The Use of Bone Hook in the Retrieval of Tibial Bony Cut. Technical Tip
Total ankle replacement, is technically demanding. Intraoperative malleolar fracture may result because of levering on the malleoli whilst removing the distal tibial cut. The technique described of using bone hook to retrieve the distal tibial bone cut is safe and easy.
Introduction
Despite the constantly increased number of replaced ankles, Total ankle replacement remains a technically significant demanding procedure. To date, numerous clinical studies have demonstrated a long learning curve associated with this procedure [1]. Intraoperative complications included fractures and malpositioning of components. Instrumentation for ankle arthroplasty was fairly crude, requiring a fair amount of free-hand technique.
The aim of this paper is to share the experience of using bone hook to retrieve distal tibial bone cut, which makes this difficult step, safe and easier.
Technique
Distal tibial cut in total ankle arthroplasty is performed with guidance of the jigs and intraoperative X-rays. The piece of bone cut is in-between the two malleoli, it is attached posterior to the capsule and soft tissue. The manual of different ankle arthroplasty techniques advice using osteotomies, rangers, or other surgical instruments, to remove all resected tibia bone. Notes Caution is given is that is pressure is applied to either the internal surfaces of the medial malleolus or lateral malleolus, this may cause fracturing. This fracturing would be increased if either of these surfaces are notched by aggressive cutting of the tibia. Often the piece of bone is split to take out in pieces, attempts to remove the resected bone in one piece is extremely difficult and impossible [2]. Levering instruments to remove the bone, can fracture the malleoli, and should be avoided. Pituitary ranger and laminar spreader can help.
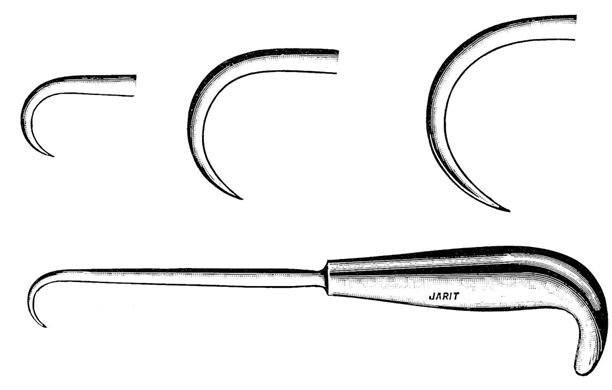
The use of blunt bone hook passed gently behind the posterior part of the resected tibia and slow pulling the bone in forward direction, does not require levering on malleoli and is safe. This can be helped using pair of Kocher’s and jolting movement to disrupt the capsular attachment in the back (Figure 1).
Discussion
The most common reasons for intraoperative fractures include extensive and inaccurate use of saw blade in combination with limited visualization, insufficient instrumentation, and improper sizing of Prosthesis Component. The incidence of the intraoperative malleolar fractures is given between 10% and 38% in the current literature. The overall rate of the intraoperative malleolar fractures may decrease with increasing surgeon experience [3].
References
-
Barg A, Saltzman CL (2014) Ankle replacement. In: Coughlin M, Saltzman CL, et al. (Eds.), Surgery of the Foot and Ankle. Philadelphia, USA, pp: 1078-1162.
-
Valderrabano V, Barg A (2014) Complications after Total Ankle Replacement. In: James K, Orio D, et al. (Eds.), Total ankle replacement an operative manual. LWW, pp: 100-115.
-
Lee KB, Cho SG, Hur CI (2008) Perioperative complications of HINTEGRA total ankle replacement: our initial 50 cases. Foot Ankle Int 29(10): 978-984.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results