Extra Periosteal Sliding Plate, a New Surgical Technique for the Treatment of Fractures of the First Metacarpal and Proximal Phalanx
Background: One of the most important objectives when performing an open reduction of a fracture is to achieve a stable internal fixation with minimal damage of the periosteum to preserve irrigation in the fracture site and thus promote adequate healing. Minimally Invasive plate osteosynthesis (MIPO) follow this key technical point with great effectiveness and efficiency, however, a reduction technique with these characteristics for the management of hand fractures has not yet been widely described for the management of hand fractures. Methods: The authors technique proposes a new surgical technique “extra-periosteal sliding plate” fixation for first metacarpal and proximal phalanx fractures. Data are obtained from 9 patients from June 2022 to January 2023 and a threemonth postoperative follow-up is performed where functionality and rehabilitation results are evaluated. Results: In total nine patients underwent to the described technique achieving adequate fracture stability and total bone healing with favorable functional outcomes without sequelae. Conclusion: Extra-periosteal sliding plate fixation is considered a great surgical option for the management of hand fractures, specially in those patients with severe trauma in whom vascular and soft tissue integrity must be preserved, providing suitable functional outcomes.
Introduction
Since the neolithic period in the stone age, evidence has been found that demonstrates the beginning of the use of tools for fracture management. Later, in ancient Greece and Rome they managed to improve these materials which are considered very similar to those found today. However, it was not until 1907 that Lambotee, et al. [1] established the term “osteosynthesis” where they speak about stable bone fixation. Then, Robert Danis succeeded in developing a plate for fracture fixation, achieving primary bone healing. By 1969, the AO (Arbeitsgemeinschaft für Osteosynthesefragen) was created with a broad development in the open reduction of fractures and the use of better quality osteosynthesis materials [2].
Complications associated with wide dissection and extensive periosteal removal to reach the fracture site were also evidenced and minimal invasive techniques that protect bone irrigation began to be contemplated. In 1995 the term minimally invasive plate osteosynthesis (MIPO) was popularized, which has been used to reduce trauma of the soft tissues and vascularization, in addition, induce secondary healing and reduce pain compared to traditional techniques [1].
Despite the effectiveness and efficacy showed in recent years with MIPO, its use has been limited to the humerus, clavicle, distal radius, femur, tibia, and calcaneus, without reports of the use of this technique in hand fractures. We present a series of 9 cases with proximal phalanx or first metacarpal fractures in which extra-periosteal sliding plate fixation was performed highlighting how the technique can be used in appropriately selected patients with outcomes comparable to standard techniques.
Methods
Between June 2022 to January 2023 nine men with proximal phalanx or first metacarpal fractures underwent to an extra-periosteal sliding plate fixation. An informed consent form was prepared explaining the technique and the virtues it was intended to demonstrate. Weekly assessment was performed for the first month and then every month until 3rd month to assess functional recovery, viability, complications, and hand rehabilitation according to the total active motion (TAM) classification system and thumb opposition was evaluated according to Kapandji score. The data were subsequently analyzed by means of a database using the SPSS statistical system.
Surgical Technique
All patients underwent for a fracture reduction and extra-periosteal sliding plate under local anesthesia as described by Lalonde, et al. [3, 4] without use of torniquet.
First Metacarpal
- A 5 mm incision in the radial dorsal aspect of the thumb at the metacarpal head, supraperiosteal proximal dissection along metacarpal.
- Careful dissection maintains periosteal bone union to ensure adequate vascularization at the fracture site.
- A 5 mm incision is made at the base of the metacarpal, identifying, and preserving the sensory branch of the radial nerve (Figure 1A).
- The osteosynthesis plate slid from distal to proximal, its length is measured and initially fixed with kirschner pin, and its position is verified under fluoroscopic vision.
- Extra-periosteal fixation is performed with locked and cortical screws in the base and head of the metacarpal, configuring a load bearing osteosynthesis construct.
- If necessary, neutralization osteosynthesis or simplification with cannulated screws can be performed.
- Minimal incision closure with non-absorbable monofilament 5/0.
Proximal Phalanx
- Two minimal skin incisions, proximal and distal of 5 mm was performed at the dorsal – lateral level of the proximal phalanx as approach (Figure 1B).
- Supraperiosteal dissection is performed preserving the integrity of the extensor mechanism, dissecting underneath it.
- After fracture reduction, sliding the condylar plate, making sure that is below of the extensor apparatus. Temporary fixation with kirschner pins is performed and verified by fluoroscopy
- Plate fixation is performed with locked screws achieving an adequate reduction of bone fragments.
- Minimal incision closure with non-absorbable monofilament 5/0.
Results
In this study, nine male patients with an average age of 29 years (20 -34), six thumb metacarpal fractures and three proximal phalanx fracture underwent reduction and extra- periosteal sliding plate fixation under local anesthesia with an average surgical time of 43 minutes. In 3 cases there was concomitant lesion of neurovascular structures that required surgical repair. There were no cases with functional impairment, an average recovery in functional active mobility (TAM%) of 100% was obtained as excellent or good according to Strickland criteria and six patients had a score of 10 points on the Kapandji score achieving adequate thumb opposition. All patients who underwent surgery achieved digital and hand functional recovery at the end of the 4th to 6th week of rehabilitation and were able to resume daily activity and work functions without any contraindication. The procedure and results of some cases of the study are described in Figures 2-5.
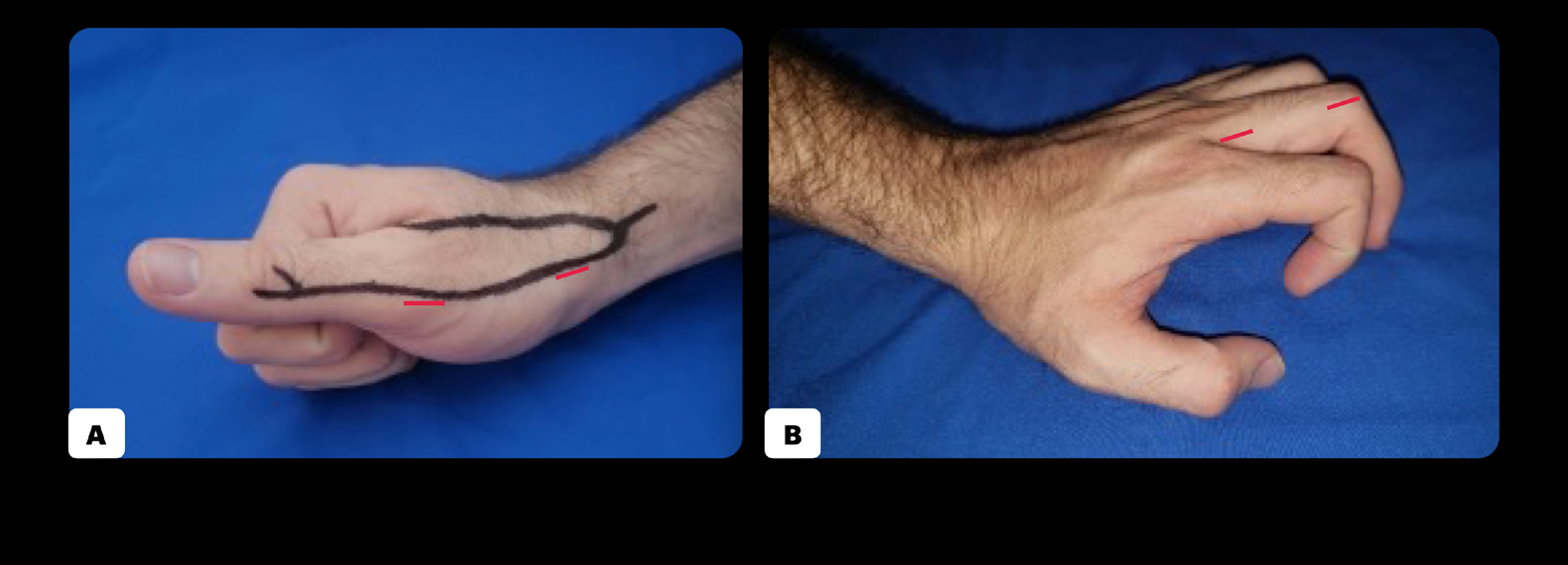
1A: 5 mm incisions in the dorsal radial aspect of the thumb preserving the sensory branch of the nerve. 1B: Minimal incisions, proximal and distal 5 mm, at the dorsal lateral level of the proximal phalanx. Figure 1: Minimal incision approach.
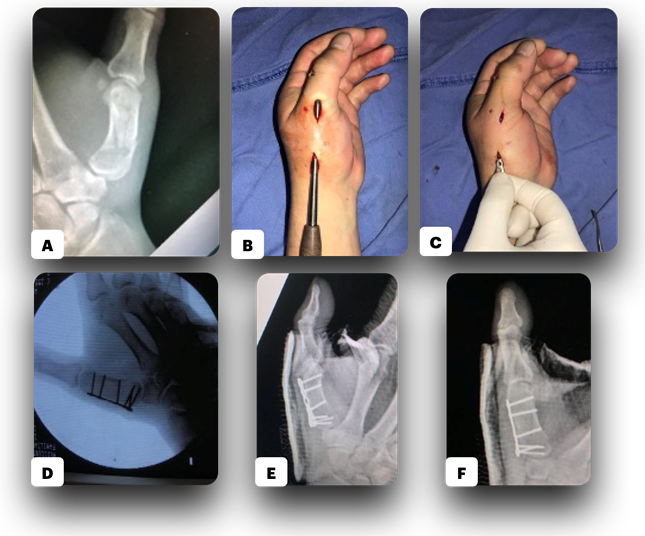
2A: Comminuted fracture of first metacarpal bone. 2B: Extra-periosteal dissection through the minimal incisions. 2C: Plate sliding and fixation. 2D: Adequate reduction and fixation under fluoroscopy. 2E, F: Immediate pop definitive radiograph showing adequate reduction and fixation of fracture. Figure 2: Thumb metacarpal fracture reduction and fixation in young male.
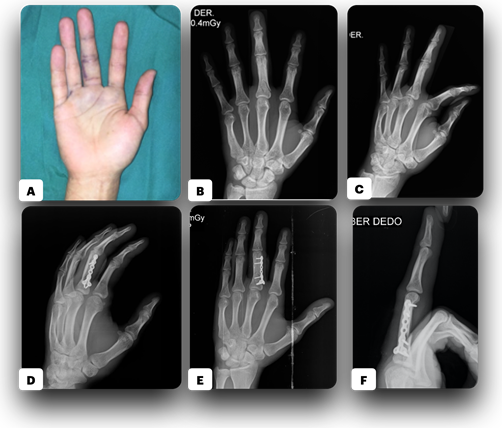
3A: Malrotation, edema and ecchymosis on the third finger. 3B, C: X-ray shows comminuted fracture of the base and diaphysis of proximal phalanx. 3D-F: Final X-ray showing adequate reduction and fixation of fracture with a sliding plate. Figure 3: 25 years old patient with blunt trauma on third finger – right hand.
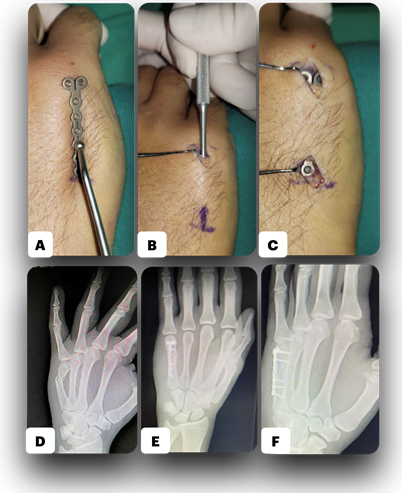
4A: Plate selection and future position. 4B: Extra-periosteal dissection through the minimal incisions. 4C: Plate sliding and fixation. 4D: Previous X-ray with a spiral and comminuted fracture of the neck of the fifth metacarpal bone with diaphysis extension. 4E, F: Fourth week X-ray showing adequate consolidation progress and stable fixation. Figure 4: Patient with high blunt trauma on the hand at fifth metacarpal area.
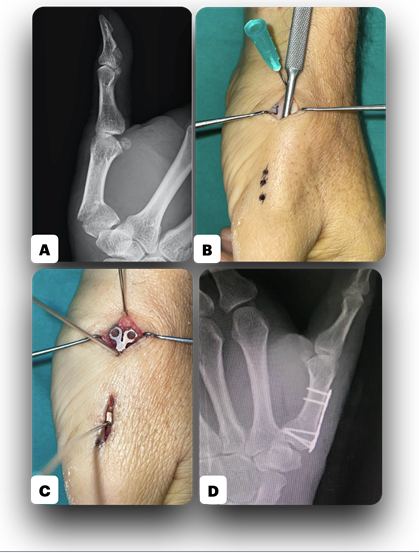
5A: Extra-articular first metacarpal bone fracture. 5B: Extra-periosteal dissection through the minimal proximal and distal incisions, minimizing periosteal damage. 5C: Plate sliding and fixation. 5D: Adequate reduction and fixation after 6 weeks. Figure 5: Thumb metacarpal fracture reduction and fixation.
Discussion
In hand trauma, metacarpal fractures represent up to 40% and a quarter of them refer to the fifth metacarpal fracture also known as “boxer´s fracture” [5]. For phalanx fractures, open fractures with different degrees of soft tissue loss and associated complications are frequently found. When they are closed fractures, up to 26% go unnoticed. Based on the characteristics of the fracture and the patient, preservative or surgical management is considered, either with kirschner pins, osteosynthesis plates or screws. Despite today’s state-of-the-art technology and very satisfactory functional results there are still many aspects to be improved and complications to be avoided. As described previously, a case of open reduction with internal fixation with plates, it was considered that to achieve an ideal anatomical reduction to the fracture site should be widely exposed, but this in turn generates damage to the periosteum and alteration in bone vascularization increasing infection, malunion or non-union rates. Krettek, et al. describe a less invasive surgical approach for femur fractures sliding the osteosynthesis plate in the submuscular plane at the lateral edge with adequate stability fixation, coining the term minimally invasive percutaneous plate osteosynthesis (MIPPO), then modified to MIPO [6].
This technique has become popular globally in the last ten years for fractures of the femur, humerus, clavicle, distal radius, tibia, and calcaneus achieving lower rates of infections, malunion, non-union, avascular necrosis with minimal incisions and better pain control. Xue, et al. conducted a cadaver study comparing minimally invasive osteosynthesis technique open reduction in humeral fractures and its effect on vascular integrity. Their study concludes that MIPO technique is superior to standard approach of open reduction and internal fixation in preserve vascular and periosteal tissue at the fracture site [7].
We consider that MIPO with extra-periosteal sliding plate in hand fractures is a superior technique compared to the gold standard management with less bone loss, neurovascular, periosteal and soft tissue injury which promotes an adequate and faster consolidation with lower complications rates and shorter surgical time, those outcomes are correlated with those studies in humerus fractures showing better results and fewer complications as well as lower rates of infection and non-union [8, 9]. For distal tibia fractures, favorable results have been reported in the literature with the MIPO technique in terms of high healing percentages, decreased malalignment and lower complications rates with respect to the surgical wound and excellent functional outcomes providing structural stability [10, 11, 12, 13].
Minimally invasive osteosynthesis has proven to be superior in many aspects compared to the conventional technique of open reduction and internal fixation and no evidence of studies on hand trauma. In the present case series, metacarpal and proximal phalanx fractures were reduced and fixated with the previously described technique, achieving adequate fracture stability and healing in 100% of the patients. Extra-periosteal sliding plate fixation is considered a great surgical option for the management of hand fractures, especially in those patients with severe trauma in whom vascular and soft tissue integrity must be preserved, providing suitable functional outcomes. Its use in clinical practice is a field for future research and publications.
References
-
Toogood P, Huang A, Siebuhr K, Miclau T (2018) Minimally invasive plate osteosynthesis versus conventional open insertion techniques for osteosynthesis. Injury 49 (S1): S19-S23.
-
Van de Wall BJM, Beeres FJP, Knobe M, Link BC, Babst R (2021) Minimally invasive plate osteosynthesis: An update of practise. Injury 52(1): 37-42.
-
Lalonde DH, Martin AL (2013) Wide-awake flexor tendon repair and early tendon mobilization in zones 1 and 2. Hand Clin 29(2): 207-213.
-
Lalonde DH (2017) Conceptual origins, current practice, and views of wide awake hand surgery. J Hand Surg Eur 42(9): 886-895.
-
Haughton D, Jordan D, Malahias M, Hindocha S, Khan W (2012) Principles of hand fracture management. Open Orthop J 6: 43-53.
-
Krettek C, Schandelmaier P, Miclau T, Tscherne H (1997) Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral fractures. Injuryn 28(S1): A20-30.
-
Xue Z, Jiang C, Hu C, Qin H, Ding H, et al. (2016) Effects of different surgical techniques on mid-distal humeral shaft vascularity: open reduction and internal fixation versus minimally invasive plate osteosynthesis. BMC Musculoskelet Disord 17(1): 370.
-
Falez F, Papalia M, Carbone S, Teti A, Favetti F, et al. (2019) Low complication rates in Minimally Invasive Plate Osteosynthesis (MIPO) for proximal humeral fractures at 5 years of follow-up. Injury 50(S2): S34-S39.
-
Hohmann E, Glatt V, Tetsworth K (2016) Minimally invasive plating versus either open reduction and plate fixation or intramedullary nailing of humeral shaft fractures: a systematic review and meta-analysis of randomized controlled trials. J Shoulder Elbow Surg 25(10): 1634-1642.
-
Collinge C, Protzman R (2010) Outcomes of minimally invasive plate osteosynthesis for metaphyseal distal tibia fractures. J Orthop Trauma 24(1): 24-29.
-
Ahmad MA, Sivaraman A, Zia A, Rai A, Patel AD (2012) Percutaneous locking plates for fractures of the distal tibia: our experience and a review of the literature. J Trauma Acute Care Surg 72(2): E81-87.
-
Paluvadi SV, Lal H, Mittal D, Vidyarthi K (2014) Management of fractures of the distal third tibia by minimally invasive plate osteosynthesis - A prospective series of 50 patients. J Clin Orthop Trauma 5(3): 129- 136.
-
Van Nguyen L, Nguyen GN, Nguyen BL, Bui HM (2021) Results and complications of minimally invasive medial plate osteosynthesis for distal metaphyseal tibial fractures: A prospective case series from Vietnam. Ann Med Surg (Lond) 70: 102886.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results