Total Hip Arthroplasty in Extensive Venous Malformations An Experience of Four Cases
Background: Extensive venous malformation (VM) (Klippel-Trenaunay syndrome, KTS) and associated degenerative joint disease of the hip is a rare condition. The difficulty of total hip replacement (THR) depends on tissue involvement around the joint, with the risk of severe blood loss. To evaluate the feasibility and outcome of hip replacement in this disease. Methods: Between 2010 and 2020, 4 patients with extensive VM of the limb and degenerative joint disease had a total hip replacement. Investigations included X-ray exams, T2 MRI with fat saturation, and hematologic tests. The main outcome endpoints of the study were success of hip replacement, postoperative complications and quality of life. Results: Four patients underwent THR. Le sex ratio was (3 males, 1 female) with a median age of 37 years (range 27-55). All were symptomatic, with worsening hip pain and use of a mechanical aid. MRI identified VM in the muscles and cellular space of the buttock. The choice of surgical approach was anterior in three patients, and lateral in one. Mean blood loss was 1500mL. Surgery was completed by peroperative sclerotherapy to reduce blood loss (3 patients). The median follow-up time was 82 months (range 12- 120). There were no postoperative complications. At 6 months, three patients were walking with normal gait, and one was using an orthopedic walker after knee arthrodesis. There was no reoperation during the follow-up. All patients returned to their professional activities. Conclusion: The difficulty of total hip replacement depends on the extent of involved soft tissue around the hip area. The choice of surgical approach, surgical skill in vascular and orthopedic procedures and per-operative sclerotherapy permit to reduce surgical risk.
Introduction
Extensive venous malformation of the limb (Klippel Trenaunay syndrome KTS) with degenerative joint disease is an unusual condition. Secondary hip osteoarthritis is one of the potential causes of pain in patients with extensive venous malformation (VM) [1, 2]. There are several underlying causes including: leg-length discrepancy, degenerative joint changes in the knee, painful weight support, or previous dystrophy of the hip. Venous malformation can also cause recurrent painful episodes due to thrombophlebitis in the involved tissue.
Severe vascular changes around the buttock and upper thigh expose to the risk of major bleeding [3, 4, 5, 6], the choice of surgical approach should be made based on the involved tissue by the VM. Peroperative sclerotherapy of soft tissue reduce the blood loss and provides a safe space for arthroplasty.
Another particularity of extensive VM is related hematologic disorders [7]. Hematologic data evaluate the potential increased risk of hemorrhagic events due to localized intravascular coagulopathy (LIC) which needs to be treated preoperatively.
To highlight the benefit of targeted investigations and the surgical strategy with sclerotherapy, we report data collected on lesions located in the same area.
The aim of the study was to demonstrate the low risks of performing THR with a targeted approach, and perioperative sclerotherapy.
Material and Methods
Study Design
We retrospectively reviewed 4 consecutive patients who had a total hip replacement (THR) in our center between 2010-2020 and who had concomitant extensive VM. A single multidisciplinary team selected the patients and a surgical team of orthopedic and vascular surgeons performed the surgery.
All patients or guardian(s) received oral and written information, and all signed a statement regarding publication consent form concerning their case and images. For this cohort, the review of the data was approved by the ethics committee of our institution.
Data Collection
Data collected from each patient’s medical record consisted of the medical history, clinical findings, radiographs, magnetic resonance imaging (MRI) reports, and hematologic tests results. Further information regarding surgical procedures, intraoperative transfusions, postoperative complications, and duration of surgery, was collected.
Institutional scores were determined according to pain, quality of gait, physical activity and educational and/ or professional activity. Function (pain, mobility, gait) was evaluated by the PMA score [8] and collected preoperatively, six months after surgery, and at the final follow-up. Professional activity was evaluated: (1: full-time work, 2: part-time work, 3: sick leave, 4: retired). Indications for secondary procedures were separated into orthopedic and vascular procedures.
Clinical Protocol
Patients were selected if they had significant symptoms with degenerative changes in the joint. All patients had digital radiographs, Ultrasound-Doppler (US), an MRI, and hematologic tests. A US examination was performed to detect deep venous anomalies. A T2 MRI with fat saturation resulted in two values: 1) a diagnostic value locating the tissue involvement by the VM (cellular space, muscles) and 2) a strategic value allowing an assessment of the best surgical approach. Hematologic results detected any potential increased risk of hemorrhagic events (abnormal D-dimers, fibrinogen, and platelets). Low molecular weight heparin (LMWH) was administrated if necessary to correct significant abnormalities.
Arteriography and arterial embolization were never indicated in venous malformations (or KTS).
Case Study
Case 1
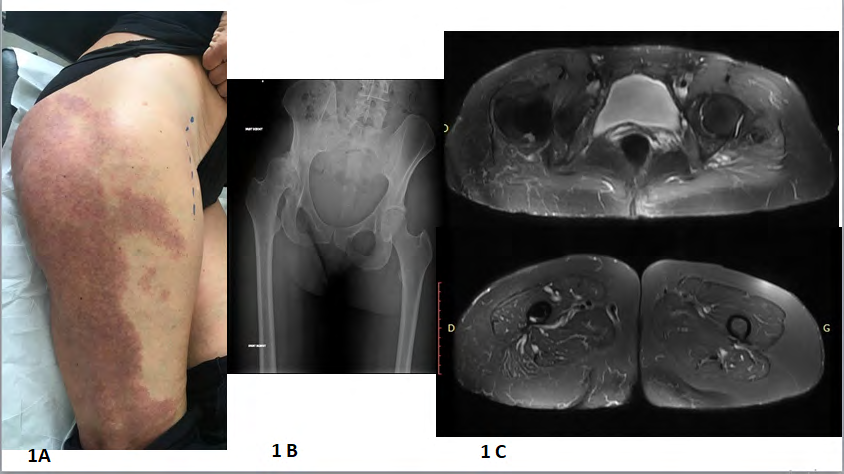
A 50 years- old female, in law practice, had extensive VM of the right limb associated with a leg length discrepancy of 4cm, and a slight limp starting 4 years before consultation. During the pre-operative period, she walked with a moderate limb using one crutch. Radiographs showed hip degenerative arthropathy and pelvis asymmetry. (Figure 1) The VM was related to a superficial port wine-stain and agenesia of the popliteal vein without deep tissue involvement. The hematologic exam was normal. A THR was done by an anterior approach with no bleeding problem.
Case 2
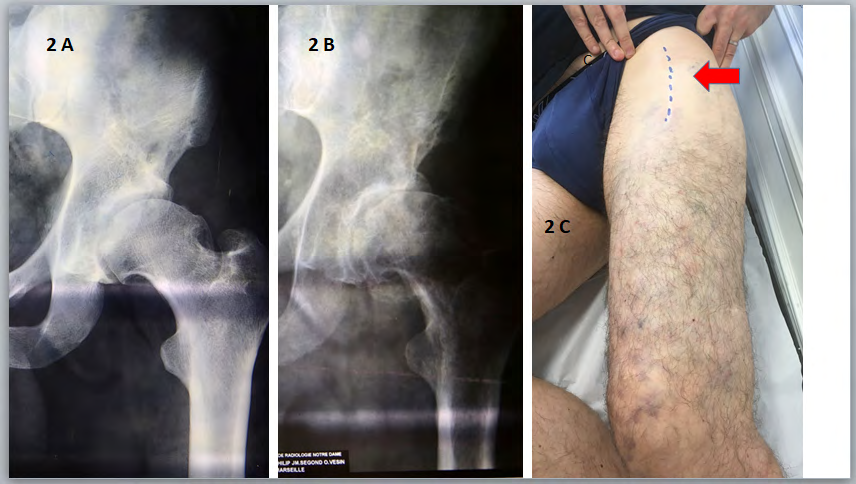
A 37 years- old male, commercial agent, had extensive VM of the left limb with superficial and deep tissue involvement (buttock, thigh, leg and foot). Moderate pain started 2 years before consultation, then became marked pain with activity limitation and gait assisted with one crutch. Radiographs showed bilateral dysplasia of the hip with degenerative arthritis in the left side (Figure 2). The hematologic exam revealed significantly increased of D-dimers. A THR using an anterior approach was done with per-operative sclerotherapy of fascia lata and cellular space.
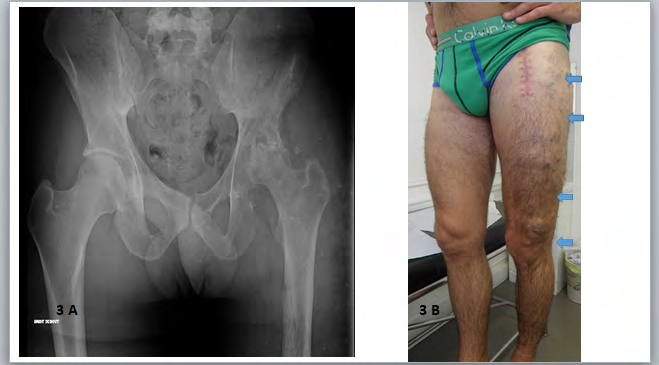
Case 3
A 27 years-old male, engineer, presented with extensive VM of the left limb. At age 12, he had a resection of an intra articular VM of left knee. He was asymptomatic for 15 years, then after a moderate trauma to the hip, he had marked pain and was totally disabled, walking with 2 crutches. Radiographs showed: a degenerative femoral head, MRI showed deep tissue VM involvement (buttock, thigh, leg) (Figure 3). Hematologic exams revealed a high level of D-dimers and a low fibrinogen level. He needed preoperative treatment by LMWH. A THR was performed using an anterior approach with per-operative sclerotherapy. Case 4: A 30 years-old male, bank assistant, presented with extensive VM of the left limb (Figure 4). At age 11, he has a resection of an intra articular VM of the knee and arthrodesis due to significant cartilaginous lesions. Orthosis was well tolerated (knee in extension, leg- length discrepancy of 4 cm). Moderate pain in the hip started 2 years before consultation, followed by activity limitation and walking assisted with one crutch. Radiographs revealed: degenerative femoral head, MRI showed a significant deep VM in the buttock, thigh, leg and foot. Hematologic exams showed: high level of D-dimers, a decreased fibrinogen level of 1g/L necessitated preoperative LMWH to stabilize the disorder. A THR was performed, a lateral approach through the VM was used to obtain a large approach to the joint.

Results
Clinical findings
Four patients underwent surgery between 2011 and 2020 (1 female, 3 males and median age 37 (27-54) years). Patients were symptomatic; 1 had acute symptoms after a minor hip trauma, 3 had chronic pain that could occur at any -time, which increased with walking and necessitated mechanical aid.
All had extensive VM of the lower limb since childhood. Three patients had previously undergone procedures on vascular components: 2 for intra-articular VM of the knee (one arthrodesis due to extensive cartilaginous lesions), and 3 for resection of varicose veins.
The clinical exam provided the following information: 1) orthopedic exams: showed that all patients had severe limitation of hip motion, 2 had a leg-length discrepancy of 4 cm, and none had previous THR attempt; and 2) vascular exams showed that three patients had extensive VM of the limb since childhood with tissue hypertrophy of the lower limb and varicose veins.
Non-invasive investigations
Radiographs of the pelvis and thigh revealed: avascular necrosis of the femoral head for one patient. Three patients had secondary osteoarthritis with joint space narrowing (one had previous femoral head dystrophy). One patient had abnormal morphology of the femoral shaft secondary to diffuse tissue involvement in the thigh (Figure 5).

MRI evaluated the extent of tissue involvement of the VM. These findings allowed us to distinguish three morphological aspects: 1) superficial VM (port-wine stain) (1 patient), 2) tissue involvement was in the lateral and posterior parts of the buttock permitting an anterior approach (3 patients) (Figure 6), and 3) extensive VM around the hip where the lateral approach permitted a better exposition of the joint (Figure 7). Three of the patients had intramuscular VM in the anterior and posterior compartments of the thigh.
Hematologic tests revealed significant abnormalities in 2 patients. All had elevated D-dimers levels (20 x normal), two had a low level of fibrinogen consequence of active intravascular coagulopathy. For them, the fibrinogen level was stabilized with LWMH during the preoperative period.
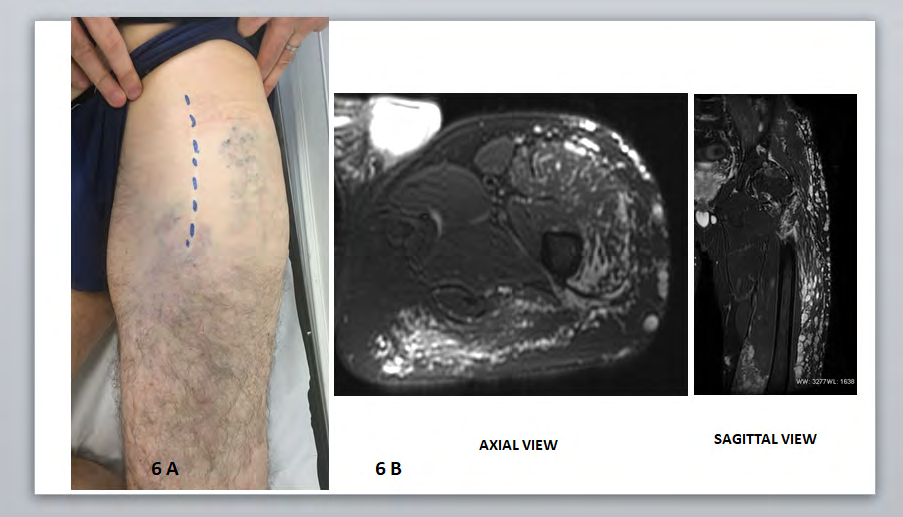
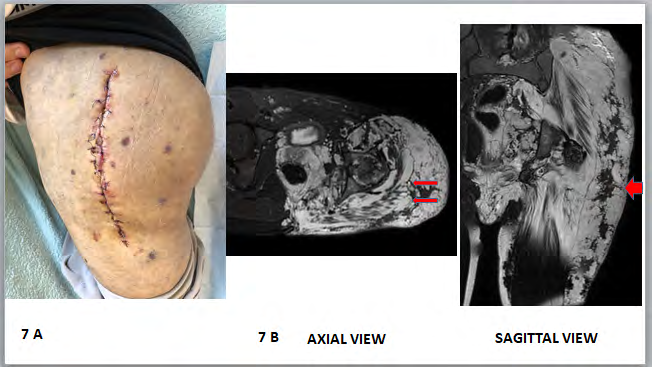
Figure 7: Significant tissue involvement around the hip. 7A: postoperative view of the lateral approach, no hematoma, no late healing 7B; Preoperative T2 MRI: axial view: extensive involvement of deep tissue around the joint (arrow). Hemostasis by sclerotherapysagittal view: significant VM in the subcutaneous tissue over the fascia lata muscle (arrow). Hemostasis by running sutures.
Operative surgical treatment by vascular and orthopedic practitioners; The surgical approaches were anterior in 3 patients, and lateral in 1. The VM in the subcutaneous layer was controlled with a continuous running suture. In the anterior approach, hemostasis was obtained with suture of varicose veins over the fascia-lata muscle and cellular space, sclerotherapy was not always required. Due to diffuse tissue involvement, the lateral approach needed per-operative sclerotherapy of the involved soft tissue around the joint to avoid severe blood loss.
In these 4 cases, we noted the absence of VM in the capsular plane, and no intraosseous VM of the hip. They had acetabular and femoral components without technical difficulties. The quality of the bone was always excellent. Mean blood loss was 1500mL (range 500-2500). A cell-saver device was always used. Three patients needed intraoperative transfusions (2 to 4 units). One needed a vasopressor for a short time at the end of the procedure. The median duration of surgery was 3 hours (range2-4).
Post-operative course: No hematomas, delayed healing or reoperation were observed. Hematologic tests were normalized at 2 and 4 days after the procedure. Patients were discharged home after 5 days. Professional activities were interrupted for one month. Between the post-operative period and the last follow-up, there were no orthopedic events, but 2 patients had vascular procedures on symptomatic lesions. At the last follow-up (median 82 months (range 12-120)), all patients reported no orthopedic events. Three had normal gait, and one was using an orthopedic walker (arthrodesis of knee, leg-length discrepancy). From the vascular stand point, none of the patients had symptomatic evolution of the VM and they wore an elastic garment. Hematologic abnormalities were limited to high levels of D-dimers. MRI follow-up showed no evolution of tissue involvement. Post- operative treatment consisted of LMWH for 3 weeks, then an antiplatelet agent for six months.
Quality of life
Four patients reported no residual pain and good hip motion. Three had normal gait without mechanical help. One had functional sequelae due to arthrodesis of the knee. Functional results showed that the mean PMA score increased significantly from 5,75 to 17. (p<0,0001) [8]. All had normal occupational and professional activity.
Discussion
In this report, we present our findings for 4 patients with degenerative arthritis of the hip with concomitant extensive venous malformation (Klippel Trenaunay syndrome) (KTS).
Literature
Four papers have been published related to experience with THR in KTS [3, 4, 5, 6]. Four cases were reported (2 females, 2 males, median age 46years (range 27-50). All had chronic progressive arthropathy of the hip. Two had a previous correction of leg- length discrepancy; one had 2 attempts of THR. Investigations were heterogeneous including:
arteriography (2 patients), MRangiography (1patient), CT scan [1]. Only one patient had hematologic tests which showed an intravascular localized coagulopathy. Three had preoperative procedures: 1 had sclerotherapy of superficial varicose veins, and 2 underwent subcutaneous injection of adrenalin on the operative site. Surgical approaches were anterior [1] lateral [2], or not defined [1]. There was no significant bony bleeding in any reports. One procedure was aborted due to severe bleeding, three were successful. The blood loss was due to significant bleeding from the subcutaneous tissue and soft tissue around the hip.
Our understanding of VM has evolved from an angiographic concept (identification of arterial pedicles) to a tissular concept with identification of targeted involved tissue by MRI. Venous malformation is hyper vascularized tissue with large veins without a true arterio-venous fistula.
Clinical Symptoms and Investigations
Three points must be evaluated: 1) clinical extent of VM on the buttock, 2) the location of involved tissue around the hip, 3) hematologic abnormalities.
The differing extent of VM explains the varying difficulty of the procedure: port-wine stain superficial lesions or hypertrophic tissue with numerous varicose veins associated with deep tissue involvement. Lesions are usually located on the lateral and posterior parts, permitting an anterior approach on healthy skin.
The exact location of the involved tissue is determined by T2 MRI fat saturation showing a specific hypersignal. A CT scan does not allow the precise evaluation of the lesions. Arteriography is never needed, showing a hyper vascularized tissue without arterio-venous shunts. Radiographs identify marked abnormalities of the hip and rarely abnormal morphology of the femoral shaft.
Hematologic disorders are an important point. A high level of D-dimers is always noted in extensive VM [7]. The low level of fibrinogen is more important reflecting phlebothrombosis in the VM. This must be treated preoperatively with LWMH to reduce the intravascular thrombosis (localized intravascular coagulation LIC). The surgical procedure must be scheduled when a normal fibrinogen and platelet levels are achieved with a related decrease in D-dimers.
Therapeutic Procedures
Vascular surgical approach: Preoperative data allows surgeons to choose the safest surgical approach. In our cases, an anterior approach was done on normal skin cover for 3 patients. In these 3 patients, exposition of the joint was close to the involved tissue which needed suture hemostasis and/ or sclerotherapy to reduce blood loss. In one patient, a lateral approach through the VM permitted a better exposition in two steps. First hemostasis of large subcutaneous varicose veins was done by running suture. Second, sclerotherapy was used in the soft tissue, fascia lata and gluteal muscles until the capsular plane were reached.
It was surprising to note that the capsular plane, like the head of the femur and acetabular component was not involved by the VM. Intra-articular VM was not observed.
The agent used for sclerotherapy was heated Horsley’s bone wax [9]. The wax had a meeting point range of 62 to 65°C after which it became a transparent liquid. We used it at this temperature to inject into the component of VM. Within few seconds, it solidified forming a continuous cast which filled the VM. This agent transformed quickly with a high occlusive seal rate. In this location, there is no risk of pulmonary embolism.
Orthopedic procedure: There were no difficulties in the replacement procedure. The proximal femur had normal morphology without abnormal bleeding in the medullary bone. The acetabular component was cemented or uncemented, femoral component was cemented.
Complementary suture hemostasis was needed. Cautery hemostasis is less effective for this disease.
Surgical Indications
Standard practice states that bony surgery should be avoided due to risks of uncontrollable hemorrhage. In spite of our precautions, the mean blood loss was 1500mL which underlines the necessity of using a cell saver device, per- operative transfusions, or vasopressor.
In our center, we proposed a THR for patients with severe symptomatic degenerative osteoarthritis of the hip after careful preoperative planning and consideration of potential complications. This surgery requires a double competence of orthopedic and vascular surgeons.
The choice of surgical approach depends on the involved tissue: 1) an anterior and lateral approach was appropriate with the absence of deep pathologic tissue, 2) an anterior approach is more frequently chosen due to predominantly lateral and posterior pathologic areas, 3) a lateral approach is chosen if there is extensive involvement of tissue around the joint, which permits a large exposition.
This study is limited by its retrospective nature and long period of recruitment. However, it is a homogeneous cohort with the same investigational data and mid- term orthopedic follow-up. Total hip replacement can be a safe treatment for these complex procedures. Sclerotherapy with heated bone wax is a reproductible procedure and will be of use to surgeons encountering such patients.
Conclusion
Total hip replacement for patients with extensive venous malformation is an invasive approach. THR after precise preoperative planning is feasible and relatively safe. THR is a valuable treatment option based on a retrospective single center analysis.
- Conflict of interest; the Authors declare that there is no conflict of interest
- Ethics approval: The review of the data of this cohort was approved by the Ethics commission of our institution.
• Consent for publication: All patients or tutor(s) were provided with oral and written consent; all signed a statement regarding publication consent form concerning their case and images.
• Funding sources: This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
• Table of Content Summary This retrospective single-center study analyzed presentation, management, and outcome of 4 patients underwent THR in extensive venous malformations. This study suggests that total hip replacement with per operative sclerotherapy is safe without significant morbidities.
• Article Highlights Type of research: Single center study, retrospective analysis of prospectively collected registry data, non-randomized cohort. Key findings: THR in extensive VM of the limb with per operative sclerotherapy avoid severe bleeding complications. The lack of intraosseous VM permits conventional orthopedic procedure with good functional result. Take home message: Targeted investigations before surgery: T2 MRI fatsat to evaluate the extent of the involved soft tissue by VM, hematologic tests to identify a coagulation disorder which must be treated preoperatively. Per- operative sclerotherapy by bone wax can prevent severe blood loss.
• Contributor ship CL involved in protocol development and gaining ethical approval, wrote the first draft FT research literature and surgical data EV radiological data, acquisitions and analysis of data PJ review of manuscript AB clinical data, review the manuscript
References
-
Enjolras O, Ciabrini D, Mazoyer E, Laurian C, Herbreteau D (1997) Extensive pure venous malformations in the lower and upper limbs. J Am Acad Dermatology 36(2): 219-225.
-
Lee A, Driscoll D, Glovickki P, Clay R, Shanghnessy W, Stans A (2005) Evaluation and management of pain in patients with Klippel-Trenaunay syndrome, a review. Pediatrics 115(3): 744-749.
-
Mallick A, Weeber AC (2007) An experience of arthroplasty in Klippel-Trenaunay syndrome. Eur J Orthop Surg Traumatol 17(1): 97-99.
-
Willis Owen CA, Cobb JP (2008) Total hip arthroplasty in Klippel-Trenaunay syndrome. Ann R Coll Surg Engl 90(8): 1-3.
-
Garcia Juarez JD, Tohen bienvenu A, Jimenez Cabuto IC, Molina Mendez J (2011) Total hip arthroplasty in Klippel-Trenaunay syndrome: case report and literature review. Acta Ortop Mex 25(2): 126-129.
-
Cirstoiu C, Cretu B, Sandu C, Dorobat B, Neagu A, et al. (2019) Failed attempt of total hip arthroplasty in a patient with Klippel-Trenaunay syndrome. JBJS 9(4): e0.
-
Mazoyer E, Enjolras O, Bisdorff A, Perdu J, Wassef M, et al. (2008) Coagulation disorders in patients with venous malformations of limbs and trunck. Arch Dermatol 144(7): 861-867.
-
Merle D’aubigne R, Postel M (1970) Resultats fonctionnels de la prothèse totale de hanche. Cotation chiffrée de la fonction de la hanche. Rev Chir Orthop 56: 481-486.
-
Mallios A, Laurian C, Houbballah R, Gigou F, Marteau V (2011) Curative treatment of pelvic arteriovenous malformation. An alternative strategy: transvenous intraoperative embolization. Eur J Vasc Endovasc Surg 41(4): 548-553.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results