Hansson K, Törnkvist H, et al. (2006) Fractures of the shaft of the humerus. The Journal of Bone and Joint Surgery. British volume 88- B(11): 1469-1473.
-
Tsai CH, Fong YC, Chen YH, Hsu CJ, Chang CH, et al. (2009) The epidemiology of traumatic humeral shaft fractures in Taiwan. Int Orthop 33(2): 463-467.
-
Kim SH, Szabo RM, Marder RA (2012) Epidemiology of humerus fractures in the United States: nationwide emergency department sample, 2008. Arthritis Care Res (Hoboken) 64(3): 407-414.
-
Kocialkowski C, Sheridan B (2021) Humeral shaft fractures: how effective really is functional bracing? Shoulder Elbow 13(6): 620-626.
-
Papasoulis E, Drosos GI, Ververidis AN, Verettas DA (2010) Functional bracing of humeral shaft fractures. A review of clinical studies. Injury 41(7): 21-27.
-
Denard A Jr, Richards JE, Obremskey WT, Tucker MC, Floyd M, et al. (2010) Outcome of nonoperative vs operative treatment of humeral shaft fractures: a retrospective study of 213 patients. Orthopedics 33(8).
-
Matsunaga FT, Tamaoki MJ, Matsumoto MH, Netto NA, Faloppa F, et al. (2017) Minimally Invasive Osteosynthesis with a Bridge Plate Versus a Functional Brace for Humeral Shaft Fractures: A Randomized Controlled Trial. J Bone Joint Surg Am 99(7): 583-592.
-
Schoch BS, Padegimas EM, Maltenfort M, Krieg J, Namdari S, et al. (2017) Humeral shaft fractures: national trends in management. J Orthop Traumatol 18(3): 259-263.
-
Bae SW (2021) Effect of professional certification on employees’ return-to-work rate after occupational injuries in Korea: focusing on vulnerable groups. Environ Health Prev Med 26(1): 6.
-
Stewart Williams J, Kowal P, Hestekin H, O Driscoll T, Peltzer K, et al. (2015) Prevalence, risk factors and disability associated with fall-related injury in older adults in low- and middle-incomecountries: results from the WHO Study on global AGEing and adult health (SAGE). BMC Med 13: 147.
-
Sarmiento A, Zagorski JB, Zych GA, Latta LL, Capps CA, et al. (2000) Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 82(4): 478-486.
-
Ali E, Griffiths D, Obi N, Tytherleigh-Strong G, Van Rensburg L, et al. (2015) Nonoperative treatment of humeral shaft fractures revisited. J Shoulder Elbow Surg 24(2): 210-214.
-
Rutgers M, Ring D (2006) Treatment of diaphyseal fractures of the humerus using a functional brace. J Orthop Trauma 20(9): 597-601.
-
Sargeant HW, Farrow L, Barker S, Kumar K (2020) Operative versus non-operative treatment of humeral shaft fractures: A systematic review. Shoulder Elbow 12(4): 229-242.
-
Mahabier KC, Vogels LM, Punt BJ, Roukema GR, Patka P, et al. (2013) Humeral shaft fractures: retrospective results of non-operative and operative treatment of 186 patients. Injury 44(4): 427-430.
-
Van Middendorp JJ, Kazacsay F, Lichtenhahn P, Renner N, Babst R, et al. (2011a) Outcomes following operative and non-operative management of humeral midshaft fractures: a prospective, observational cohort study of 47 patients. Eur J Trauma Emerg Surg 37(3): 287-296.
-
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, et al. (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 350: 7647.
-
Armijo Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG, et al. (2012) Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: methodological research. J Eval Clin Pract 18(1): 12-18.
-
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, et al. (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355: 4919.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7): e1000097.
-
Hendy BA, Zmistowski B, Wells Z, Abboud JA, Namdari S, et al. (2020) Humeral Shaft Fractures: Surgical versus Nonsurgical Management in Workers’ Compensation. Arch Bone Jt Surg 8(6): 668-674.
-
Kumar S, Shanmugam N, Kumar S, Ramanusan K (2017) Comparison between operative and non operative treatment of fracture shaft of humerus: an outcome analysis. International Journal of Research in Orthopaedics 3(3).
-
Rämö L, Sumrein BO, Lepola V, Lähdeoja T, Ranstam J, et al. (2020) Effect of Surgery vs Functional Bracing on Functional Outcome Among Patients With Closed Displaced Humeral Shaft Fractures: The FISH Randomized Clinical Trial. JAMA 323(18): 1792-1801.
-
van de Wall BJM, Ochen Y, Beeres FJP, Babst R, Link BC, et al. (2020) Conservative vs. operative treatment for humeral shaft fractures: a meta-analysis and systematic review of randomized clinical trials and observational studies. J Shoulder Elbow Surg 29(7): 1493-1504.
-
Ahrens PM, Garlick NI, Barber J, Tims EM (2017) The Clavicle Trial: A Multicenter Randomized Controlled Trial Comparing Operative with Nonoperative Treatment of Displaced Midshaft Clavicle Fractures. J Bone Joint Surg Am 99(16): 1345-1354.
-
Qvist AH, Vaesel MT, Jensen CM, Jensen SL (2018) Plate fixation compared with nonoperative treatment of displaced midshaft clavicular fractures: a randomized clinical trial. Bone Joint J 100-B(10): 1385-1391.
-
Koch PP, Gross DF, Gerber C (2002) The results of functional (Sarmiento) bracing of humeral shaft fractures. J Shoulder Elbow Surg 11(2): 143-150.
-
Shields E, Thirukumaran C, Thorsness R, Noyes K, Voloshin I, et al. (2016) Patient factors influencing return to work and cumulative financial claims after clavicle fractures in workers’ compensation cases. J Shoulder Elbow Surg 25(7): 1115-1121.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results