Time Frame to Surgery from Presentation of Ankle Fractures and the Impact of the BOAST Standards, do we meet the BOAST Guidelines?
Purpose: The aim of this study was to evaluate the compliance with the BOAST guidelines for early fixation on the day or day after ankle fractures in the age group of 60 years old or less when the ankle mortise is unstable. Method: This retrospective study reviewed all the ankle fractures that were admitted for ankle fixation in 2015-2016, preBOAST standard, and following it in 2018- 2019. The inclusion and exclusion criteria used in the standard were then applied. Results: In 2018-19, 44 patients fulfilled the inclusion criteria, 18 males with an average age of 39.3 and 26 females with an average age of 42.2. Twenty-nine ankles (66%) were fixed on the day or day after injury while 5 ankles (11%) had the surgery within 48 hours. In 2015-16, 37 patients fulfilled our inclusion criteria, 21 males with an average age of 37.8 years, 16 females with an average age of 42.1 years. Twenty-one ankles (56.7%) were fixed on the day or day after injury. While 8 ankles (21.6%) had the surgery within 48 hours. Conclusion: Most of the ankle fractures requiring surgery, who presented to our trust, were fixed within 48 hours accounting for 77% of cases in 2018-19 versus 79% in 2015-16 with no statistically significant difference in our practice between pre and post BOAST guidelines publishing. The rest of cases had delayed fixation mainly due to the surrounding soft tissue swelling.
Ahmed Al Wadiya1*, Mohamed Nagy2, Mohammed Hassan3, Islam Sarhan4 and Neil Ashwood5
Introduction
Ankle fractures are common accounting for 9-10% of all fractures [1], being the fourth most common injury [2]. Ankle fractures account for the half the fractures in the foot and ankle region affecting mainly the elderly female population with osteoporosis [3, 4].
The injury can be classified according to Danis Weber, and the AO/OTA classification systems [5, 6].
The aim of treatment is to early return the patient to their pre-injury functional activity. The incidence of these fractures is increasing over the last few decades. In 2002, Kannus noted a three hundred percent rise in the last 30 years [7]. The time of surgery is a significant risk factor for complication like wound break down, wound edge necrosis, superficial and deep infection and post traumatic osteoarthritis [8]. It has been approved that the rate of these complications increased to 12.9% if the surgery is delayed compared to 3.6% with early surgery [8].
The patient general and local conditions, fracture pattern, surgical time frame and the surgeon experience contributed to the outcome. In August 2016, The British Orthopaedic Association introduced an Audit Standard for Trauma (BOAST) related to the management of ankle fractures and this has been used as a benchmark for this study. The study looked to determine whether adherence to the standard has improved early outcomes for patients.
Method
This study included all the fixable ankle fractures, that fulfilled the BOAST guidelines criteria, who were admitted at Queens Burton Hospitals between October 2018 to October 2019 and compared them with the group admitted between August 2015 to August 2016, a year before publishing the guidelines.
Hours from the time of presentation to the accident and emergency department to the time of surgery have been calculated. The aim of the project was to check whether we were complying with the British Orthopaedic Association Audit Standards for Trauma (BOAST) guidelines, in regard to, the early fixation role which is recommended to be on the day or day after injury.
We have retrospectively reviewed and analyzed the electronic notes of patients. Computerized medical record system (Meditech V6, PACS) was used for data collection and reviewing the x-rays. Pilon, open fractures, skeletally immature patients and patients more than 60-year-old were excluded. Ankle fractures were classified anatomically and according to Danis-Weber classification. Data related to time frame from presentation to fixation was collected with the possible cause of ankle fixation delay as well.
Results
Between October 2018-19, 73 ankle fractures were admitted to Queens Hospital Burton. Forty-four patients fulfilled the study inclusion criteria. Eighteen males with average age of 39.3 years old (range from 20-60) and 26 females with average age of 42.2 years old (range from 18- 58).
Twenty-nine ankles (66%) were fixed on the day or day after injury while 5 ankles (11%) had the surgery within 48 hours. Five patients (11%) were operated between 3 to 4 days of presentation because they required medical optimization while 5 patients (11%) were operated between 6 and 10 days due to soft tissue swelling.
Regarding the 29 patient who undergone fixation within the day or the day after injury, 11 patients (38%) had Weber B fractures, 8 patients (28%) had Weber C fractures, 7 patients (24%) had Weber A fractures and 3 patients (10%) had Trimalleolar ankle fracture. While the 5 cases fixed within 48 hours were divided into; 2 Weber B, 2 Weber C and 2 trimalleolar fractures. So, 77.2% of our admitted patients with fixable ankle fractures had their surgery within 48 hours of admission.
Between August 2015-16, 37 patients fulfilled the study inclusion criteria. Twenty-one males with average age of 37.8 years old (range from 18-57) and 16 females with average age of 42.1 years old (range from 22-60).
Twenty-one ankles (56.7%) were fixed on the day or day after injury while 8 ankles (21.6%) had the surgery within 48 hours. Two patients (5%) were operated on 5 days due to swelling while 6 patients (16%) were operated after 7 days due to required medical optimization or failed conservative treatment. Regarding the 21 patient who undergone fixation within the day or the day after injury, 5 patients (24%) had Weber B fractures, 5 patients (24%) had Weber C fractures, 1 patient (4.5%) had trimalleolar ankle fracture, 9 (43%) patients had bimalleolar ankle fractures and 1 (4.5%) patient had an isolated medial malleolar fracture. So, 79% of our admitted patients with fixable ankle fractures had their surgery within 48 hours of admission.
A high BMI, above 30 as per the World Health Organization (WHO), was recorded in many patients, but was not a contributing factor of fixation delay which was mainly due to the soft tissue oedema. The ankle fracture pattern and complexity did not affect the delay of fixation; on the contrary many complex ankle fractures were good to be fixed within 48 hours.
Majority of the patients who required ankle fixation were operated on within the proposed time frame recommended by the BOAST guidelines.
A similar cross site study was done at Royal Derby Hospital, showed at a 6 months period that 52% of the patients underwent fixation on the day or day after the injury [6] (Figure 1).
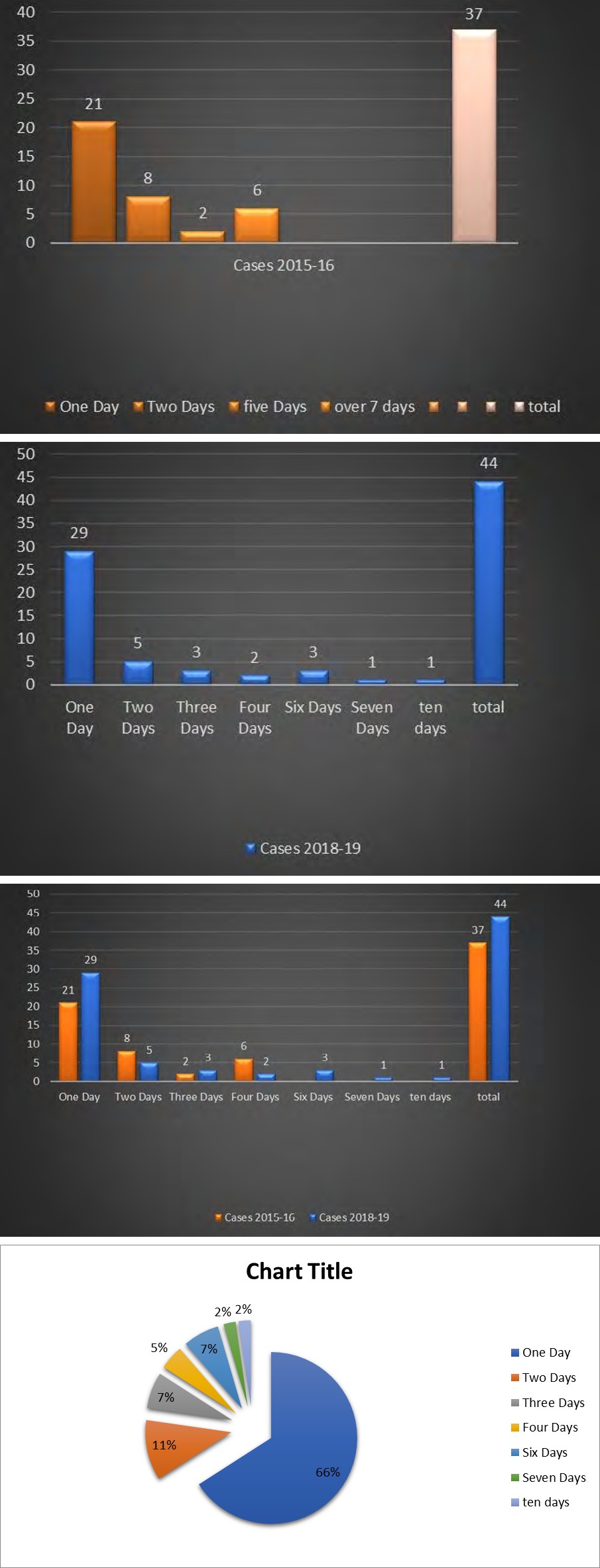
Days to Surgery 2018-2019
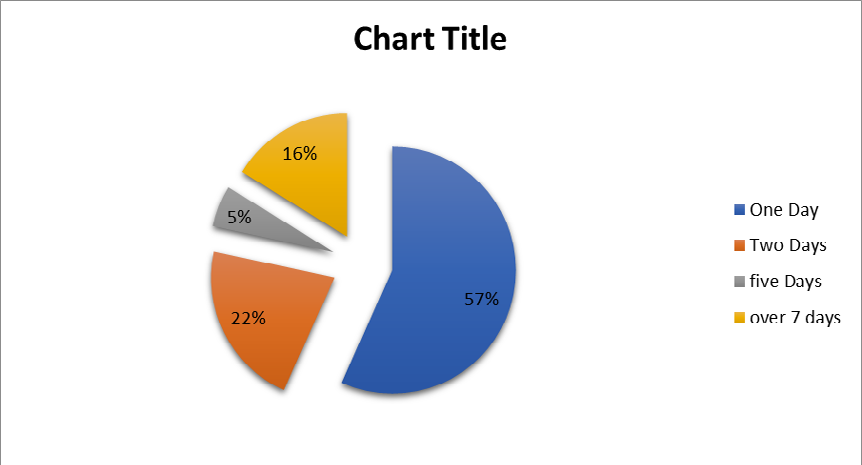
Days to Surgery 2015-2016 Figure 1: Results of Cross site study at Royal Derby Hospital.
Discussion
One of the biggest questions about ankle fractures are, whether to admit the patients or send them home and bring them on the day of the surgery. Patients’ compliance with strict elevation to reduce the swelling and making it ready for surgery is variable. Admitting the patient on the day of the injury will be the wisest approach to achieve adequate elevation which is at or above the level of the heart aiming to minimize the soft tissue swelling and to avoid the related post-operative complications like wound break down, wound edge necrosis or superficial and deep infection.
Reduction and splinting should be performed urgently for clinically deformed ankles. Radiographs should be obtained before reduction unless this will cause an unacceptable delay. Adequate reduction must be confirmed by review of repeat radiographs and documented before transfer from ED. If the reduction is not satisfactory and a talar shift still seen, a repeat of the reduction and plastering must be done as was advised in the BOAST guidelines.

At the district hospitals in the UK, the main obstacle to admit the patients who need ankle fixation in a district general hospital is the bed availability. During the winter pressure times, most of the beds in the wards including the surgical wards are occupied by medically unwell patients. During the Covid time, it was advised to send the fit and healthy patients who need surgery home and to bring them back to have their surgeries in the treatment centre where they can be admitted and discharged at the same time.
Conclusion
The study showed that the BOA recommendations for the ankle fractures, regarding the time frame from injury to surgery within the day or the day after injury, has achieved good results in 78% of cases with ankle fractures regardless the fracture type. Authors recommend that ankle cases to be admitted directly from the ED with strict antioedematous measures to enable the surgery within the defined time frame. This help to achieve better short- and long-term results and decrease the hospital stay (Figure 2).

References
-
Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: a review. Injury 37(8): 691-697.
-
Juto H, Nilsson H, Morberg P (2018) Epidemiology of Adult Ankle Fractures: 1756 cases identified in Norrbotten County during 2009–2013 and classified according to AO/OTA. BMC Musculoskelet Disord 19(1): 441.
-
Kannus P, Palvanen M, Niemi S, Parkkari J, J¨arvinen M (2002) Increasing number and incidence of low-trauma ankle fractures in elderly people: Finnish statistics during 1970-2000 and projections for the future. Bone 31(3): 430-433.
-
Thur C, Edgren G, Jansson K, Wretenberg P (2012) Epidemiology of adult ankle fractures in Sweden between 1987 and 2004: a population-based study of 91,410 Swedish inpatients. Acta Orthop 83(5): 276-281.
-
Audigé L, Bhandari M, Kellam J (2004) How reliable are reliability studies of fracture classifications? A systematic review of their methodologies. Acta Orthop Scand 75(2): 184-194.
-
D. Morris, E. Fitzpatrick, R. Rajan (2019) Ankle fractures – An audit of BOAST 12 guidelines. Journal of Orthoplastic Surgery [S.l.] 2(2): 209227233
-
Bengner U, Johnell O, Redlund-Johnell I (1986) Epidemiology of ankle fracture 1950 and 1980. Increasing incidence in elderly women. Acta Orthop Scand 57(1): 35-37.
-
Schepers T, De Vries MR, Van Lieshout EM, Van der Elst M (2013) The timing of ankle fracture surgery and the effect on infectious complications; A case series and systematic review of the literature. International Orthopaedics (SICOT) 37(3): 489-494.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results