A Review of Necrotizing Fasciitis and the Utility of the Laboratory Risk Indicator for Necrotizing Fasciitis Score in its Early Diagnosis at a Rural Australian Hospital
Background: Necrotizing fasciitis is a life-threatening orthopaedic emergency. This paper is a retrospective review of confirmed cases of necrotizing fasciitis (NF) in a rural centre. The primary aim was to define the trends in incidence, microbiological profile, management and mortality. The secondary aim was to assess the accuracy of the LRINEC score as a tool to diagnose and distinguish NF from cellulitis and other non-necrotizing soft tissue infections (NNSTIs). Methods: A retrospective paper based, and computerized search of the medical records was undertaken to identify adult patients diagnosed with NF between January 2009 and January 2018 was conducted. An age matched control group was generated from a randomized sample of patients diagnosed with cellulitis over the same timeframe. LRINEC scores of the NF and control group were calculated and compared. Results: Forty-five patients with NF were identified. A decreasing trend in incidence was noted from 2011 (5.43 per 100000 per year) to 2016 (3.81 per 100000 per year), however 13 cases of necrotizing fasciitis presented in 2017 with an estimated incidence of 13.7 per 100000. The overall mortality of patients with NF was 15.6%. The genus Streptococcus was the most common isolate (47%) with Staphylococcus a close second (32.4%). The LRINEC score had a sensitivity of 61% and a specificity of 79% at a score of ≥ 6. Conclusion: LRINEC scores in isolation cannot be reliably used to distinguish between NF and NNSTIs. A high index of clinical suspicion and early surgical referral for surgical cut-down diagnosis is recommended.
Manuscript Background
Necrotizing fasciitis (NF) is a relatively rare, rapidly progressing skin and soft tissue infection with potential life and limb-threatening consequences making early diagnosis of the utmost importance. The global incidence has been reported to be around 0.40 cases per 100,000 affecting primarily middle-aged to elderly males [1]. The lower extremities seem to have the highest rates of NF followed by the abdomen and then the perineum [2]. Mortality rates vary considerably between studies, however, data from various centres in Australia and New Zealand demonstrate a mortality rate between 15.9% and 20.3% [3, 4]. Multiple risk factors are associated with NF. Some of these include advanced age, smoking, obesity, diabetes, immunosuppression, intravenous drug use, chronic kidney disease and peripheral vascular disease [1]. Classic physical examination signs have been proposed to differentiate NF from non-necrotizing soft tissue infections (NNSTIs), including severe pain, erythema, oedema, haemorrhagic bullae, fever, and septic shock [5]. Various imaging modalities are utilized in diagnosis, i.e., plain radiography may demonstrate gas in the soft tissues. Additionally, Computed Tomography (CT) performed with contrast may demonstrate fascial air or gas, soft-tissue oedema, or enhancement of the fascia [5]. Early in the infection, signs such as swelling, pain and erythema can be indistinguishable from cellulitis or abscess formation. As a result, studies have shown delayed diagnosis occur in 46– 80% of patients [6]. This unfortunately results in potentially preventable morbidity and mortality. Early recognition of NF, with timely and aggressive surgical debridement, remains the mainstay of successful treatment [6].
Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) is a scoring tool developed in 2004 for distinguishing NF from other soft tissue infections [7]. LRINEC scoring methodology is represented in Table 1. The developmental investigation by Wong, et al. [6] reported the tool had a sensitivity of 90%, specificity of 95%, 92% positive predictive value and 96% negative predictive value for detecting early NF.
| Variable | Range | Score |
|---|---|---|
| CRP | >150 | 4 |
| White cell count per mm3 | <15 | 0 |
| 15-25 | 1 | |
| >25 | 2 | |
| Haemoglobin, g/ml | >135 | 0 |
| 110-135 | 1 | |
| <110 | 2 | |
| Sodium, mmol/L | <135 | 2 |
| Creatinine, µmol/L | >141 | 2 |
| Gloucose, mmol/L | >10 | 1 |
| Total Score | Risk Stratification | |
| ≤5 | Low risk | <50% chance of necrotizing fasciitis |
| 6-7 | Medium risk | 50-75% Chance |
| ≥8 | High risk | >75% Chance |
Table 1: Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) is a scoring tool.
In 2012, Chun-I, et al. [8] published a validation study examining 233 patients with NF and 3,155 with severe cellulitis. They found that a LRINEC score >=6 had a sensitivity of 59.2% (CI 52.9-65.6%), specificity of 83.8% (CI 81.9 - 85.7%), likelihood ratio of 3.89, positive predictive ratio of 37.9% (95% CI 32.9-42.9%), and negative predictive ratio of 92.5% (95% CI 91.0-94.0%) [7]. Further concluded in the study was severe cellulitis had a LRINEC score ≥ 6 only 16.2% of the time.
However, in 2018, Narasimhan, et al. [6] concluded the use of the LRINEC score for early diagnosis of NF correlated well with clinical diagnosis, with a Spearman ρ correlation coefficient of 0.708 (P < 0.001). Furthermore, diagnostic accuracy was excellent, with an area under the ROC curve of 0.925 (0.890–0.959, P < 0.001. We have reviewed the incidence, risk factors, microbiology, management, and outcomes of patients with NF at Bundaberg Base Hospital (BBH), a rural hospital in Queensland over a 9-year span. Special attention has been paid to the method of diagnosis and the LRINEC scores. A randomized, age range matched group of patients within the same time frame, with the diagnosis of cellulitis, have been used as the control group to determine the utility of the LRINEC tool in our setting.
Methods and Materials
Data Collection
To conduct a retrospective observational study of NF at Bundaberg Base Hospital (BBH), a search of clinical records in our medical archives was performed. The search identified all adults managed at BBH between the 1st of January 2009 and the 1st of January 2018 with a diagnosis at the time of discharge of either necrotizing fasciitis (ICD M72.6) or Fournier’s gangrene (ICD N49.3). Forty-five cases of NF infections were found. The 45 clinical records and operative notes were reviewed to confirm that the diagnosis was accurate. We determined the accuracy using the usual definitive diagnosis based on operative findings such as necrotic, grey, and bloodless fascia [4]. The 45 NF patients’ demographic information, co-morbidities, aetiology, microbiology, clinical and biochemical variables on admission were recorded. All blood and tissue culture results were also recorded. LRINEC scores based on their initial blood workup were calculated. Two of the positive patients had incomplete laboratory test and therefore their LRINEC scores could not be calculated. This brought the total number of confirmed NF cases with LRINEC scores to forty-three (study n=43). Outcome measures for the NF group included the length of hospital stay, ICU admission, interhospital transfers, and time to surgical intervention from admission, number of operations, amputations and mortalities. The incidence of NF was calculated for each year with reference to the population of the Bundaberg Base Hospital catchment area.
A case control study was undertaken to assess the utility of the LRINEC score in distinguishing between NF and NNSTIs. Medical records of all patients with a diagnosis of cellulitis occurring in the same time frame were retrieved to develop a control group. The control group data was age range matched (23 to 85 years old) generating 3812 patients. Individual control group subjects were selected by random number generation. Medical records with insufficient criteria were omitted from this study resulting in a control group of forty-seven subjects (control n=47).
Statistical Analysis
All statistical analysis was conducted with an alpha (α) of 0.05 in NCSS™. Data was assessed for normal distribution with the Shapiro-Wilk W test. Followed by analysis using the students t-test or the Mann-Whitney U test for continuous data; chi-squared test for nominal data.
Results
Forty-five patients were diagnosed with NF between 1st January 2009 and 1st of January 2018.The group had a mean age of 56 years. The cohort included 30 males (66.6%) and 15 females. The average BMI was 30. The average number of days from onset of symptoms to presentation was 6 days. The mean length of hospital stay was 19 days for the NF group and 7 days for the cellulitis group (p<0.001).
The most common site of NF infection was the lower limb at 36% (n=16). The anatomical regions affected with NF are summarized in Table 2. Of the forty-five patients with NF, 57.8% (n=26) were smokers and 37.8% (n=17) had diabetes. The comorbidities are summarised in Table 3 along with their association with mortality.
| % | n | |
|---|---|---|
| Lower limb | 36 | 16 |
| Perineum | 20 | 6 |
| Foot | 18 | 8 |
| Upper limb | 13 | 6 |
| Trunk | 7 | 3 |
| Hand | 4 | 2 |
| Digit | 2 | 1 |
Table 2: Anatomical regions affected with NF.
| % (n=45) | n | Deceased with Comorbidity | Deceased from group | Deceased (n=7) with Comorbidity | |
|---|---|---|---|---|---|
| Smokers | 57.8% | 26 | 3 | 11.5% | 42.9% |
| Diabetes | 37.8% | 17 | 2 | 11.8% | 28.6% |
| NSAID | 35.7% | 15 | 2 | 13.3% | 28.6% |
| Alcohol abuse | 33.3% | 15 | 3 | 20.0% | 42.9% |
| Immunosuppressed | 19.0% | 8 | 4 | 50.0% | 57.1% |
| Gout | 18.2% | 8 | 1 | 12.5% | 14.3% |
| PVD | 18.2% | 8 | 0 | 0.0% | 0.0% |
| IVDU | 17.8% | 8 | 2 | 25.0% | 28.6% |
| CKD | 11.4% | 5 | 1 | 20.0% | 14.3% |
| Obesity | 8.9% | 4 | 2 | 50.0% | 28.6% |
Table 3: Comorbidities of patients with NF.
Upon admission, only eighteen patients (40.0%) were confidently assigned a definite diagnosis of NF and commenced on appropriate treatment based on clinical findings alone. Imaging was used as a diagnostic tool in six patients (13.3%). Twenty-one patients (46.6%) were assigned a suspected diagnosis of NF and proceeded to surgical cut downs in theatre where the diagnosis was confirmed intraoperatively. All our patients were deemed suitable operative candidates and proceeded to surgical debridement. Nearly 30.0% of patients (n=13) did not have surgical management within 24 hours with an average delay of 31.6 hours to surgical debridement. Our patients had a mean length of stay of
19 days, underwent a median of two procedures with five (11.0%) eventually requiring limb amputations. Twenty- six NF patients (58%) required an ICU admission compared to 2% in the cellulitis control group (p<0.001) and fifteen (33.0%) of the patients were transferred to a tertiary health facility for further management. Forty patients with necrotizing fasciitis (88.9%) had positive blood, tissue, or swab microbiology cultures. Of these twenty-one (52.5%) were monomicrobial. The genus Streptococcus was the most common isolate (35.0%) with mixed enteric bacteria forming 28% and Staphylococcus (18.0%).
| Pathogen | Monomicrobial n=21 21/40 (52.5%) | percentage of monomicrobial=X/21 |
|---|---|---|
| Streptococcus pyogenes | 7 | 33.3% |
| Staphylococcus aureus | 4 | 19% |
| Aeromonas hydrophila | 3 | 14.3% |
| Escherichia coli | 2 | 9.5% |
| Streptococcus agalctiae | 1 | 4.7% |
| Serratia marcescens | 1 | 4.7% |
| Enterobacter asburiae | 1 | 4.7% |
| Klebsiella Pneumonia | 1 | 4.7% |
| Vibrio Vulnificus | 1 | 4.7% |
Table 4: Microbiology Data for NF group with positive monomicrobial microbiology cultures (n=21).
| Pathogen | Polymicrobial 19/40=47.5% | Percentage of polymicrobial=x/19 |
|---|---|---|
| Mixed enteric bacteria | 11 | 57.9% |
| Staphylacoccus aureus | 3 | 15.8% |
| Proteus mirabilis | 3 | 15.8% |
| Streptococcus pyogenes | 2 | 10.5% |
| Streptococcus agalactiae | 2 | 10.5% |
| Enterococcus faecalis | 2 | 10.5% |
| Pseudomonas aeruginosa | 2 | 10.5% |
| Morganella morgani | 1 | 5.3% |
| Klebsiella axytoca | 1 | 5.3% |
| Enterobacter cloacae | 1 | 5.3% |
| Candida albicans | 1 | 5.3% |
| Streptococcus constellatus | 1 | 5.3% |
| Streptococcus milleri | 1 | 5.3% |
| Bacteroides ureolyticus | 1 | 5.3% |
| Finegoldia magna | 1 | 5.3% |
| Eikenella corrodens | 1 | 5.3% |
| Vibrio parahaemalyticus | 1 | 5.3% |
| Aeromonas hydrophilia | 1 | 5.3% |
Table 5: Microbiology Data for NF group with positive polymicrobial microbiology cultures (n=19).
Only 18 patients (40%) with NF received the recommended electronic therapeutic guidelines (ETG) empirical triple antibiotic regimen used at our facility vancomycin; lincomycin or clindamycin and meropenem or piperacillin-tazobactam with definitive regimens guided by microbiology. The microbiology findings are summarised in the Tables 4 & 5. The overall mortality of these patients was 15.6% (n=7). A decreasing trend in incidence was noted from 2011 (5.43 per 100000 per year) to 2016 (3.81 per 100000 per year); however, 13 cases of necrotizing fasciitis presented in 2017 with an estimated incidence of 13.7 per 100000. No clear cause for this spike in incidence was identified.
Comparison of LRINEC Scores between Necrotizing Fasciitis and Cellulitis Groups
The forty-three NF patients had complete laboratory work and their LRINEC scores were calculated. Twenty-six of these patients (60.5%) had a LRINEC score of ≥6. Eight (41.9%) had a score of ≥8 (Table 7). Of the forty-seven randomised patients with cellulitis, ten (21.3%) had a score of ≥6 and four (8.5%) had a score of ≥8. A statistically significant difference was reported between the LRINEC scores as well as between the three risk categories. Analysis on the LRINEC components revealed a statistically significant difference (P <0.05) between the sample groups of sodium (Na), white cell count (WCC), creatinine (Cr) and C-reactive protein (CRP) measures (Table 6).
| Cellulitis | NF | P-Value | ||
|---|---|---|---|---|
| HB | 134 (127-139) | 126 (121-140) | <0.323t | |
| Na | 135 (134-137) | 133 (132-135) | <0.013u | |
| WCC | 10.1 (8.8-12) | 15.9 (13.5-17.9) | <0.001u | |
| BSL | 6.9 (5.9-8.3) | 8.1 (6.5-10.8) | <0.0242u | |
| Cr | 75 (67-93) | 118 (85-148) | <0.002u | |
| CRP | 52 (23-95) | 249 (149-294) | <0.00tu | |
| LRINEC SCORE | 3 (1-4) | 7 (5-8) | <0.010# | |
| LRINEC SCORE STRATIFIED | Totals | P-Value | ||
| Low risks (55) | 37 (78.7%) | 17 (39.5%) | 54 (60.0%) | <0.001# |
| Medium risk (6-7) | 6 (12.8%) | 8 (185.6%) | 14 (15.6%) | |
| High risk (≥8) | 4 (8.5%) | 18 (41.9%) | 22 (24.4%) | |
| Totals | 47 (100%) | 43 (100%) | 90 (100%) |
Table 6: LRINEC score components.
Normality of data was accessed with Shapiro-Wilk W test. Data is represented as median (95% CL LCL-UCL), and number (percentage,%). t=student’s t=test #= Chi-squared test u= Mann-Whitney U-test. Table 6: LRINEC score components.
Diagnostic Utility
In our study a score of ≥ 6 had a sensitivity of 60.5%
and specificity of 78.7%. The accuracy at ≥ 6 was 70.0%. The diagnostic accuracy of the LRINEC scoring method in our study is summarised in Table 7.
| LRINEC score | |||
|---|---|---|---|
| ≤5 | ≥6 | ≥8 | |
| Total (n=90) | 54 (60%) | 36 (40%) | 22 (24%) |
| Cellulitis (n=47) | 37 (79%) | 10 (21%) | 4 (9%) |
| NF (n=43) | 17 (40%) | 26 (60%) | 18 (42%) |
| Sensitivity/Correct identify pos | 72.1% | 60.5% | 41.9% |
| Specificity/Correct identify neg | 74.5% | 78.7% | 91.5% |
| Positive predictive value/True pos | 72.1% | 72.2% | 81.82% |
| Negative predictive value/True neg | 74.5% | 68.5% | 63.24% |
| Likelihood ratio (+)/False neg | 2.82 | 2.84% | 4.92 |
| Likelihood ratio (-)/False pos | 0.38 | 0.50 | 0.64 |
| Accuracy | 73.3% | 70.0% | 67.8% |
| False Positive Rate/Falsely rejecting the null hypothesis | 25.5% | 21.3% | 8.5% |
Table 7: Diagnostic accuracy of LRINEC scoring method.
Prevalence of NF in group is 47.8% Table 7: Diagnostic accuracy of LRINEC scoring method.
The LRINEC score spearman ρ correlation coefficient of diagnosing NF was 0.4841 (P <0.001). Additionally, the receiver operating characteristic (ROC) area under the curve (AUC) measure was ~0.779 (0.663-0.858, P <0.001). This is represented in Figure 1.
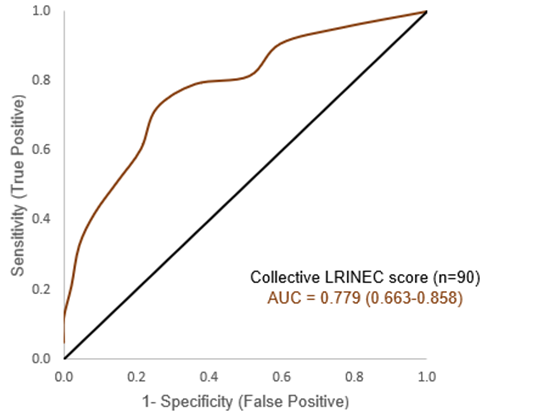
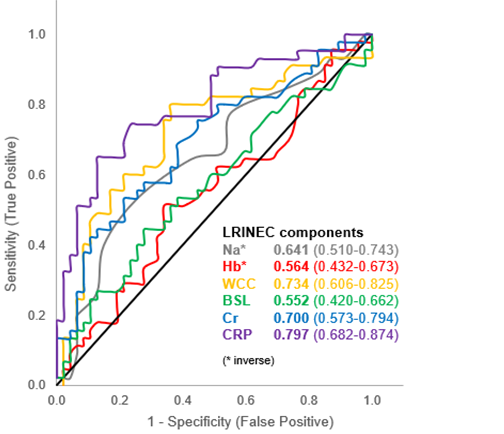
Figure 2 illustrates the ROC curves and AUC measures of each LRINEC component. Wherein, the CRP has the greatest measure of accuracy at 0.797 (0.682-0.875, P <0.001) with BSL the lowest at 0.552 (0.420-0.662, P ~0.198).
Discussion
This 9-year review of NF is the largest single centre series of NF in a rural Queensland hospital that also evaluates the utility of the LRINEC score in our population. The most significant findings of this study are the increasing incidence of NF in our community, the delay in diagnosis and first surgical debridement and the poor utility of the LRINEC score in distinguishing between NF and non- necrotizing soft tissue infections (NNSTIs). Holland in 2009 performed a retrospective review of the application of the LRINEC score in a tropical tertiary referral centre. He admits that his sample size was small with only 10 biopsy-proven NF patients and 18 controls that were also selected on the basis of an admitting diagnosis of NF and later had negative biopsy results or deemed not to require a biopsy [9]. His calculated sensitivity was 80% and specificity was 67% with the inherent inaccuracies of a small sample size and a control group with severe enough NNSTIs that a diagnosis of NF was initially made. This may have skewed the LRINEC scores as the tool is essentially a measure of the systemic inflammatory response to infection.
We did not identify any obvious reason for our increasing incidence and further research into this is indicated. The average time from onset to presentation to a hospital is also concerning at six days. This may be due to our rural population, decreased medical literacy, wide catchment area and smaller health facilities with limited resources that may be the first contact for patients with NF. Therefore, studies like ours may improve time to presentation, diagnosis and treatment if disseminated amongst our rural doctors to encourage early referrals to facilities with surgical services. While most facilities admit patients with cellulitis to medical teams, Kulasegaran et al. demonstrated that a policy of admitting patients with cellulitis under general surgery leads to prompt identification of NF and appropriate surgical care with a median time to operation of 10hrs [4]. In addition, McHenry et al. showed that the average time from admission to operation in those who survived was 25 h versus 90 h in the non-survivors. This was both clinically and statistically significant [4, 10].
It is therefore imperative that we diagnose and treat patients with NF early. Fernando et al explored the various tools at our disposal to make an early diagnosis and demonstrated that imaging tests should only be used as adjuncts and did not find LRINEC scores to be particularly sensitive in the diagnosis of NF [5]. Wong, et al. [7] LRINEC study was internally validated using a small cohort, this revealed a sensitivity of 90%, specificity of 95%, 92% positive predictive value and 96% negative predictive value for detecting early NF. Our study and others have revealed less encouraging results. This is summarised table 8 below.
| Wong 2004 | Chun-I 2012 | Narasimhan 2016 | Our Results | |
|---|---|---|---|---|
| Sensitivity | 90% | 60% | 76% | 61% |
| Specificity | 95% | 84% | 93% | 79% |
| PPV | 92% | 38% | 86% | 73% |
| NPV | 96% | 93% | 88% | 69% |
Table 8: Comparison of diagnostic parameters Our results are similar to other published validation studies overseas and Narasimha
Table 8: Comparison of diagnostic parameters Our results are similar to other published validation studies overseas and Narasimhan et al. in 2016 at the Royal Darwin Hospital. The LRINEC score consistently has a low sensitivity and slightly better specificity suggesting that with further improvements to this score may achieve a role in ruling out NF, but it is currently not a reliable diagnostic tool. Narasimhan, et al. [6] concluded that the LRINEC score accurately excludes significant disease with a low-risk score (LRINEC ≤5). They were willing to accept the false positive rate therefore making it an excellent tool in the context of high clinical suspicion to pick up most patients with NF. However, they do acknowledge that they did not consider the time to presentation which is often delayed in the Northern Territory due to varied access to medical services. Their patients anecdotally present late with severe disease that is reflected in biochemical variables [6]. Our false positive rate was 21% in the cellulitis group. We find this difficult to accept as it can be misleading and result in unnecessary surgical procedures with their attendant risks and expenditure of resources. Our false negative rate was 40% which we similarly find unacceptable as a false sense of reassurance would lead to delays in diagnosis that has been demonstrated to result in increased morbidity and mortality from NF. Regarding microbiology, our population had predominantly monomicrobial infections with Streptococcus our most common isolate (35%).
Mixed enteric bacteria (28%) formed the predominant group in the polymicrobial infections. This is comparable to Kulasegaran et al. that found slight predominance of monomicrobial infections_. Streptococcus pyogenes_ was their most common causative pathogen isolated in both monomicrobial and polymicrobial encounters. Anaerobes, often mixed, were the most common causative organism found in the polymicrobial group [4]. Antibiotic sensitivity profiles did not form part of our objectives for this study.
There are some limitations in this study that warrant mention. This is a retrospective review with reliance on paper-based documentation completeness and accuracy. We strived to exclude all subjects with incomplete data.
Conclusion
We conclude that LRINEC scores in isolation cannot be reliably used to distinguish between NF and NNSTIs. A high index of clinical suspicion and early surgical referral for surgical cut-down diagnosis is recommended. Given that a significant proportion of patients in our facility experienced delays prior to surgical debridement, prompt diagnosis remains a challenge but is of the utmost importance. Despite comparable mortality rates with other centres, further improvements can be made to facilitate early diagnosis and time to operation.
Declarations
Ethics Approval
Ethics approval was obtained from The Prince Charles Hospital Human Research Ethics committee.
Availability of Data and Materials
The data and materials used during this study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests in relation to this study.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Acknowledgements
Not applicable.
Authors Contributions
This study was designed, conducted and authored by AK. ZM and KK contributed to data collection. DH performed statistical analysis. AM guided authorship of the manuscript. DP was the academic supervisor.
References
-
Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, et al. (2014) Current concepts in the management of necrotizing fasciitis. Front Surg 1: 36.
-
Anaya DA, McMahon K, Nathens AB, Sullivan SR, Foy H, et al. (2005) Predictors of mortality and limb loss in necrotizing soft tissue infections. Arch Surg 140(2): 151- 157.
-
Proud D, Raiola FB, Holden D, Paul E, Capstick R, et al. (2014) Are we getting necrotizing soft tissue infections right? A 10‐year review. ANZ J Surg 84(6): 468-472.
-
Kulasegaran S, Cribb B, Vandal AC, McBride S, Holland D, et al. (2016) Necrotizing fasciitis: 11‐year retrospective case review in South Auckland. ANZ J Surg 86(10): 826- 830.
-
Fernando SM, Tran A, Cheng W, Rochwerg B, Kyeremanteng K, et al. (2019) Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-analysis. 269(1): 58-65.
-
Narasimhan V, Ooi G, Weidlich S, Carson P (2018) Laboratory Risk Indicator for Necrotizing Fasciitis score for early diagnosis of necrotizing fasciitis in Darwin. ANZ J Surg 88(1-2): E45-E49.
-
Wong CH, Khin LW, Heng KS, Tan KC, Low CO (2004) The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) scores: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med 32(7): 1535-1541.
-
Liao CI, Lee YK, Su YC, Chuang CH, Wong CH (2012) Validation of the laboratory risk indicator for necrotizing fasciitis (LRINEC) score for early diagnosis of necrotizing fasciitis. Tzu Chi Medical Journal 24(2): 73-76.
-
Holland MJ (2009) Application of the Laboratory Risk Indicator in Necrotizing Fasciitis (LRINEC) score to patients in a tropical tertiary referral center. Anaesth Intensive Care 37(4): 588-592.
-
McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA (1995) Determinants of mortality for necrotizing soft- tissue infections. Ann Surg 221(5): 558-563.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results