Stripe Wear - Ceramic on Polyethylene Bearing Surface: A Case Report
Background: Stripe wear is a well-known phenomenon that might be caused by rim impingement, edge loading, metal particle entrapment, micro-separation, and transient subluxation. Stripe wear is felt to represent metal transfer and has been associated with squeaking in ceramic-on-ceramic bearings. In our paper, we report the presence of stripe wear on a retrieved modular ceramic femoral head from a patient with ceramic-on-polyethylene-bearing total hip arthroplasty. Method: We report a case of a 57-year-old male who originally had metal-on-metal (MOM) THA and underwent debridement and exchange of the bearing surface from MOM to ceramic-on-polyethylene (COP) articulation for pain and metallosis. He subsequently developed sepsis and underwent resection arthroplasty. Result: Intraoperatively, a cross-table lateral radiograph revealed the forward flexion of the acetabular component and femoral neck to posterior acetabular margin impingement. By analyzing the retrieved components macroscopically and microscopically, linear scars were found on the polyethylene liner, femoral neck, and femoral head in a pattern consistent with the X-ray finding. Conclusion: If metallosis is encountered after THA, the source of the metal wear should be identified. Component malposition is a possible cause, and the surgeon should consider revision or repositioning of the components if evidence of impingement is seen, as a simple bearing exchange may not solve the problem. This report indicates that stripe wear is not limited to ceramic on ceramic articulations.
Introduction
Ceramic hip bearings were introduced in the 1970s as an alternative to metal-on-polyethylene bearings due to their increased hardness, wettability, improved wear, and decreased coefficient of friction and bioreactivity [1, 2, 3]. Improved wear characteristics have been demonstrated in many clinical and in vitro studies, but the complications include fracture of the bearing, acoustic phenomena, and stripe wear. Stripe wear is a well-known phenomenon that is felt to represent metal transfer and has been associated with squeaking in ceramic-on-ceramic bearings [4, 5, 6].
Ceramic head on polyethylene liner bearing surfaces were introduced to prevent the complications associated with ceramic-on-ceramic bearings. There are several studies on follow-up results and complications of the ceramic-on- polyethylene bearing surface [7, 8]. In this paper, we report the presence of stripe wear on a retrieved modular ceramic femoral head (Biolox Delta, Depuy, Warsaw, Indiana, USA) from a patient with ceramic-on-polyethylene-bearing total hip arthroplasty.
Case Report
A 57-year-old male (height: 71 inches, weight: 205 lbs.) underwent an uncemented total hip arthroplasty (Summit femoral component and Pinnacle acetabular component, Depuy, Warsaw, Indiana, U.S.A.) using a metal-on-metal articulation (a 36-mm cobalt chrome alloy femoral head with a 36-mm cobalt chrome alloy metal liner, Ultamet, Depuy) by another surgeon for treatment of osteoarthritis of the hip. Five months following his primary surgery, he returned to his orthopedic surgeon with complaints of continued pain in his groin, which did not improve with conservative measures. Aspiration of the hip was performed, which revealed cloudy fluid. He then underwent exploration of the hip joint with irrigation and debridement at 6 months post index arthroplasty. Intraoperative findings revealed “black pigmentation” around the lining of the hip joint. Cultures grew Staphylococcus epidermidis in broth only. Based on intra- operative findings, the surgeon indicated that the condition could be consistent with a “metal-on-metal hypersensitivity reaction.” 3 months following the hip exploration (9 months following the index procedure), the patient continued to have debilitating pain, and the surgeon elected to revise the hip joint to exchange the metal-on-metal bearing. Revision surgery involved re-debridement and an exchange of the bearing surface from a metal-on-metal articulation to a ceramic femoral head (Biolox Delta, Depuy, Warsaw, Indiana, USA) on a highly cross-linked polyethylene liner (Marathon, Depuy, Warsaw, Indiana, USA) articulation. The surgeon’s operative note did not mention evidence of impingement or damage to the uncemented tapered femoral component or the acetabular shell. Therefore, these components were left in situ. Moderately turbid amber joint fluid was encountered, and the fluid was sent for cell count with differential, which revealed a total leukocyte count of 3804 cells per cubic millimeter, and 78% were neutrophils. Final intraoperative cultures produced no bacterial growth. No tissue sections were sent from the surgery.
The patient returned for follow-up six weeks after his second revision surgery with a draining sinus from his hip. He was subsequently referred to our institution for further treatment. Clinical examination and laboratory analysis suggested a deep prosthetic infection. Aspiration of the hip joint, under fluoroscopic control revealed frank purulent material. Cultures revealed a polymicrobial infection, and the patient underwent resection arthroplasty. The intra- operative findings revealed a slight thickening of the pseudocapsule but no remarkable hypersensitivity reaction or synovial hyperplasia. Prior to the extraction of implants, precise marking of the implant at the anterior, posterior, medial, and lateral sites was done. The components were carefully retrieved to prevent damage to the articular surface and were cleaned with normal saline. The retrieved implants were a 36-mm ceramic head (Depuy, Warsaw, Ind), uncemented tapered femoral stem (Summit, Depuy, Warsaw, Ind), uncemented titanium hemispheric acetabular shell (Pinnacle, Depuy, Warsaw, Indiana), and an unlipped 36-mm cross-linked polyethylene liner (Marathon, Depuy, Warsaw, Ind). Histological analysis showed no lymphocytic response in the periprosthetic tissues to suggest a hypersensitivity response. The retrieved components were analyzed macroscopically and under a dissecting microscope. On the acetabular shell, metal abrasion was observed on the external border of the rim over the postero-superior aspect. Examination of the polyethylene liner revealed impingement marks on the postero-superior aspect of the liner rim (Figure 1).
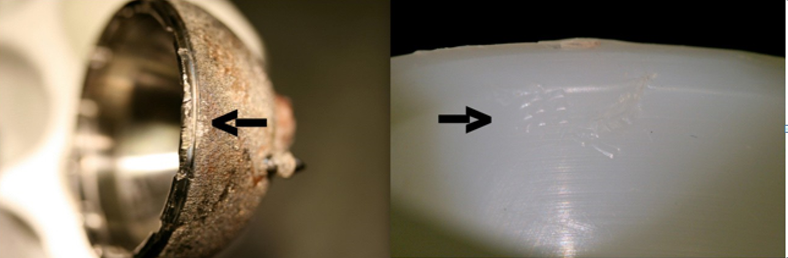
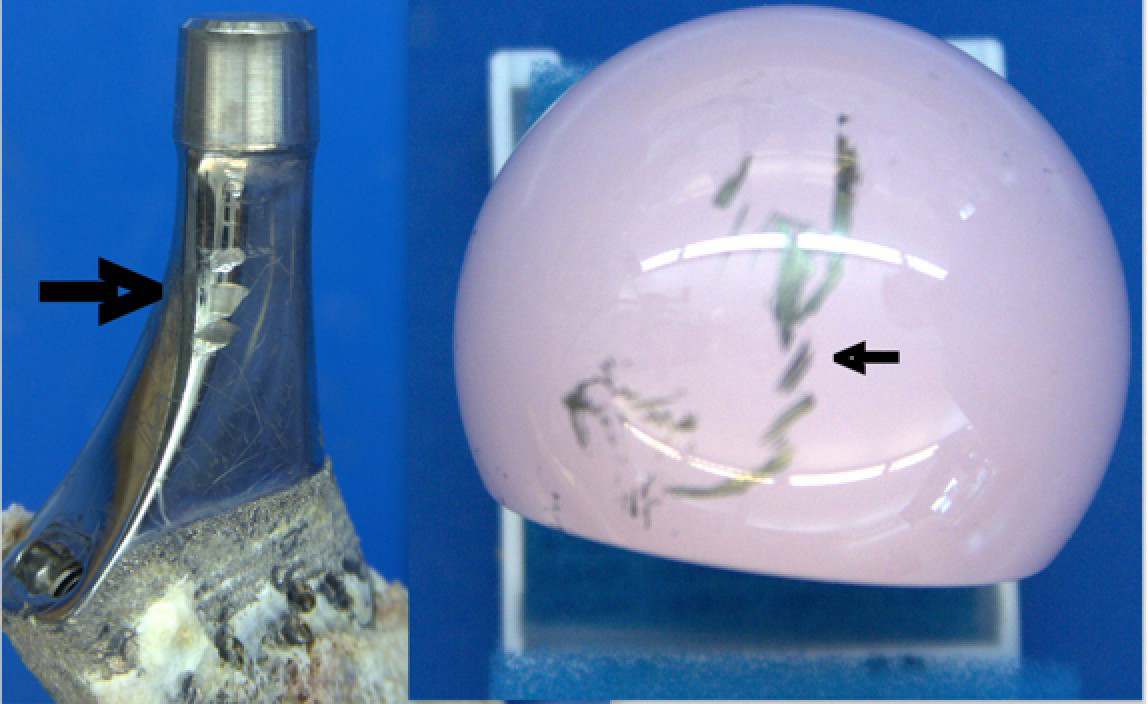
There were linear scars on the posterior aspect of the femoral neck oriented in a vertical direction, consistent with neck impingement against the rim of the shell. A wear scar in the form of a black stripe was also seen on the antero- superior aspect of the femoral head (Figure 2). The stripe wear noted was peripheral in the retrieved femoral head, and the direction was from antero-superior to antero-inferior. This suggested possible superior edge loading, giving rise to an anteverted stripe scar on the femoral head. Prior to resection arthroplasty, the tapered femoral component was well positioned in the femoral canal without evidence of radiolucency or migration. A cross-table lateral radiograph revealed the forward flexion of the acetabular component and the femoral neck to posterior acetabular margin impingement.
Discussion
Stripe wear has been described in conjunction with ceramic-on-ceramic bearing surfaces [9, 10, 11]. Multiple reasons include rim impingement, edge loading, metal particle entrapment, micro-separation, and transient subluxation. Walter, et al. studied the mechanism of stripe wear on sixteen third-generation alumina-on-alumina bearings. Their analysis showed that the majority of stripe wear was caused by edge loading when the hip was flexed, as when rising from a sitting position or climbing stairs [4, 11]. A hip simulator study comparing hip implants with micro- separation vs. non-separation mode revealed that stripe wear could be caused by micro-separation of the bearing surface during the swing phase of walking and subsequent edge loading with heel strike [10, 12]. Another hip simulator study by Neavolos [13] showed that transient subluxation could be a possible cause of stripe wear. Yamamoto, et al. found no stripe scars on the load-bearing surfaces of three ceramic-on-ceramic hips, but they did find stripe scars at the rim of the alumina inlay without any indentations on the acetabular rim or femoral neck. According to them, the femoral head separated from the acetabular component and contacted the rim of alumina, which gave rise to stripe wear. They concluded that the femoral head can separate from the socket without neck-socket impingement [14]. Studies have also shown that a malpositioned cup leads to high stress on the femoral head and edge of the acetabulum, resulting in stripe wear. Walter, et al. suggested that impingement between the femoral neck and the metal acetabular rim leads to the generation of metal debris. Metal debris can get in between the bearing surface and act as a third body wear, thereby giving rise to stripe wear [4]. Catonne Y, et al. reported revision of metal-on-metal THA failure and conversion to ceramic-on-ceramic delta alumina inserts and femoral heads for osteolysis, impingement, and macroscopic metallosis. Their preoperative and intraoperative findings showed osteolysis, radiolucenies, impingement, and severe metallosis in the majority of cases [15]. Willert, et al. termed the abnormal response seen in a series of metal-on-metal total hip replacements an aseptic lymphocytic-dominated vasculitis associated lesion (ALVAL) and suggested that this was due to a Type IV hypersensitivity response, and this has been supported by other authors [16, 17, 18].
The black pigmentation seen in the periprosthetic tissues in this case implies metal-on-metal wear. If encountered, the surgeon should make every effort to understand the source of the metal wear. Surgeons should consider component malposition as a possible cause in this instance and should consider revision or repositioning of the components if they find evidence of impingement wear, as a simple bearing exchange may not solve the problem. The pattern of stripe wear and impingement marks seen in our case suggests that metal debris could have caused stripe wear. In our study, the bearing surface of the hip was changed from metal on metal to ceramic on polyethylene. The intra-operative findings, radiographs, and analysis of the retrieved implant suggested impingement of the femoral neck on the acetabulum, which likely produced metal debris as well as micro-separation of the femoral head from the polyethylene liner [19].
However, we cannot be sure when the metal particles were generated (during the metal-on-metal articulation or during the ceramic-on-poly articulation). As the metal liner margin sits flush with the acetabular shell, unlike the polyethylene liner margin, the likelihood of femoral neck to socket impingement and the production of metal wear are higher when metal-on-metal articulation was in-situ.
Even though there were increased numbers of metal particles in the synovium from the initial surgery, we would expect them to produce a more diffuse pattern of metal deposition on the ceramic femoral head. Therefore, any revision hip arthroplasty involving metallosis requires thorough irrigation and debridement followed by a complete synovectomy to decrease the metal particle burden as much as possible. Also, in this situation, repositioning the acetabular component should be considered if impingement scars are seen on the neck of the femoral prosthesis. It certainly appears that metal-on-metal bearings are less tolerant of component malposition than metal-on-polyethylene bearings. If bearing surfaces are changed in revision surgery, the surgeon should make sure that there is no intra-articular or extra-articular impingement.
It is not known if stripe wear on a ceramic femoral head will increase polyethylene wear on its bearing couple, but the presence of a third body within the articulation certainly suggests that wear would be accelerated. Further studies are required to determine the prevalence of stripe wear in ceramic-on-polyethylene bearing surface.
Conclusions
This case report indicated that stripe wear is not limited to ceramic on ceramic articulations. Therefore, during THA revision secondary to metallosis, it is essential to perform thorough irrigation and debridement, complete synovectomy, and the source of the metal wear should be identified. Component malposition is a possible cause, and the surgeon should consider revision or repositioning of the components if evidence of impingement is seen, as a simple bearing exchange may not solve the problem.
Conflicts of Interest
N/A
Acknowledgements
N/A
Funding
N/A
References
-
Boutin P, Christel P, Dorlot JM, Meunier A, Roquancourt AD, et al. (1988) The use of dense alumina-alumina ceramic combination in total hip replace- ment. J Biomed Mater Res 22(12): 1203-1232.
-
Ueno M, Ikeuchi K (2001) Wear properties of ceramic total hip prosthesis made of alumina and zirconia. Jpn Soc Clin Biomech.
-
Ueno M, Ikeuchi K (2003) Investigation of the wear properties of ceramic total hip prostheses made of alumina and zirconia combination: A hip simulator study. In Proceedings of the Key Engineering Materials 240-241: 806-812.
-
Restrepo C, Parvizi J, Kurtz SM, Sharkey PF, Hozack WJ, et al. (2008) The Noisy Ceramic Hip: Is Component Malpositioning the Cause. Journal of Arthroplasty 23(5): 643-649.
-
Taylor S, Manley MT, Sutton K (2007) The Role of Stripe Wear in Causing Acoustic Emissions From Alumina Ceramic-On-Ceramic Bearings. Journal of Arthroplasty 22(7S3): 47-51.
-
Walter WL, Insley GM, Walter WK, Tuke MA (2004) Edge loading in third generation alumina ceramic-on-ceramic bearings: Stripe wear. Journal of Arthroplasty 19(4): 402-413.
-
Saito M, Saito S, Ohzono K, Takaoka K, Ono K (1992) Efficacy of alumina ceramic heads for cemented total hip arthroplasty. Clin Orthop Relat Res 283: 171-177.
-
Sugano N, Nishii T, Nakata K, Masuhara K, Takaoka K (1995) Polyethylene sockets and alumina ceramic heads in cemented total hip arthroplasty. A ten-year study. J Bone Joint Surg Br 77(4): 548-556.
-
Barrack RL, Burak C, Skinner HB (2004) Concerns about ceramics in THA. Clin Orthop Relat Res 429: 73-79.
-
Manaka M, Clarke IC, Yamamoto K, Shishido T, Gustafson A, et al. (2004) Stripe Wear Rates in Alumina THR - Comparison of Microseparation Simulator Study with Retrieved Implants. J Biomed Mater Res B Appl Biomater 69(2): 149-157.
-
Walter WL, Otoole GC, Walter WK, Ellis A, Zicat BA (2007) Squeaking in Ceramic-on-Ceramic Hips. The Importance of Acetabular Component Orientation. Journal of Arthroplasty 22(4): 496-503.
-
Nevelos J, Ingham E, Doyle C, Streicher R, Nevelos A, et al. (2000) Microsepara- tion of the centers of alumina- alumina artificial hip joints during simulator testing produces clinically relevant wear rates and patterns. Journal of Arthroplasty 15(6): 793-795.
-
Nevelos JE, Ingham E, Doyle C, Nevelos AB, Fisher J (2001) Wear of HIPed and non-HIPed alumina-alumina hip joints under standard and severe simulator testing conditions. Biomaterials 22(16): 2191-2197.
-
Yamamoto T, Saito M, Ueno M, Hananouchi T, Tokugawa Y, et al. (2005) Wear analysis of retrieved ceramic-on- ceramic articulations in total hip arthroplasty: Femoral head makes contact with the rim of the socket outside of the bearing surface. J Biomed Mater Res B Appl Biomater 73(2): 301-307.
-
Catonné Y, Lazennec JY, Nogier A, Fourniols E, Masson B (2006) Revision strategy after metal on metal THR failure: Conversion to ceramic on ceramic. Bioceramics and Alternative Bearings in Joint Arthroplasty 1-4.
-
Hallab NJ, Caicedo M, Finnegan A, Jacobs JJ (2008) Th1 type lymphocyte reactivity to metals in patients with total hip arthroplasty. J Orthop Surg Res 3: 1-6.
-
Korovessis P, Petsinis G, Repanti M, Repantis T (2006) Metallosis after contemporary metal-on- metal total hip arthroplasty: Five to nine-year follow-up. Journal of Bone and Joint Surgery 88(6): 1183-1191.
-
Willert HG, Buchhorn GH, Fayyazi A, Flury R, Windler M, et al. (2005) Metal- on-metal bearings and hypersensitivity in patients with artificial hip joints: A clinical and his- tomorphological study. J Bone Joint Surg Am 87(1): 28- 36.
-
Schüller HM, Marti RK (1990) Ten-year socket wear in 66 hip arthroplasties: Ceramic versus metal heads. Acta Orthop 61(3): 240-243.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results