Panton-Valentine Leucocidin-Positive Staphylococcus Aureus Gonarthritis in a Healthy Adult Leads To Fulminant Sepsis with Multiple Metastatic Soft Tissue Infection and Necessity of Extracorporeal Membrane Oxygenation
Background: Infections with Panton-Valentine leucocidin (PVL) positive Staphylococcus aureus (S. aureus) are often complicated by necrotizing pneumonia, myositis and osteomyelitis. Case Description: We describe a 50 years old, previously healthy male which presented a severe infection with PVL-positive, methicillin- susceptible S. aureus (MSSA) in his left knee after returning from China. He developed a fulminant sepsis with necrotizing pneumonia, acute respiratory distress syndrome (ARDS), acute renal failure and multiple soft tissue abscesses. Extra-corporeal membrane oxygenation (ECMO) was needed for five days. The patient recovered after multiple surgical interventions and long-term antibiotic treatment and eventually returned to work five months after initial admission. Conclusion: While most staphylococcal skin and soft tissue infections (SSTI) show a favorable outcome, SSTI caused by PVLpositive bacteria can lead to fulminant and fatal disease manifestations. Immunocompetent individuals are equally affected as immunocompromised ones. Early suspicion, surgical intervention with debridement and drainage of abscess formations are of key importance in concert with appropriate antibiotic therapy without delay. Imaging should be done to identify clinically silent foci.
Introduction
S. aureus associated skin infections are quite frequent among travelers to the tropical or subtropical area [1, 2]. In many cases S. aureus carries a virulent factor called Panton-Valentine leucocidin (PVL). This bi-component, pore forming cytotoxin is related to a broad spectrum of diseases including skin and soft-tissue infections, severe bone and joint infections, deep-seated abscesses, and life threatening necrotizing pneumonia. Clear evidence, however, is lacking that the PVL influences clinical presentation and outcome [3].
Case Presentation
A 50 years old engineer presented to the emergency room with pain, swelling and redness of his left lower leg. He first suffered from a stiff left knee, body aches and shivering two weeks ago in China. He did not report about any trauma or skin lesion. Since he believed that the complaints were related to a thrombosis, he started to inject Nadroparin s.c.. Because of progressive pain he went to a medical doctor two days later, who performed a knee joint puncture without, to our knowledge, any further treatment. With worsening symptoms including tachycardia, he returned home and went straight to our hospital.
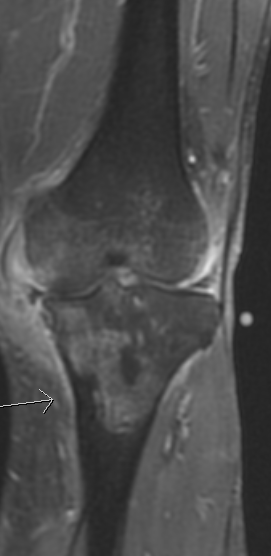
At the emergency room the patient presented a tachycardia of 139/minute and a blood pressure of 93/65 mm Hg. The body temperature was 36.9°C. The left lower leg was severely swollen with limited flexion and large joint effusion of the left knee. Local skin necrosis was present (Figure 1). The patient also suffered from acute kidney failure and a thrombosis of the left popliteal vein proven by ultrasound. The white cell count was 14.6 x 109 L-1, the C-reactive protein 319 mg/l (reference range < 5 mg/l) and the pro-calcitonin 27.23 µg/l (reference range < 0.1 µg/l). The patient’s history was otherwise unremarkable. With a severe SIRS the patient was transferred to the ICU immediately. In agreement with the infectious disease consultants, we started with flucloxacillin i.v., daptomycin, i.v., ciprofloxacin i.v. and later clindamycin i.v.. MRI reveals hints to a septic arthritis of the left knee with abscess formation in the adjoining soft tissue (Figure 2). Arthroscopy, lavage and synovial debridement were done the following day. The microbiology of the intra-articular aspirate demonstrated gram-positive bacteria. At day 3, daptomycin and ciprofloxacin were replaced by Ertapenem and two days later Meropenem for a better coverage of Pseudomonas aeruginosa super infection while flucloxacillin was continued. Endocarditis was excluded by trans- esophageal echocardiography. The eventual microbiology showed MSSA encoding the PVL and thus treatment was continued solely with flucloxacillin for in total 69 days and later changed to ciprofloxacin and rifampicin (Table 1).

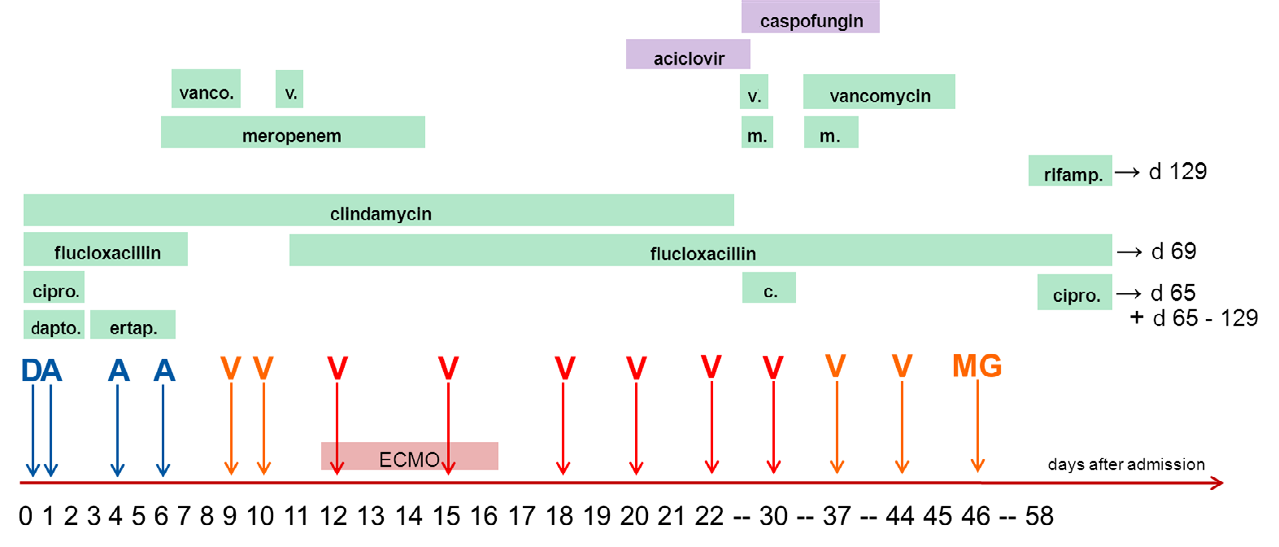
- D: Debridement of the left knee; A: arthroscopy of the left knee; V: negative pressure wound therapy of upper and lower extremities combined with repeated surgical debridement procedures; MG: Wound closure of the left knee with skin graft. cipro.: ciprofloxacin; dapto.: daptomycin; ertap.: ertapenem; rifamp.: rifampicin.
Table 1: Antibiotic and operative treatment after admission to our hospital.
Due to elevated sepsis parameters, another MRI scan of all four extremities was arranged, in which multifocal myogenic abscess formation appeared. Hence, all abscesses underwent open surgical debridement in the theatre followed by a negative pressure wound therapy. During management the patient developed a necrotizing pneumonia with ARDS. However, the cardio-pulmonal situation aggravated in suchlike way that an ECMO therapy for 5 days became necessary.
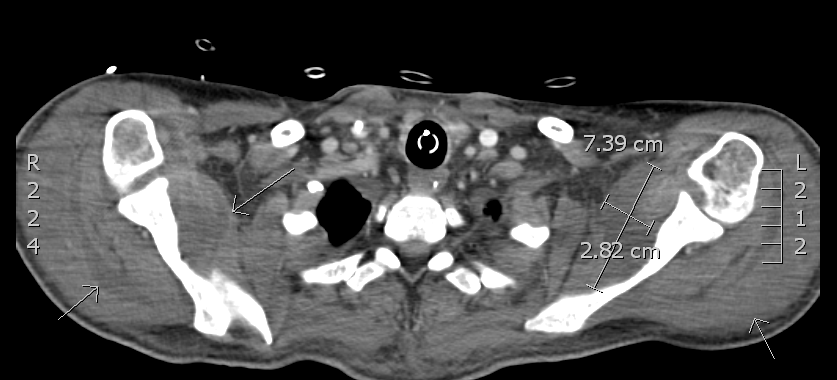
Due to the worsening clinical situation and persisting signs of osteomyelitis in the left tibia shown in the MRI, an amputation of the left lower leg was discussed but nevertheless discarded. There was a necessity for multiple surgical operative revisions on the left knee joint and tibia, thorax, both arms and pelvis because of abscess formations on different locations (Figure 3, Table 2). During further operative and antibiotic treatment, the patient started to incline gradually and wounds could be closed secondarily on several occasions.
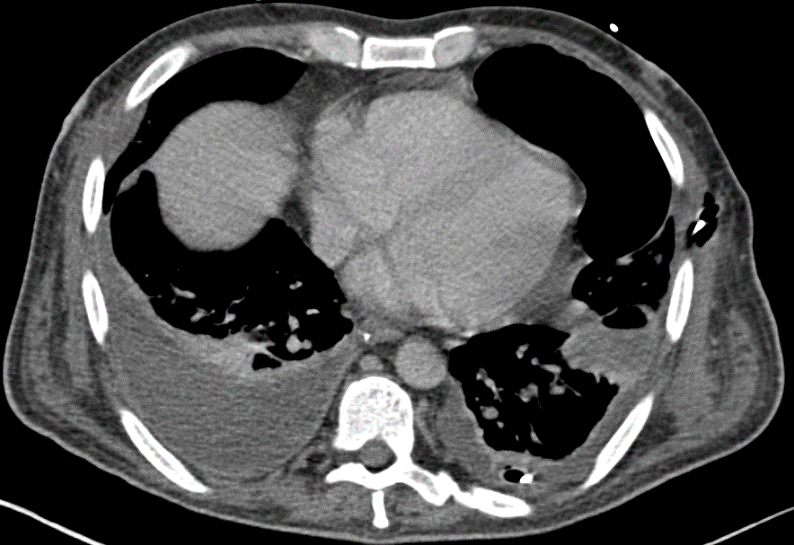
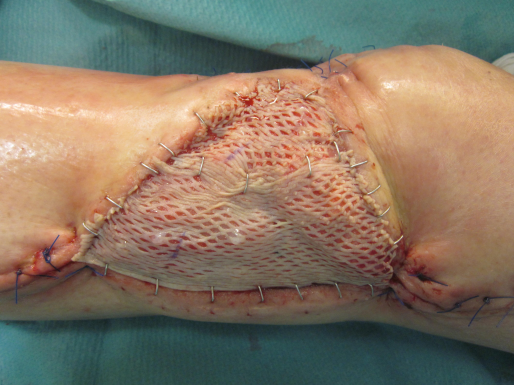
33 Days after admission to hospital the respiratory situation worsened again and bilateral pulmonary infiltration was noted. After consulting the thoracic surgery department, thoracotomy with debridement and decortication of the right lung was performed (Figure 4). 46 days after admission and following clinical improvement the patient was transferred to normal ward. The remaining soft tissue defect at his left knee was treated with negative pressure therapy and later closed with autologous skin graft (Figure 2 and 3). An intensive physiotherapeutic program was initialized and the patient was moved to a rehabilitation center subsequently. The total time of hospital stay in our clinic was 87 days, including 17 days of intensive care treatment.

At first follow up 5 months after initial admission, no signs of further infection could be identified. Both parameters, white cell count of 8,21 x 109 L-1 and C-reactive protein of 7,8 mg/l, were in normal range (Table 1). All former wounds appeared well healed without local inflammation. The patient was able to walk independently with help of two crutches and has already returned to his former job as engineer.
A follow up MRI of the left knee 6 months after admission showed signs of chronic low-grade osteomyelitis, however, an acute infection could be precluded (Figure 7). Because of limited pain complaints of the affected knee joint, an antibiotic therapy with Ciprofloxacin and Rifampicin was administered for 8 weeks anew. The patient was last seen 3 months later with good clinical results including full weight bearing of his left knee without any pain and ability to work in his former job without limitations.
| On admission | 1 day | 1 week | 2 weeks | 1 month | 2 months | 3 months | 5 months | 7 months | |
|---|---|---|---|---|---|---|---|---|---|
| WBC (G/l) | 14.66 | 15.36 | 24.04 | 11.11 | 14.27 | 6.59 | 6.02 | 8.29 | 8.01 |
| C-reactive protein (mg/l) | 319 | 233 | 241 | 107 | 119 | 88 | 35 | 7.2 | 4.3 |
| Procalcitonin (μ/l) | 27.23 | 34.51 | 2.56 | 2.99 | 1.67 |
Table 2: White blood cell count and acute phase reactants levels during clinical course of infection.
Discussion
This case presents an invasive community-onset PVL- positive staphylococcal infection with osteomyelitis of the tibia, multiorgan failure and necessity of extracorporeal membrane oxygenation which in that combination was to our knowledge not reported before.
The PVL-toxin was first described by Panton and Valentin in 1932 and is widely discussed ever since as a pathogenic or epidemiological marker [3, 4]. PVL-coding genes can occur in Methicillin-sensitive and –resistant strains, whereas PVL-
positive MRSA infections are more common in the USA than in Europe [3]. Remarkably, a study from France showed that strains with PVL-genes are more frequently causing disease and tissue destruction by direct invasion than causing secondary infection after injuries or in hospital-acquired pneumonia [5].
In 1999, Lina et al. examined 172 strains of S. aureus associated with various clinical syndromes for PVL-genes. 13 strains were detected in patients with osteomyelitis and only 23% of those were PVL-positive [5]. Boccini et al. found a more severe local disease and greater inflammatory response in such strains analyzing children with hematogenous osteomyelitis. Hence, PVL might play some kind of role in this context [6].
ARDS associated with PVL-positive S. aureus pneumonia is known as a severe complication with a mortality rate of more than 70% [7]. As described by Noah et al., the use of an ECMO is a valuable option to permit lung-protective ventilation and bridge the time an antibiotic therapy needs to take effect [8]. In this case, ECMO therapy was needed for 5 days.
In our case, the patient developed multiple soft tissue abscesses due to hematogenic spread on the basis of a gonarthritis. Early drainage of abscess and surgical debridement in combination with lavage is important and should be performed whenever possible [9, 10]. It has been shown that patients with PVL-positive infections are more likely to require surgical treatment [3]. Therefore, it might be useful to perform an early PVL testing in case a strong suspicion is present. The correct antibiotic therapy – advisably in agreement with the infection control team – should be supplemented by repetitive surgical debridement as soon as possible. A negative pressure wound therapy could be a valuable option. Following these procedures, a good clinical outcome could be achieved in our case.
Conflict of Interest
The authors declare that there is no conflict of interest. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Ansart S, Perez L, Jaureguiberry S, Danis M, Bricaire F, et al. (2007) Spectrum of dermatoses in 165 travelers returning from the tropics with skin diseases. Am J Trop Med Hyg 76(1): 184-186.
-
Caumes E, Carrière J, Guermonprez G, Bricaire F, Danis M, et al. (1995) Dermatoses associated with travel to tropical countries: A prospective study of the diagnosis and management of 269 patients presenting to a tropical disease unit. Clin Infect Dis 20(3): 542-548.
-
Shallcross LJ, Fragaszy E, Johnson AM, Hayward AC (2013) The role of the Panton-Valentine leucocidin toxin in staphylococcal disease: A systematic review and meta- analysis. Lancet Infect Dis 13(1): 43-54.
-
Panton PN, Valentine FCO (1932) Staphlyococcal toxin. Lancet 219(5662): 506-508.
-
Lina G, Piémont Y, Godail-Gamot F, Bes M, Peter MO, et al. (1999) Involvement of Panton-Valentine leukocidin- producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis 29(5): 1128- 1132.
-
Bocchini CE, Hulten KG, Mason EO, Gonzalez BE, Hammerman WA, et al. (2006) Panton-Valentine leukocidin genes are associated with enhanced inflammatory response and local disease in acute hematogenous Staphylococcus aureus osteomyelitis in children. Pediatrics 117(2): 433-440.
-
Morgan MS (2007) Diagnosis and treatment of Panton- Valentine leukocidin (PVL)-associated staphylococcal pneumonia. Int J Antimicrob Agents 30(4): 289-296.
-
Noah MA, Dawrant M, Faulkner GM, Hill AM, Harvey C, et al. (2010) Panton-Valentine leukocidin expressing Staphylococcus aureus pneumonia managed with extracorporeal membrane oxygenation: Experience and outcome. Crit Care Med 38: 2250-2253.
-
Gillet Y, Dumitrescu O, Tristan A, Dauwalder O, Javouhey E, et al. (2011) Pragmatic management of Panton- Valentine leukocidin-associated staphylococcal diseases. Int J Antimicrob Agents 38(11): 457-464.
-
Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, et al. (2011) Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 52(3): e18-55.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results