Congenital Oblique Talus Spontaneous Reduction-Case Report
Congenital oblique talus is a very rare condition which presents as an isolated deformity or in association with neuromuscular and/or genetic disorders. Pathoanatomically the deformity shows a dislocated talonavicular and subtalar joint. The ethiology and pathogenesis are still not finally determined, although in some cases a genetic basis has been identified. The clinical picture is that of a flat longitudinal arch. Clinical diagnosis is confirmed by plain radiographic imaging of anteroposterior and lateral views. Congenital oblique talus should not be confused with other deformities of the foot, such as congenital vertical talus, which with stress view X-Ray can be reduced. The object of treatment of congenital oblique talus is to restore a normal anatomical relationship between the talus, navicular bone and calcaneus. Good early results of modified non-operative treatment using serial manipulations, physiotherapy, special shoes or cast treatment may change therapeutic concepts.
Background
Congenital oblique talus has Idiopathic ethiology; most of the patients have spina bifida, arthrogryposis multiplex, congenital or chromosomal abnormality (trisomy 18) and neuromuscular abnormalities or diseases [1, 2, 3].
Jaya Kumar and Ramsey in 1977 highlighted the differential diagnosis between oblique talus and vertical talus and how to make reduction. Treatment of congenital oblique talus by non-operative treatment using serial manipulation, stretching, cast treatment and minimally invasive surgery (Ponseti Method by percutaneous cut of Achilles tendon) may change therapeutic concepts [2, 3].
A mild variant of vertical talus is congenital oblique talus. This variant is characterized by the same clinical deformities as seen in vertical talus, but they are less rigid or lax [2, 4, 5].
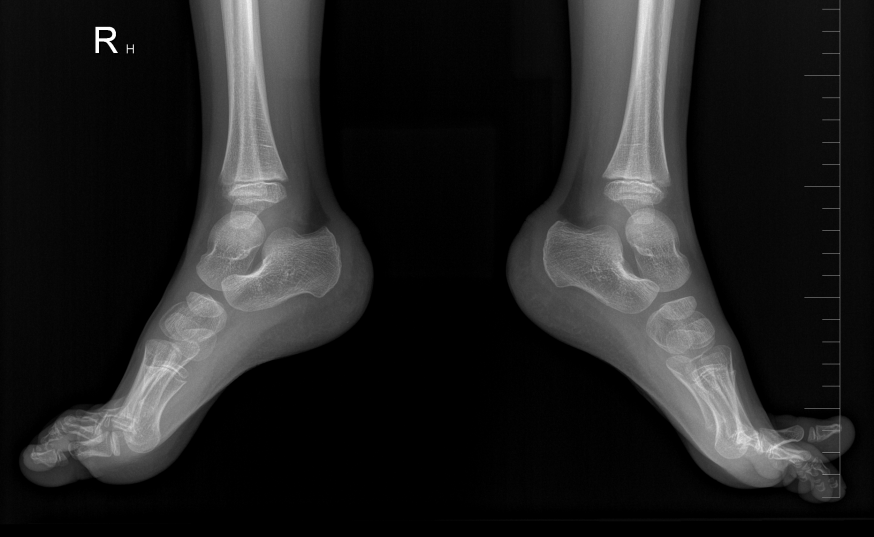
A 2 years and 4 months old male child with abnormal gait came to paediatric orthopaedic clinic with referral from paediatrician, no previous medical illness, physical examinations shows that he is walking on the balls of the feet or toe walking, dorsal flection in the right ankle is 80 degrees and in the left ankle 90 degrees, no pain, no swelling, no redness, without neurovascular deficit. X-Ray was done for both ankles and it shows bilateral oblique talus but in the right side had worse finding (Figure 1). Special shoes were prescribed and physiotherapy began.
Total number of 4 special shoes were prescribed and he went to physiotherapy for 3 circuits each one of 10 visits (60 minutes per visit) with exercises to stretch the foot and improve flexibility. Passive mobilisation, of the talocrural joint by a high proximal grip, passive stretching of anterior tibial and fibular muscles, Reflex stimulation of pronator muscles, realignment of the cuneometatars joint by passive manipulation, passive stretching of medial foot muscles. Physiotherapist put the lower limb in basic position, then in middle position of the hip joints (only allow light flexion), the knees are also in light flexion and the ankle joints at right angle as well. We prevent rotation, abduction, adduction and passively stretched muscles that are kept relaxed or in the middle position.
Massage of plantar foot and anterior aspect of all tibia. Then the physiotherapist did passive movements to the fullest extent possible, but not through pain. Exercises to maintain freedom of movement are performed 5-7 times and where we need to release movement in the joint, physiotherapist increase the number to 10-15 times. Physiotherapist and parents repeat them several times a day. Then ankle plantar flexion and forefoot inversion, place one hand on patient’s flexed knee. Grasp the heel of patient’s foot with the other hand. Physiotherapist gently pushes the foot down and inwards, stretching as much as possible. Start with five repetitions and work up to 40 repetitions.
Relaxation is needed after training and massage. During lockdown caused by COVID-19 exercises were performed at home without controlled physiotherapy or appointment in our paediatric orthopaedic clinic and percutaneous Achilles tendon tenotomy wasn’t provided due to lockdown.
After two and half years X-Ray check was done and showed the normal position of talus and normal gait (Figure 2). The Patient is still in dispensary.

Conclusion
Sometimes minimal surgical intervention will be needed (Ponseti method). Good early results of modified non-operative treatment using serial manipulations, physiotherapy, special shoes or cast treatment may change therapeutic concepts.
Conflict of Interest Statement
Author declares that the research was conducted in the absence of any commercial or financial relationship that could be considered as a potential conflict of interest.
Contribution Statement
The author confirms contribution to the paper as follows: study conception and objectives of paper; Author reviewed the results and approved the final version of the manuscript.
Funding
No funding.
Declarations
We confirm that all methods were carried out in accordance with relevant guidelines and regulations. We confirm that:
- All methods were carried out in accordance with relevant guidelines and regulations.
- Informed consent was signed by the parent.
Acknowledgment
We thank the staff of paediatric orthopaedic clinic in university hospital, which helped us in this study.
References
-
Harris EJ (2000) The oblique talus deformity. What is it, and what is its clinical significance in the scheme of pronatory deformities. Clin Podiatr Med Surg 17(3): 419-442.
-
MILLER M (2012) Review of Orthopaedics. In: 6th (Edn.), Philadelphia: Saunders, 896 s. ISBN 9781437720242.
-
Vojtaššák J (2006) Ortopédia a Traumatológia. Bratislava: SAP, 576 s. ISBN 80-89104-95-9.
-
Arbab D, Rath B, Quack V, Lüring C, Tingart M (2013) Talus verticalis: Aktuelle Diagnose-und Therapieoptionen Vertical talus: current diagnostic and therapy options. Orthopade 42(6): 402-408.
-
Alaee F, Boehm S, Dobbs MB (2007) A new approach to the treatment of congenital vertical talus. J Child Orthop 1(3): 165-174.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results