Association of Hip Geometry with Proximal Femoral Fracture in Elderly Population
Introduction: Hip fractures are a significant global health concern, particularly among the elderly population, with increasing incidence rates predicted in the coming decades. Although different factors like age-related osteoporosis, alcoholism, smoking, high BMI are established causes of hip fracture but none can fully explain the cause of hip fracture. Proximal hip geometry (HAL. FNAL, FNA, FHD, FND) may be associated with hip fracture and is under investigation with conflicting reports. Method: Our study is X-ray based prospective case-control study aiming to evaluate the association of hip geometry parameters with proximal femoral fractures in elderly population. We conducted study involving 102 subjects, including 34 cases with proximal femoral fractures and 68 controls. Various hip geometry parameters were calculated, tabulated and compared to see the difference in hip parameters among fractured and non-fractured group. Additionally, we calculated the mean and standard deviation among male and female subjects and compared between them Result: Our study revealed differences in HAL and FNAL between the case and control groups, suggesting their potential role as risk factors for proximal femoral fractures. However, no significant differences were observed in NSA, FHD, and FND between the two groups. Gender-wise analysis showed significant differences in HAL, FNAL, FHD, and FND between males and females, possibly due to variations in height among them. Conclusion: This study contributes to the understanding of hip fracture risk factors in the elderly population and underscores the importance of considering hip geometry parameters in fracture risk assessment. Larger studies are recommended to further validate these findings.
Introduction
Fractures around Hip are common and comprise 20% of the operative workload of an orthopedic trauma unit globally Thesis [1]. The lifetime risk of a person of sustaining a hip fracture lies within the range of 40% to 50% in women and 13% to 22% in men. The global number of hip fractures is expected to increase from 1.26 million in 1990 to 4.5 million by the year 2050 [2]. In Asia It has been estimated there will be 2.28-fold increase in incidence of hip fracture form 2018 (1,124,060 cases) to 2050 (2,563,488 cases) [3].
Age related osteoporosis is an established cause for proximal femoral fracture but neither age-related osteoporosis nor the increased risk of falling sufficiently explain the exponential increase in the incidence of hip fracture in the elderly, much research has focused on proximal femoral geometry [4]. Studies have showed that proximal femur geometry is a significant factor for hip fracture [5]. Longer femoral axis length (FAL) may increase the impact energy caused by a fall, and thus a longer hip axis length (HAL) may be related to the occurrence of hip fracture.
We conducted case-control study in Patan Hospital and Nepal Orthopedic Hospital to compare the hip geometry parameters (Femoral neck diameter, Neck shaft angle, Hip Axis Length, Femoral Axis Length, Femoral Head Diameter) in the (fractured) study and the (non-fractured) control group. Additionally, we aimed to find out the gender-wise difference in hip geometry parameters in males and females.
Methods
After obtaining ethical approval from IRC PAHS Prospective Observational Analytical Study (Case-Control Study) study was conducted from January 2022 to January 2023. The sampling technique used was Purposive Non- Probability Sampling.
Sample size with a case-to-control ratio of 1:2 was calculated to be 34 and 68 respectively with a mean difference formula about an Indian study by Patel, et al. [5].
| Gender | Case | Control | |
|---|---|---|---|
| Neck of Femur fracture | Intertrochanteric fracture | ||
| Male | 8 | 9 | 36 |
| Female | 9 | 8 | 32 |
| 17 | 17 | ||
| Total | 34 | 68 |
Table 1: Number of control and cases with neck and intertrochanteric fractures with gender.
| Age group | Cases | Control |
|---|---|---|
| 51-60 years | 6 | 8 |
| 61-70 years | 13 | 20 |
| 70-80 years | 10 | 22 |
Table 2: Table showing the distribution of cases and control according to age.
| Cases (34) | Control(68) | P value | Significance | |
|---|---|---|---|---|
| HAL (cm) | 11.4882±0.90700 | 11.0231±0.89621 | 0.016 | Significant |
| FNAL(cm) | 10.032±0.8988 | 9.6265±0.7264 | 0.015 | Significant |
| FHD(cm) | 5.0168±0.4150 | 5.0318±0.4188 | 0.865 | Not significant |
| NSA (degree) | 129.9265±4.02718 | 130.0735±3.61306 | 0.852 | Not significant |
| FND | 3.3324±0.4093 | 3.3524±0.3583 | 0.801 | Not significant |
Table 3: Analysis of all HAL, FNAL, FHD, FND and NSA (mean± SD) between cases and controls.
| Cut off value | Specificity | Sensitivity | AUC | 95% CI | |
|---|---|---|---|---|---|
| HAL | 11.24 | 0.647 | 0.691 | 0.67 | 0.557-0.785 |
| FNAL | 9.51 | 0.735 | 0.529 | 0.65 | 0.528-0.761 |
Table 4: ROC Analysis of HAL and FNAL.
| Male (50) | Female (52) | P value | Significance | |
|---|---|---|---|---|
| HAL (cm) | 11.471±0.880 | 10.897±0.880 | 0.001 | Significant |
| FNAL(cm) | 9.9704±0.7681 | 9.05637±0.80067 | 0.01 | Significant |
| FHD(cm) | 5.2046±0.42522 | 4.8558±0.3279 | 0 | significant |
| NSA (degree) | 130.280±3.98912 | 129.7788±3.4988 | 0.501 | Not significant |
| FND | 3.4470±0.3900 | 3.2483±0.3340 | 0.007 | Significant |
Table 5: Analysis of all HAL, FNAL, FHD, FND and NSA (mean ± SD) between male and female.
Patients above 50 years with a diagnosis of Intertrochanteric (IT) and Neck of Femur (NOF) fracture were included in the case group. However, all cases with high-energy trauma, Pathological fractures, with preexisting deformities around the hip and thigh, having osteoplastic or osteoplastic lesions seen in the measurement site of the proximal femur, inadequate radiograph and not willing to participate in study were excluded.
For controls and gender-matched (+/- 2 years) patients above 50 years with no radiographic evidence of the current or past hip fracture were considered.
Measurement was taken on AP views taken in 15°-20° internal rotation using Radiant DICOM viewer in the normal side of case (fractured) group and in right side for the control group.
After data collection statistical analysis was performed using EPI Info V7.2.2.2, Microsoft Excel, and Easy software. Descriptive statistics were presented using frequencies with percentages for categorical variables, while mean and standard deviation were used for continuous variables. The association between the measured variables was analyzed using unpaired Student T-tests to obtain t-values. The significance level was set at a probability value of 0.05 for all the aforementioned statistical tools.
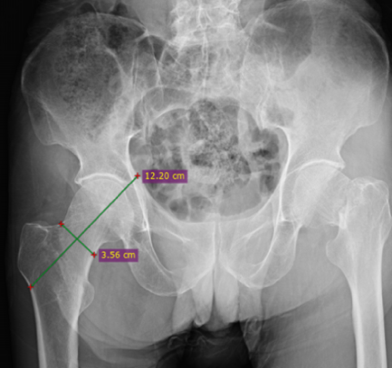
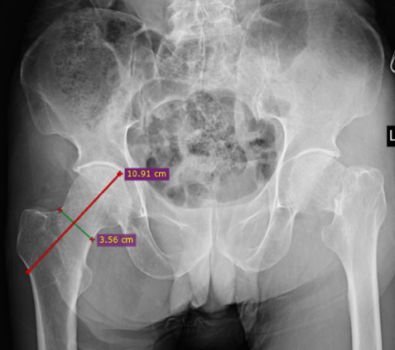
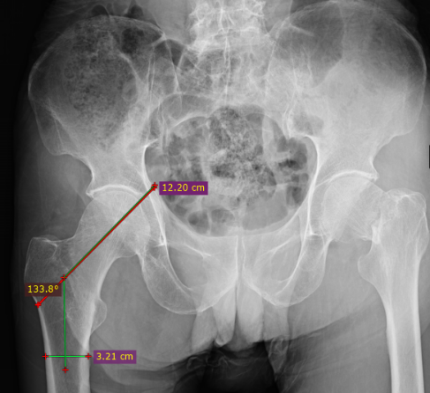
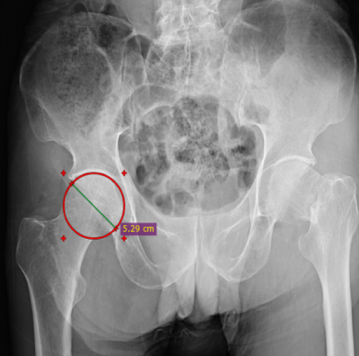
Measurement
Hip Axis Length: A line drawn that is perpendicular to a line drawn at the narrowest portion of the neck, medially passes through the center of the head up to the inner pelvic table and laterally to the outer cortex of the femur. Femoral neck diameter: Shortest distance between the outer-superior edge of the femoral neck and the lateral cortex of the medial-inferior margin. Femoral Neck Axis Length: A line drawn that is perpendicular to a line drawn at the narrowest portion of the neck, medially passes through the center of the head up to the tip of the head and laterally to the outer cortex of the femur (base of Greater Trochanter). Neck shaft angle: It is the angle between a line along the anatomical axis of the shaft of femur and the anatomical axis of the neck. Femoral Head Diameter: It is the diameter of the superimposed circle of particular diameter over the head of Femur Field.
Result
Our study consisted of 102 subjects 34 in the case group and 68 in the control group.
The mean age of the studied population was 70.47 years, median of 71 and mode of 70 years.
The mean age in fracture group was 68.64 years and in study population was 71 years.
Highest number of patient were in age group 61 to 70 years.
We calculated the mean value and standard deviation to the mean for each variable for both cases as well as controls. Using t test we carried out the p-value for each parameter and observed that p- value less than 0.005 was observed in HAL (p value 0.016) and FNAL (p value 0.015) as shown in table 3.
ROC analysis of HAL and FNAL was done as tabulated in table 4. Mean and standard deviation was calculated for each variable for male and female and there was statistical difference in terms of HAL (p-value 0.001), FNAL (p-value 0.010), FHD (p-value 0.000) and FND (p-value 0.007). However, there was no significant difference in terms of NSA (p-value 0.501)
Discussion
The occurrence of hip fractures in the elderly is related to multiple factors, including age-related osteoporosis, increased tendency to fall, coexisting diseases, and poor nutritional status etc [6]. The mechanical properties of bone at the tissue level are determined by the structure of the bone and the quality of the bone. It is necessary to evaluate the structural anatomy of the bone to predict the fracture pattern and incidence. It has been well established that a significant role is played by the geometrical configuration and the bio-material characteristics in providing strength to a structure. But this has shown inconsistency [7].
Various sections of the femoral neck can function as cantilever beams, playing a role in enhancing the strength of the proximal femur. The stress on the proximal femur resulting from a fall shows a positive correlation with five factors: longer femoral neck length, the greater force of the fall, and a smaller cross-sectional area of the femoral neck. Consequently, a longer hip axis length of the proximal femur may be associated with an increased likelihood of experiencing a hip fracture [8].
In our study the mean age of the studied population was 70.47 years, the median of 71 and mode of 70 years. The mean age in the fracture group was 68.64 years and in the study population was 71 years. However Ahuja et al reported a mean age of 62 years in Indian population [9]. However the life expectancy of both countries is comparable. Small number of sample size usually from urban area presenting to a tertiary center might have caused this difference.
The case group had a higher mean hip axis length (HAL) of 11.4882 ± 0.90700 compared to the control group with 11.0231 ± 0.89621, showing a statistical difference (p = 0.016). This increased HAL in the case group may contribute to fractures. Our findings align with studies by Patron, et al. [10], Deboeuf, et al. [11], and Giovanni, et al. [12], as well as Karlsson, et al. [13], Leslie, et al. [14], and G. I am, et al. [15]. However, Amit J Patel, et al. [5] and Gnudi, et al. [16] found no HAL association.
In a 2017 meta-analysis by Jonny Karunia Fajar et al. [7] on hip geometry and femoral neck fractures, HAL was associated with fractures (OR = 1.53, p = 0.025), but the study did not consider factors like age, ethnicity, and gender affecting HAL measurements.
In the case group, the femoral neck axis length (FNAL) was 10.0362 ± 0.898, while in the control group, it was 9.6365 ± 0.726, with a p-value of 0.015, indicating a significant difference. This increased FNAL in the case group may contribute to fractures.
Our finding for FNAL was supported by Peacock, et al. [17], who found that combining hip geometry (HAL and FNAL) with bone mineral density improved hip fracture discrimination. Kaissi, et al. [18] also showed that increased FNAL is associated with femoral neck fractures.
However, studies by Dincel, et al. [19], Stephen Kaptoge, et al. [20], and IM Gi, et al. [15] found no association between hip fracture and FNAL. In a meta-analysis by Fajar et al, [7] no significant association was found between FNAL and femoral neck fractures [odds ratio (OR) 95% confidence interval (CI) = 0.36, p-value = 0.117].
In our study, the Neck Shaft Angle (NSA) showed no significant difference between the case and control groups (p = 0.852). This aligns with findings from Peacock, et al. [17] and Jun Han, et al. [21] who also found no association between NSA and hip fractures. However, other studies suggest NSA is linked to hip fractures, including a recent meta-analysis by Fajar, et al. [7] reporting a significant association (OR = 1.47, p = 0.044).
In our study, there was no statistical difference in Femoral Neck Diameter (FND) between the case and control groups (p = 0.865). This aligns with findings from Im GI, et al. (retrospective) [15], Dincel, et al. [19] (cross-sectional), and Peacock et al17, which showed no association of proximal femoral fracture with hip geometry.
However, several studies, including those by Karlsson [13], Kaissi [18], and Han J, et al. [21], suggest a strong association between FND and proximal femoral fractures. A meta-analysis by Fajar, et al. [7] revealed that elevated FND was associated with the risk of femoral neck fractures (OR = 2.68, p < 0.001). Specifically, a one-millimeter increase in FND correlated with a 31% rise in the odds of femoral neck fracture and a 22.9% increase in the odds of intertrochanteric fracture. This suggests FND plays a crucial role in determining the likelihood of both types of fractures, possibly due to its correlation with osteoporosis and overall femur dilatation associated with aging [22].
Significant differences were observed in hip parameters (HAL, FNAL, FHD, and FND) between males and females, likely influenced by the height disparity. Nepali men have an average height of 163 cm compared to 150.8 cm for women, impacting hip parameter sizes as these values vary with body size. This height difference may explain the statistical disparities observed. However, no significant difference was noted in neck shaft angle (NSA) between genders. This study has several limitations as it had non-randomization in case selection. We utilized only two-dimensional (2D) but CT scans could offer a three-dimensional view of the affected areas, allowing for a more comprehensive analysis and a better understanding of the fractures extent and severity.
In our study neck of femur fracture and intertrochanteric fracture were not assessed separately but would be better if evaluated differentially.
Conclusion
An increase in HAL and FNAL could increase the possibility of sustaining a fracture and screening the potential patient with risk fracture can be identified and preventive measures can be taken. But as the sample size was small larger sample is recommended to conclude this finding.
References
-
Singer BR, McLauchlan GJ, Robinson CM, Christie J (1998) Epidemiology of fractures in 15,000 adults: the influence of age and gender. The Journal of Bone and Joint Surgery British 80(2): 243-248.
-
Melton LJ, Kearns AE, Atkinson EJ, Bolander ME, Achenbach SJ, et al. (2009) Secular trends in hip fracture incidence and recurrence. Osteoporos Int 20(5): 687- 694.
-
Cheung CL, Ang SB, Chadha M, Chow ESL, Chung YS, et al. (2018) An updated hip fracture projection in Asia: The Asian Federation of Osteoporosis Societies study. Osteoporosis and Sarcopenia 4(1): 16-21.
-
Ulusoy H, Bilgici A, Kuru O, Sarica N, Arslan S, et al. (2008) A new value of proximal femur geometry to evaluate hip fracture risk: True moment arm. HIP International 18(2): 101-107.
-
Patel AJ, Gandhi MV (2021) A radiological study of proximal femoral geometry and its relationship with hip fractures in Indian population. Int J Orthop Sci 7(2): 428- 435.
-
Alekel DL, Mortillaro E, Hussain EA, West B, Ahmed N, et al. Lifestyle and biologic contributors to proximal femur bone mineral density and hip axis length in two distinct ethnic groups of premenopausal women. Osteoporos Int 9(4): 327-338.
-
Fajar JK, Taufan T, Syarif M, Azharuddin A (2018) Hip geometry and femoral neck fractures: A meta-analysis. Journal of Orthopaedic Translation 13: 1-6.
-
Yang RS, Wang SS, Liu TK (1999) Proximal Femoral Dimension in Elderly Chinese Women with Hip Fractures in Taiwan. Osteoporosis International 10(2): 109-113.
-
Ahuja K, Sen S, Dhanwal D (2017) Risk factors and epidemiological profile of hip fractures in Indian population: A case-control study. Osteoporosis and Sarcopenia 3(3): 138-148.
-
Patron MS, Duthie RA, Sutherland AG (2006) Proximal femoral geometry and hip fractures. Acta Orthop Belg 72(1): 51-54.
-
Szulc P, Duboeuf F, Schott AM, Dargent-Molina P, Meunier PJ, et al. (2006) Structural determinants of hip fracture in elderly women: re-analysis of the data from the EPIDOS study. Osteoporos Int 17(2): 231-236.
-
Iolascon G, Moretti A, Cannaviello G, Resmini G, Gimigliano F (2015) Proximal femur geometry assessed by hip structural analysis in hip fracture in women. Aging Clin Exp Res 27(S1): 17-21.
-
Karlsson KM, Sernbo I, Obrant KJ, Redlund-Johnell I, Johnell O (1996) Femoral neck geometry and radiographic signs of osteoporosis as predictors of hip fracture. Bone 18(4): 327-330.
-
Leslie WD, Pahlavan PS, Tsang JF, Lix LM, Manitoba Bone Density Program (2009) Prediction of hip and other osteoporotic fractures from hip geometry in a large clinical cohort. Osteoporos Int 20(10): 1767-1774.
-
Im GI, Lim MJ (2011) Proximal hip geometry and hip fracture risk assessment in a Korean population. Osteoporos Int 22(3): 803-807.
-
Gnudi S, Ripamonti C, Lisi L, Fini M, Giardino R, et al. (2002) Proximal Femur Geometry To Detect and Distinguish Femoral Neck Fractures from Trochanteric Fractures in Postmenopausal Women. Osteoporosis International 13(1): 69-73.
-
Peacock M, Turner CH, Liu G, Manatunga AK, Timmerman L, et al. (1995) Better discrimination of hip fracture using bone density, geometry and architecture. Osteoporos Int 5(3): 167-173.
-
El-Kaissi S, Pasco JA, Henry MJ, Panahi S, Nicholson JG, et al. (2005) Femoral neck geometry and hip fracture risk: the Geelong osteoporosis study. Osteoporos Int 16(10): 1299-1303.
-
Dincel VE, Sengelen M, Sepici V, Cavusoglu T, Sepici B (2008) The association of proximal femur geometry with hip fracture risk. Clin Anat 21(6): 575-580.
-
Kaptoge S, Beck TJ, Reeve J, Stone KL, Hillier TA, et al. (2008) Prediction of Incident Hip Fracture Risk by Femur Geometry Variables Measured by Hip Structural Analysis in the Study of Osteoporotic Fractures. J Bone Miner Res 23(12): 1892-1904.
-
Han J, Hahn MH (2016) Proximal Femoral Geometry as Fracture Risk Factor in Female Patients with Osteoporotic Hip Fracture. J Bone Metab 23(3): 175-182.
-
Michelotti J, Clark J (1999) Femoral Neck Length and Hip Fracture Risk. J Bone Miner Res 14(10): 1714-1720.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results