Reliability of the Posterior Condylar Axis as an Alternative Reference for Femoral Rotation in Japanese Patients with Varus Knee Osteoarthritis Undergoing Total Knee Arthroplasty
Background: This study aimed to assess the reliability of the posterior condylar axis (PCA), the most widely used alternative reference for the surgical transepicondylar axis (sTEA), as a reference for appropriate femoral rotational alignment in total knee arthroplasty (TKA) by comparing variances with other alternative reference axes. Methods: A total of 305 knees in 233 Japanese patients who underwent TKA due to varus knee osteoarthritis were assessed in this study. Variances and relationships between alternative references were determined. Angles of alternative reference axes relative to the sTEA in the axial plane were measured using computer software based on computed tomography. Results: The PCA line was 3.0°±1.8° (range, -2.1° to 8.8°) internally rotated relative to the sTEA. No significant differences were observed in the PCA angle relative to the sTEA angle between males and females. The variance with respect to the sTEA was significantly smaller in the order of anatomical transepicondylar axis (aTEA), PCA, and antero-posterior axis (APA). The variance of the APA and that of the femoral anterior tangent line (FAT) did not significantly differ, while the variance of the FAT was significantly smaller than that of the trochlear anterior line (TAL). The proportion of outliers for PCA (>3° away from the average value) was 9.8%. The PCA was weakly correlated with the aTEA, APA, FAT, and TAL. Conclusions: In terms of variance with respect to the sTEA, the PCA was second to aTEA in reliability as an alternative reference axis, and was on average 3.0°±1.8° internally rotated relative to the sTEA. Our findings suggest that the PCA is a reliable and reproducibly identifiable alternative axis for accurately determining femoral rotational alignment in TKA.
Introduction
Appropriate rotational alignment of the femoral component is essential for both successful outcomes and long-term survival of the implant itself in total knee arthroplasty (TKA) [1, 2, 3]. Studies have consistently used the surgical transepicondylar axis (sTEA) as the anatomical reference axis for this purpose [1, 4, 5]. Although the sTEA is the most reliable intraoperative rotational reference, its practical use can be difficult due to the location of the medial epicondyle and sulcus during surgery [1, 6]. The sTEA can also be difficult to identify in minimally invasive TKA due to limited surgical exposure. Thus, landmarks and axes that are both reliable and reproducibly identifiable are important for accurately determining proper rotational alignment. Secondary (alternative) reference axes used to determine the rotational alignment of the femoral component in previous studies include the posterior condylar axis (PCA) [7, 8], the trochlear anteroposterior axis (APA) (Whiteside’s line) [9], and the anatomical transepicondylar axis (aTEA) [6, 10], and several studies have examined the angles created between these reference axes [5, 9, 11, 12, 13, 14]. In addition, the femoral anterior tangent line (FAT) and the trochlear anterior line (TAL), two alternative reference axes in the anterior femur, are reportedly useful for determining the rotational alignment of the femoral component [11, 13, 14, 15, 16].
The most widely used alternative reference axis of the sTEA is the PCA [7]. The PCA is easily identifiable and is often used for setting femoral component rotation and determining correct component sizing. The PCA is internally rotated by an average of 3° relative to the sTEA [4, 6, 17, 18], and this corresponds to the built-in correction of the posterior referencing jig. Common TKA systems which use measured resection techniques adopt a fixed PCA (i.e., the same cutting angle default to 3° external rotation of the femoral component relative to the PCA).
Despite the importance of the PCA as an alternative reference, no study to date has compared its reliability to other alternative reference axes. We hypothesized that the PCA is a reliable and reproducibly identifiable axis for the accurate determination of proper rotational alignment in TKA. To this end, this study aimed to compare the variance of the PCA relative to those of other alternative reference axes.
Materials and Methods
This study targeted a total of 305 knees in 233 Japanese patients (44 men and 189 women) who underwent TKA due to varus knee osteoarthritis from October 2014 to December 2019. All patients were treated at our institution and had neither extra-articular deformity of the femur or tibia due to previous trauma or surgery (e.g., hip arthroplasty or internal fixation of a femoral fracture) nor severe distal femoral or tibial bone loss. Average age of participants was 74.8±8.1 years, and average femorotibial angle was 183.4°±4.6°. The Kellgren-Lawrence classification of osteoarthritis was grade III for 104 knees and grade IV for 201 knees.
To compare the reliability of the PCA as an alternative reference for setting the rotational alignment of the femoral component, we compared its variance to those of other alternative references (aTEA, APA, FAT, and TAL) and also investigated relationships among the alternative references. Angles of each alternative reference axis relative to the sTEA in the axial plane were measured using computer software (ZedKnee®) (LEXI Inc., Tokyo, Japan). A three-dimensional (3D) computed tomography (CT) scan of the whole leg was taken to create a preoperative TKA plan using 3D models of bone. The computer software created the femoral coordinate system based on a femoral coronal plane consisting of the spherically approximated femoral head center and the sTEA. The femoral mechanical axis was defined as the line connecting the center of the femoral head and the portion bisecting the prominence of the lateral epicondyle and the sulcus of the medial epicondyle (center of the knee).
The sTEA, aTEA, PCA, APA, FAT, and TAL were determined as described in previous studies. The sTEA was defined as the line connecting the prominence of the lateral epicondyle and the sulcus of the medial epicondyle [12, 17], the aTEA as the line connecting the prominence of the lateral epicondyle and the medial epicondyle [10, 12], the PCA as the line connecting the posterior aspects of the femoral posterior condyles [7, 8], the APA (Whiteside’s line) as the line connecting the deepest point of the patellar groove and the point of the intercondylar notch [1, 9], the FAT as the line parallel to the anterior surface of the distal femur in the axial plane where the femoral trochlea begins [14, 15, 16], and the TAL as the line connecting the anterior aspects of greatest protrusion of the femoral medial and lateral condyles [11, 13] (Figure 1). The ∠aTEA, ∠PCA, ∠FAT, and ∠TAL were defined as the aTEA, PCA, FAT, and TAL angles relative to the sTEA, respectively, and ∠⊥APA was defined as the line perpendicular to the APA angle relative to the sTEA. External rotation relative to the sTEA was defined as a positive value for the angles of the alternative reference axes. To evaluate intra- and inter- observer reliability, 50 patients were randomly selected, and all angular parameters were measured twice by two observers, with a 4-week interval between measurements. Intraclass correlation coefficients (ICCs) of intra-observer reliability were >0.90, and those of inter-observer reliability were >0.85 for all angular measurements. Given the high reproducibility of the angular measurements, those made by one of the researchers were used for all subsequent analyses. The sTEA, aTEA, PCA, APA, and TAL were definable on all assessed knees, while the FAT could not be defined on three knees due to extensive osteophyte formation from the anterior aspects of the femoral condyle.
This study was approved by the ethics committee of our institution, and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. Patient anonymity was maintained during data collection, and the security of personal information was strictly controlled.
Statistical Analysis
All values are presented as averages with standard deviations. The Shapiro-Wilk test was used to test the normality of data. Variances between alternative references were compared with the F-test. A sample size of 305 knees was determined to provide sufficient power (>80%) to show significant differences in variances between alternative references, with a two-tailed α of 0.05. Correlation analysis was performed using Pearson’s correlation coefficients. Comparisons between two groups were performed with the Mann-Whitney U test for continuous variables. Intra- and inter-observer reliabilities were determined with ICCs. P<0.05 was considered statistically significant. Data were analyzed using SPSS for Windows, version 22.0 (SPSS, Inc., Chicago, IL, USA).
Results
Angular parameters for the five alternative references relative to the sTEA are shown in Table
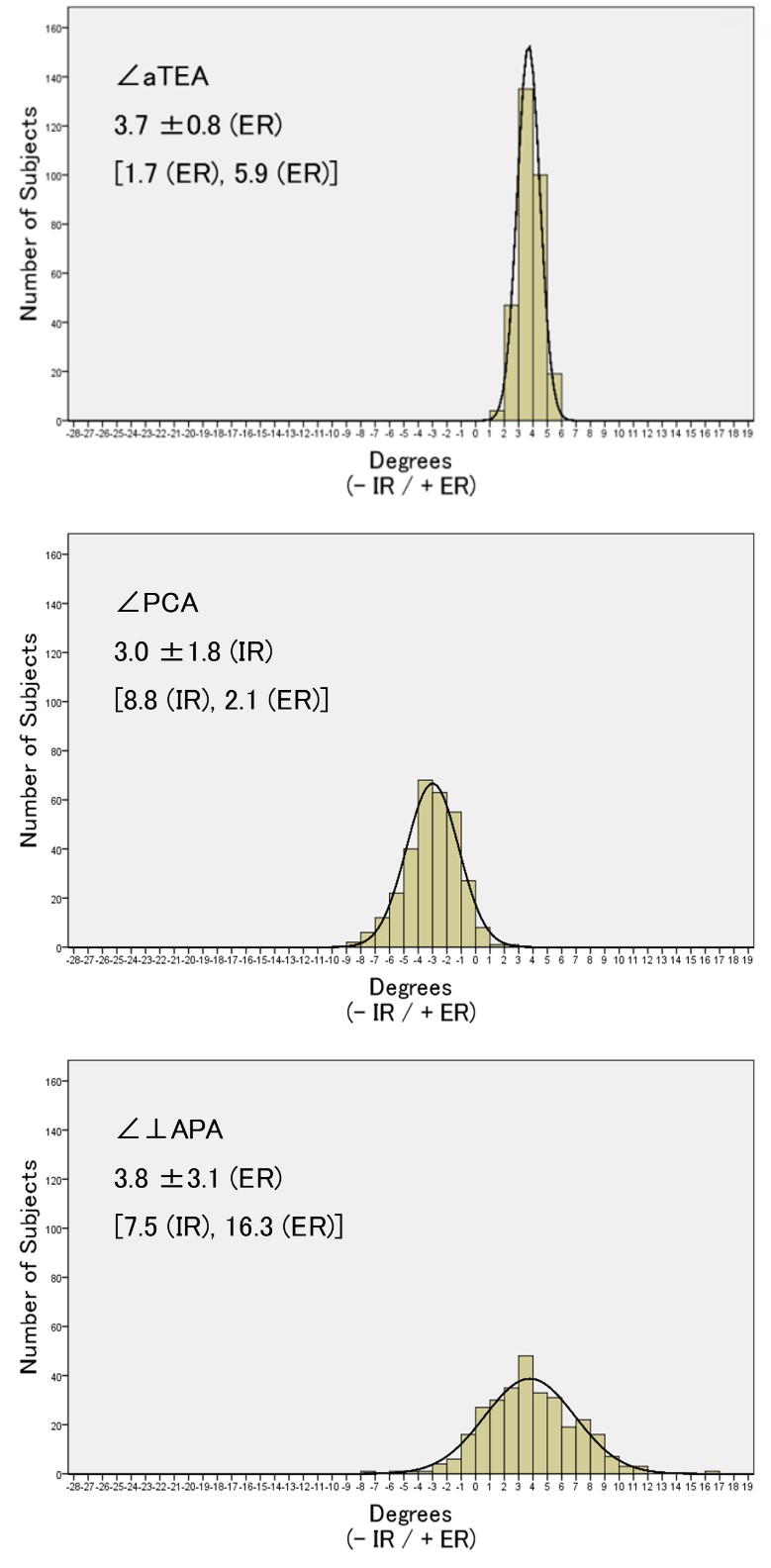
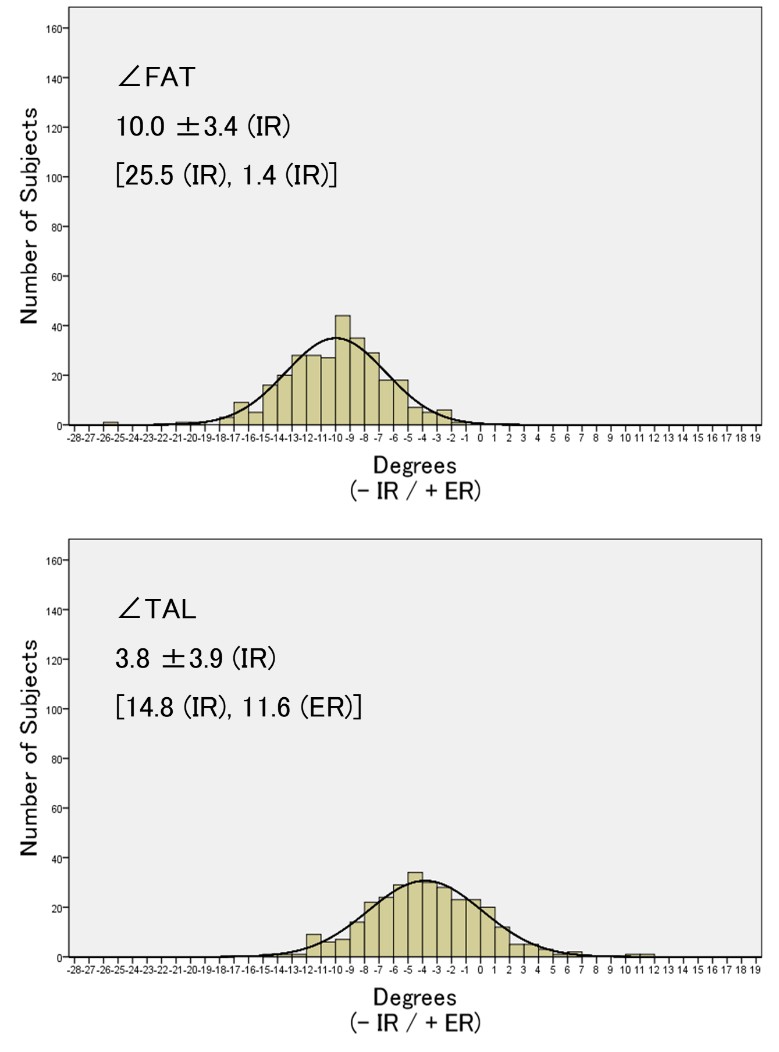
- External rotations relative to the sTEA were 3.7°±0.8° for the aTEA and 3.8°±3.1° for the ⊥APA. Internal rotations relative to the sTEA were 3.0°±1.8° for the PCA, 10.0°±3.4° for the FAT, and 3.8°±3.9° for the TAL. ∠PCA and ∠⊥APA did not significantly differ between males and females, while a significant difference was observed between sexes for ∠aTEA, ∠FAT, and ∠TAL. Distributions using histograms for the five alternative references relative to the sTEA are shown in Fig.
- All alternative references relative to the sTEA were normally distributed. Outliers of the PCA (>3° away from the average value) accounted for 9.8%. Table 2 shows a comparison of variances with respect to the sTEA between alternative references using the F-test. Variances were significantly smaller in the order of the ∠aTEA, ∠PCA, and ∠⊥APA. There was no significant difference between variances of the ∠⊥APA and ∠FAT. The variance of the ∠FAT was significantly smaller than that of the ∠TAL. Correlations between alternative references are shown in Table
- The ∠PCA was weakly correlated with the ∠aTEA (r: 0.29), ∠⊥APA (r: 0.27), ∠FAT (r: 0.34), and ∠TAL (r: 0.30).
| Angular parameter, ° ( - IR / + ER ) | Knees in all patients | Gender | |||
|---|---|---|---|---|---|
| Males | Females | p value | |||
| ∠aTEA | The aTEA angle relative to the sTEA | 3.7 ±0.8 | 3.4 ±0.7 | 3.8 ±0.8 | < 0.01 |
| ∠PCA | The PCA angle relative to the sTEA | -3.0 ±1.8 | -2.8 ±1.7 | -3.0 ±1.9 | 0.22 |
| ∠⊥APA | The line perpendicular to the APA angle relative to the sTEA | 3.8 ±3.1 | 3.9 ±2.6 | 3.8 ±3.3 | 0.72 |
| ∠FAT | The FAT angle relative to the sTEA | -10.0 ±3.4 | -11.3 ±2.5 | -9.7 ±3.6 | < 0.01 |
| ∠TAL | The TAL angle relative to the sTEA | -3.8 ±3.9 | -5.0 ±3.0 | -3.6 ±4.1 | < 0.05 |
| Values are presented as mean ± standard deviation. sTEA: surgical transepicondylar axis, aTEA: anatomical transepicondylar axis, PCA: posterior condylar axis, APA: trochlear anteroposterior axis, FAT: femoral anterior tangent line, TAL: trochlear anterior line, IR: internal rotation, ER: external rotation |
Table 1: Angular parameters for the five alternative references relative to the sTEA.
| ∠aTEA | ∠PCA | ∠⊥APA | ∠FAT | ∠TAL | |
|---|---|---|---|---|---|
| ∠aTEA | |||||
| F value | 1.0 | ||||
| ∠PCA | |||||
| F value | 141.2** | 1.0 | |||
| ∠⊥APA | |||||
| F value | 269.0** | 70.4** | 1.0 | ||
| ∠FAT | |||||
| F value | 272.2** | 86.3** | 3.7 | 1.0 | |
| ∠TAL | |||||
| F value | 284.1** | 108.2** | 11.7** | 4.1* | 1.0 |
| ∠aTEA | |||||
| r | 1.00 | ||||
| ∠PCA | |||||
| r | 0.29** | 1.00 | |||
| ∠⊥APA | |||||
| r | 0.14* | 0.27** | 1.00 | ||
| ∠FAT | |||||
| r | 0.12* | 0.34** | 0.34** | 1.00 | |
| ∠TAL | |||||
| r | 0.19** | 0.30** | 0.32** | 0.29* | 1.00 |
Table 2: Comparisons of variances with respect to the sTEA between alternative references by using F-test. **p<0.01, *p<0.05, sTE
Table 2: Comparisons of variances with respect to the sTEA between alternative references by using F-test. **p<0.01, *p<0.05, sTEA: surgical transepicondylar axis, aTEA: anatomical transepicondylar axis, PCA: posterior condylar axis, APA: trochlear anteroposterior axis, FAT: femoral anterior tangent line, TAL: trochlear anterior line, ∠aTEA: the aTEA angle relative to the sTEA, ∠PCA: the PCA angle relative to the sTEA, ∠⊥APA: the line perpendicular to the APA angle relative to the sTEA, ∠FAT: the FAT angle relative to the sTEA, ∠TAL: the TAL angle relative to the sTEA.
Table 3: Correlations between alternative references. r: correlation coefficient, **p<0.01, *p<0.05, sTEA: surgical transepicondylar axis, aTEA: anatomical transepicondylar axis, PCA: posterior condylar axis, APA: trochlear anteroposterior axis, FAT: femoral anterior tangent line, TAL: trochlear anterior line, ∠aTEA: the aTEA angle relative to the sTEA, ∠PCA: the PCA angle relative to the sTEA, ∠⊥APA: the line perpendicular to the APA angle relative to the sTEA, ∠FAT: the FAT angle relative to the sTEA, ∠TAL: the TAL angle relative to the sTEA.
Discussion
The present study is the first to investigate the reliability of the PCA as an alternative reference for the rotational alignment of the femoral component in TKA by comparing its variance to those of other alternative reference axes. Important findings of the present study were as follows: (1) as an alternative reference, the PCA is reliable and second only to aTEA in variance with respect to the sTEA, (2) the PCA was on average 3.0°±1.8° internally rotated relative to the sTEA, (3) the proportion of outliers for the PCA (>3° away from the average value) was 9.8%, and (4) there was little correlation between alternative references.
According to a literature review, the PCA is on average 3° internally rotated relative to the sTEA, 5° relative to the aTEA, and 4° relative to the line perpendicular to the APA [19]. However, the relationship between the transepicondylar axis and PCA varies in osteoarthritic knees, making such generalizations difficult [19]. Previous studies targeting Japanese patients reported the angle between the PCA and the aTEA to be on average 6°[18, 20], 6.8° [2], and 6.4° [6]. The APA is generally assumed to lie perpendicular to the transepicondylar axis and is thus considered a reliable axis of reference [1, 9]. However, this line can be difficult to draw accurately, and identifying it in cases of trochlear dysplasia or destructive arthritis is challenging [21]. In Japanese patients, the angle between the PCA and the line perpendicular to the APA has been reported to be on average 6.1° in patients with varus knee osteoarthritis and 3.5° in volunteers [20]. The results of the present study are similar to those reported previously, with the PCA on average 3.0° internally rotated relative to the sTEA, 6.7° relative to the aTEA, and 6.8° relative to the line perpendicular to the APA.
Surgeons typically compare the transepicondylar axis, the PCA, and the APA to ensure a more accurate rotational alignment of the femoral component. However, applying alternative references in the operative field is not always straightforward because arthritic changes such as deformities, bony defects, and osteophytes not only make it difficult to identify them, but also distort them [1, 12]. Some studies have reported the use of two or more axes in femoral rotational alignment [5, 22, 23]. In one study [24], a combination of three axes (PCA+3° external rotation, APA, and aTEA) maximized the accuracy of femoral rotational alignment in healthy femora without evidence of degenerative arthritis. The results of the present study revealed interindividual variability in the five alternative references, suggesting the possibility that using a single alternative reference could result in malrotation relative to the sTEA. We also found that a combination of three axes did not result in an accurate femoral rotational alignment in patients with varus knee osteoarthritis, since the interindividual variability (standard deviation = 1.4°) in these alternative references was inferior to that of the aTEA and there was little correlation between alternative references in each patient. Thus, the strategy of attempting to improve femoral rotational alignment by simply combining several alternative references might be unreliable in such patients, limiting the clinical utility of this approach.
The TAL has been reported to have a more consistent distribution than the FAT in variance, as the configuration of the anterior femoral surface to determine the FAT tends to be more variable [25]. In the present study, however, the FAT had a more consistent distribution than the TAL in variance, since the TAL was affected by arthritic changes such as osteophytes and deformities. As these alternative reference axes in the anterior femur had wide interindividual variability, the no use of angular reference tailored to each patient to target the sTEA may result in malrotation relative to the sTEA.
Since aiming for the transepicondylar axis directly has been shown in numerous studies to have lower reproducibility compared to referencing from the PCA [26, 27], simple and accurate systems to ensure external rotation relative to the PCA (surrogate landmark for the sTEA) have been used. Whether the PCA is a reliable intraoperative axis or not depends on how reproducibly accurate the detection of the PCA is intraoperatively, the posterior referencing jig used intraoperatively, and the operation support system used to determine intraoperative femoral component rotation. In the present study, the PCA had a homogenous distribution, with small ranges and standard deviations. The PCA is also useful when considering the variability that exists in the distal femoral rotational anatomy. While the angle between the PCA and sTEA has been reported to significantly differ by sex [24], we did not observe sex-based differences in this study. Importantly, however, 9.8% of patients had PCA TAL
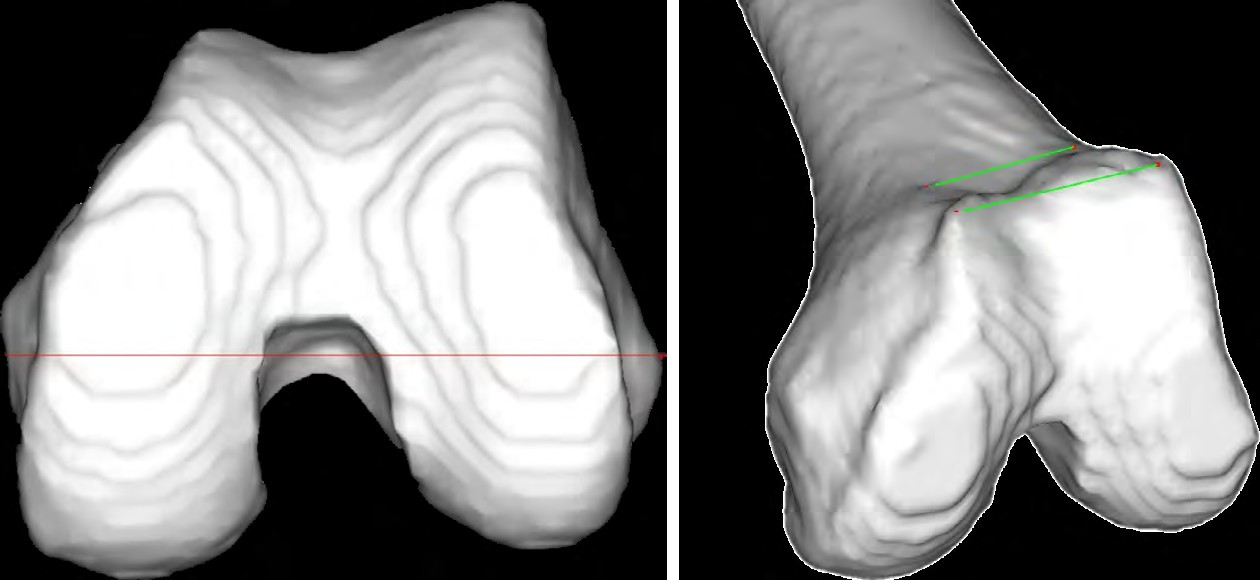
Figure 1: Alternative references for femoral component rotation are depicted. Three-dimensional reconstructed distal femur seen from below and from the front in an oblique direction. sTEA: surgical transepicondylar axis, aTEA: anatomical transepicondylar axis, PCA: posterior condylar axis, APA: trochlear anteroposterior axis, FAT: femoral anterior tangent line, and TAL: trochlear anterior line.
outliers, suggesting that reliance on a single reference axis or technique for every patient may not be appropriate. As the same cutting angle for posterior femoral resection may lead to malrotation of the femoral component, tailoring the PCA to each patient could enhance the accuracy of rotational alignment compared to using the same fixed PCA for all patients. Some studies recommend preoperative CT prior to TKA to obtain the PCA for each patient [19, 28, 29]. For viability in clinical settings, an individually-tailored PCA should be used to achieve appropriate rotational alignment of the femoral component and reduce the risk of postoperative malalignment due to planning errors that can arise from the use of a fixed PCA.
This study has some limitations. First, most patients were classified into Kellgren–Lawrence grade III or IV. Thus, disease progression may have impacted the measurements. Second, as there was no healthy control group, it is unclear to what extent variations in femoral shape were due to osteoarthritis. Third, despite accurate measurements of alternative reference axes on the femoral coordinate system, unlike magnetic resonance imaging, a CT scan (as used in the present study) does not show residual cartilage of the posterior condyle. In this regard, some studies have reported that an unequal amount of cartilage between the medial and lateral condyles in osteoarthritis can cause errors in determining the PCA [19, 30]. Finally, all samples were obtained from Japanese patients. Thus, our results may not fully apply to other populations.
TAL FAT
(A) aTEA
(B) PCA
(C) APA
(D) FAT
(E) TAL
Figure 2: Distributions using histograms for the five alternative references relative to the sTEA. Values are presented as mean ± standard deviation [range]. sTEA: surgical transepicondylar axis, aTEA: anatomical transepicondylar axis, PCA: posterior condylar axis, APA: trochlear anteroposterior axis, FAT: femoral anterior tangent line, TAL: trochlear anterior line, ∠aTEA: the aTEA angle relative to the sTEA, ∠PCA: the PCA angle relative to the sTEA, ∠⊥APA: the line perpendicular to the ⊥APA angle relative to the sTEA, ∠FAT: the FAT angle relative to the sTEA, ∠TAL: the TAL angle relative to the sTEA, IR: internal rotation, ER: external rotation.
Conclusion
We investigated the reliability of the PCA as an alternative reference for the rotational alignment of the femoral component by comparing its variance with several other alternative axes in Japanese patients with varus knee osteoarthritis undergoing TKA. The reliability of the PCA was second only to aTEA in terms of variance with respect to the sTEA, and was on average 3.0°±1.8° internally rotated relative to the sTEA. 9.8% of patients had PCA outliers, suggesting that tailoring the PCA to each patient could enhance the accuracy of rotational alignment. Our findings suggest that the PCA is a reliable and reproducibly identifiable alternative axis for accurately determining femoral rotational alignment in TKA.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgement
We thank Dr. Daihei Kida (Mie-LOCOMO Rheumatology Clinic, Yokkaichi, Japan), Dr. Nobunori Takahashi (Department of Orthopedic Surgery, Nagoya University Graduate School of Medicine, Nagoya, Japan), and Koichi Mori (Nagoya Ekisaikai Hospital, Nagoya, Japan) for their kind suggestions.
References
-
Arima J, Whiteside LA, McCarthy DS, White SE (1995) Femoral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg Am 77(9): 1331-1334.
-
Akagi M, Matsusue Y, Mata T, Asada Y, Horiguchi M, et al. (1999) Effect of rotational alignment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res 366: 155-163.
-
Sikorski JM (2008) Alignment in total knee replacement. J Bone Joint Surg Br 90(9): 1121-1127.
-
Asano T, Akagi M, Nakamura T (2005) The functional flexion-extension axis of the knee corresponds to the surgical epicondylar axis: in vivo analysis using a biplanar image-matching technique. J Arthroplasty 20(8): 1060-1067.
-
Paternostre F, Schwab PE, Thienpont E (2014) The combined Whiteside’s and posterior condylar line as a reliable reference to describe axial distal femoral anatomy in patient-specific instrument planning. Knee Surg Sports Traumatol Arthrosc 22(12): 3054-3059.
-
Yoshino N, Takai S, Ohtsuki Y, Hirasawa Y (2001) Computed tomography measurement of the surgical and clinical transepicondylar axis of the distal femur in osteoarthritic knees. J Arthroplasty 16(4): 493-497.
-
Laskin RS (1995) Flexion space configuration in total knee arthroplasty. J Arthroplasty 10(5): 657-660.
-
Hungerford DS, Krackow KA (1985) Total joint arthroplasty of the knee. Clin Orthop Relat Res 192: 23- 33.
-
Whiteside LA, Arima J (1995) The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop Relat Res 321: 168-172.
-
Stoeckl B, Nogler M, Krismer M, Beimel C, de la Barrera JL, et al. (2006) Reliability of the transepicondylar axis as an anatomical landmark in total knee arthroplasty. J Arthroplasty 21(6): 878-882.
-
Morizane K, Takahashi T, Konishi F, Yamamoto H (2011) The anterior trochlear line as a reference for femoral component positioning in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 19(12): 2009-2015.
-
Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS (1993) Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res 286: 40-47.
-
Talbot S, Bartlett J (2008) The anterior surface of the femur as a new landmark for femoral component rotation in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 16(3): 258-262.
-
Watanabe H, Gejo R, Matsuda Y, Tatsumi I, Hirakawa K, et al. (2011) Femoral anterior tangent line of the osteoarthritic knee for determining rotational alignment of the femoral component in total knee arthroplasty. J Arthroplasty 26(2): 268-273.
-
Watanabe H, Gejo R, Tokunaga A, Hirano N, Kimura T (2013) Intraoperative measurements of femoral anterior tangent (FAT) line for determining the rotational alignment of femoral component of total knee arthroplasty. J Arthroplasty 28(10): 1757-1759.
-
Hattori Y, Asai N, Mori K, Mori S, Ikuta K, et al. (2021) Evaluation of an operation support system using the femoral anterior tangent line to determine intraoperative femoral component rotation in total knee arthroplasty. J Orthop Sci S0949-2658(21): 00082-8.
-
Griffin FM, Insall JN, Scuderi GR (1998) The posterior condylar angle in osteoarthritic knees. J Arthroplasty 13(7): 812-815.
-
Matsuda S, Matsuda H, Miyagi T, Sasaki K, Iwamoto Y, et al. (1998) Femoral condyle geometry in the normal and varus knee. Clin Orthop Relat Res 349: 183-188.
-
Victor J (2009) Rotational alignment of the distal femur: a literature review. Orthop Traumatol Surg Res 95(5): 365-372.
-
Nagamine R, Miura H, Inoue Y, Urabe K, Matsuda S, et al. (1998) Reliability of the anteroposterior axis and the posterior condylar axis for determining rotational alignment of the femoral component in total knee arthroplasty. J Orthop Sci 3(4): 194-198.
-
Vanin N, Panzica M, Dikos G, Krettek C, Hankemeier S (2011) Rotational alignment in total knee arthroplasty: intraoperative inter- and intraobserver reliability of Whiteside’s line. Arch Orthop Trauma Surg 131(11): 1477-1480.
-
Aunan E, Ostergaard D, Meland A, Dalheim K, Sandvik L (2017) A simple method for accurate rotational positioning of the femoral component in total knee arthroplasty. Acta Orthop 88(6): 657-663.
-
Inui H, Taketomi S, Nakamura K, Sanada T, Tanaka S, et al. (2013) An additional reference axis improves femoral rotation alignment in image-free computer navigation assisted total knee arthroplasty. J Arthroplasty 28(5): 766-771.
-
Jang ES, Connors-Ehlert R, LiArno S, Geller JA, Cooper HJ, et al. (2019) Accuracy of Reference Axes for Femoral Component Rotation in Total Knee Arthroplasty: Computed Tomography-Based Study of 2,128 Femora. J Bone Joint Surg Am 101(23): e125.
-
Ji HM, Jin DS, Han J, Choo HS, Won YY (2016) Comparison of alternate references for femoral rotation in female patients undergoing total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 24(8): 2402-2406.
-
Jerosch J, Peuker E, Philipps B, Filler T (2002) Interindividual reproducibility in perioperative rotational alignment of femoral components in knee prosthetic surgery using the transepicondylar axis. Knee Surg Sports Traumatol Arthrosc 10(3): 194-197.
-
Kinzel V, Ledger M, Shakespeare D (2005) Can the epicondylar axis be defined accurately in total knee arthroplasty? Knee 12(4): 293-296.
-
Luyckx T, Zambianchi F, Catani F, Bellemans J, Victor J (2013) Coronal alignment is a predictor of the rotational geometry of the distal femur in the osteo-arthritic knee. Knee Surg Sports Traumatol Arthrosc 21(10): 2331- 2337.
-
Thienpont E, Schwab PE, Paternostre F, Koch P (2014) Rotational alignment of the distal femur: anthropometric measurements with CT-based patient-specific instruments planning show high variability of the posterior condylar angle. Knee Surg Sports Traumatol Arthrosc 22(12): 2995-3002.
-
Tashiro Y, Uemura M, Matsuda S, Okazaki K, Kawahara S, et al. (2012) Articular cartilage of the posterior condyle can affect rotational alignment in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 20(8): 1463-1469.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results