Does the Time taken to Remove the Syndesmosis Screw Influence the Onset of Tibiotalar Osteoarthritis
Introduction: Syndesmosis lesions are common in ankle trauma. They can be treated with screws (rigid fixation) or endobuttons (elastic fixation). When rigid fixation is chosen, the problem arises as to how long it should be removed, since according to some authors, prolonged retention of the screw can impair ankle biomechanics and lead to osteoarthritis in the long term. In our study, for various reasons, this screw was either removed at different times or remained in place. The aim of this study was to assess the impact of the time taken to remove the syndesmosis screw on the outcome of the ankle. Materials and method: We carried out a cross-sectional, analytical study with a retrospective and a prospective phase. Patients presenting with ankle trauma with syndesmostic lesion, without risk factors for osteoarthritis were included. Parameters such as age, sex, radiological analysis postoperatively and at the last follow-up, time to removal of the syndesmosis screw and AOFAS score for functional assessment. Data were analyzed using CS Pro7.5 software. Results: Eighty-one patients participated in the study. Mean age was 47.21 ±16.88. The majority were men, with a sex ratio of 1.38. All patients underwent surgical treatment with screw fixation of the syndesmosis. According to the time of screw removal, 02 were removed before 8 weeks, 20 between 8-12 weeks and 49 after 12 weeks. Assessment using the AOFAS score showed excellent results in 17 patients (21%), good results in 28 patients (35%), fair results in 27 patients (33%) and poor results in 9 patients (11%). The analysis between the time of screw removal and the onset of osteoarthritis showed signs of osteoarthritis beyond 12 weeks, with a rate of 44.4%. Conclusion: A syndesmosis screw left in place for more than 12 weeks increases the risk of osteoarthritis.
Introduction
Syndesmotic lesions are common in ankle trauma. Their incidence varies between 0.5 and 20%. They are often secondary to ankle dislocation or malleolar fractures [1, 2]. When associated with malleolar fractures, they are found in almost 40% of Weber B fractures and 80% of Weber C fractures [3]. When left untreated or inadequately treated, these syndesmotic lesions lead to pain and permanent ankle instability, ultimately resulting in osteoarthritis [4, 5, 6]. Several types of syndesmotic stabilization have been defined in the literature: Rigid fixation with screws and elastic fixation with pins or endo-buttons, but to date there is no consensus regarding the choice of type of fixation. Xu, et al. [7], Wang, et al. [8], report that elastic fixation in the treatment of acute syndesmosis lesions offers several advantages (better postoperative recovery of ankle function, low incidence of postoperative complications).
In our working environment, due to the unavailability of endo-buttons and their high cost, we have opted for cortical screw fixation, as it offers rigid stabilization and better healing of the syndesmosis. However, the question remains as to when the screw should be removed. Some authors believe that removal of the screw is not essential, as it generates additional financial costs and has no impact on the functional outcome of the ankle [9, 10]. Other authors, on the other hand, believe that if the syndesmosis screw remains in place beyond 12 weeks after ligament healing, ankle function will be impaired by the presence of unnecessary hardware [11]. Numerous studies have been reported in Africa on the epidemiological, clinical and therapeutic aspects of bi-malleolar fractures [12]. However, very little attention has been paid to syndesmosis lesions, which is why we undertook this study with the aim of assessing the impact of the delay in syndesmosis screw removal on the functional outcome of the ankle. Our working hypothesis was that timely removal of the syndesmosis screw improves the functional prognosis of the ankle with regard to the occurrence of osteoarthritis.
Materials and Method
Study Design: We conducted a descriptive and analytical cross-sectional study, with a retrospective and a prospective phase. It was a multicenter study conducted in three referral hospitals in the city of Yaoundé over a 5-year 3-month period from January 2018 to March 2023. Study Population: We included all consenting patients at least 18 years of age, operated on for ankle trauma with a screw- or pin-fixed syndesmosis lesion, and with a good SKINNER test on follow-up radiography. We excluded those with risk factors for ankle osteoarthritis (angular deviation of the lower limbs, associated tibial pilon fractures, and infections) and Weber A bi-malleolar fractures. The variables studied were sociodemographic (age, sex, socioeconomic level); radiographic (immediate postoperative films and films at final evaluation for analysis of consolidation and signs of osteoarthritis); and therapeutic (operative time; indication; time to removal of syndesmosis implants, occurrence of complications). Evaluation: After a mean follow-up of 2 years, patients were functionally assessed using the AOFAS score. Data Analysis: Data were analyzed using CS Pro 7.5 software. Qualitative variables were expressed as headcount and frequency; quantitative variables were presented as means (standard deviations) in the case of normal data distribution, or medians (range) in the case of asymmetric distribution. For comparison of quantitative variables, the Student’s T-test for independent data was used in the case of normal distribution, or the Mann Whitney-U test for non-parametric data. To compare qualitative data, the chi-square test or Fisher’s exact test was used. A p value ˂ 0.05 is considered statistically significant.
Results
Our Series: We identified 155 patients, 74 of whom did not meet our criteria. We retained 81 patients. The mean age was 47.21 ± 16.88 years, with extremes ranging from 19 to 86 years. The most affected population was the over-40s, i.e. 49 (60.5%). There were 47 men and 34 women, giving a sex ratio of 1.38. Bimalleolar fracture was the main etiology. According to the Danis and Weber classification, there were 52 (64%) Weber B fractures and 29 (36%) Weber C fractures. Therapeutic Features: All patients underwent osteosynthesis of the lateral malleolus with a third- tube plate or anatomical plate and rigid fixation of the syndesmosis with a 4.5mm or 3.5mm cortical screw, which was quadricortical in 34 cases and tricortical in 47 (Figure 1). No patient underwent endobutton syndesmesis. The majority of patients (72.8%) had their syndesmosis implant removed after 12 weeks (Table 1).
| Time to ablation screw (week) | Number (N) | Percentage (%) |
|---|---|---|
| < 8 | 2 | 2,5 |
| [8 - 12] | 20 | 24,7 |
| > 12 | 59 | 72,8 |
Table 1: Breakdown by time to mount removal.
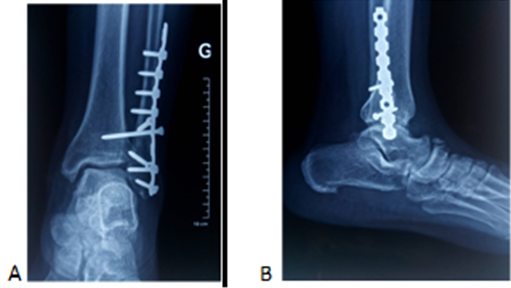
Note: A- Amtero-posterior View, B- Lateral view Figure 1: Osteosynthesis of a bimalleoar + fracture. Tricortical syndesmosis screw. Functional Results: Functional outcome based on the AOFAS score was excellent in 17 patients (21%) and good in
28 patients (35%), fair in 27 patients (33%) and poor in 9 patients (11%). Analysis of Occurrence of Osteoarthritis as a Function of Screw Removal Time (table 2): Of the 2 patients who had the screw removed before 8 weeks, none showed signs of osteoarthritis (P>0.05). Of the 20 patients who had the screw removed between [8, 9, 10, 11, 12] weeks, 5 showed signs of osteoarthritis, and at more than 12 weeks, 36 patients showed signs of osteoarthritis (Figure 2).
| Time to ablation screw (week) | Fate of the joint | P value | OR (IC à 95%) | |
|---|---|---|---|---|
| A- | A+ | |||
| < 8 | 2 (2,5) | 0 | 0,241 | |
| [8 - 12] | 15 (18,5) | 5 (6,2) | 0,008 | 4,32 (1,39 – 13,42) |
| > 12 | 23 (28,2) | 36 (44,4) | 0,002 | 0,18 (0,06 – 0,58) |
Table 2: Tibio-talar joint outcome as a function of time to ablation, with regard to the onset of osteoarthritis.
Note: A-: No signs of osteoarthritis A+: Presence of signs of osteoarthritis Table 2: Tibio-talar joint outcome as a function of time to ablation, with regard to the onset of osteoarthritis.

Note: A-Antero-posterior view, B- Lateral View Figure 2: Tibiotalar osteoarthritis after plate + screw removal at 3 years.
Discussion
Our study assessed the impact of the delay in syndesmosis screw removal on the outcome of the tibiotalar joint during surgical procedures performed on the traumatized ankle with syndesmotic lesion. The results show that late removal of syndesmosis screws has an impact on the occurrence of ankle osteoarthritis. However, it has the advantage of being a preliminary study that will serve as support for surgeons in our working environment. But it has the disadvantage of having a small sample size compared with European series, and of not having analyzed all the factors in syndesodesis that may influence the occurrence of long-term osteoarthritis.
All authors agree that bi-malleolar Weber B and C fractures are the main causes of syndesmosis lesions [12, 13]. Syndesmosis stabilization was performed using 4.5mm and 3.5mm cortical screws separately, depending on their availability on a patient-by-patient basis. In fact, the cortical screw is the reference implant for syndesmosis fixation, as it ensures rigid stabilization without distal tibio-fibular diastasis during loading on dynamic radiography [14, 15]. According to Tourné, et al., [16] there is no superiority in the choice of one screw over the other in terms of diameter, but the type of fixation (quadricortical or tricortical) may influence the medium- and long-term outcome of the ankle [16].
With regard to the time taken to remove the syndesmosis screw, 2 patients underwent surgery before 8 weeks, 20 patients between 8-12 weeks. This variation in duration in our study is due to the fact that in the first group, patients experienced discomfort with the syndesmosis screw, which would have precipitated its removal. In the second group, on the other hand, the surgeons wanted to comply with the recommendation to remove the screw between 6 and 12 weeks [16]. For economic reasons, and due to non-compliance with follow-up appointments, 59 patients (72.8%) had the osteosynthesis material removed after 12 weeks.
In terms of function, the AOFAS score was mostly good (between 80 and 89) in 34.6% of cases. The median AOFAS score was 80 [65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89], with a minimum of 30 and a maximum of 98. The onset of osteoarthritis was recorded in 41 patients (50.6%). Thus we find more or less equality between the occurrence and absence of osteoarthritis in our study population. A univariate analysis of the different patient groups showed no evidence of osteoarthritis in patients who underwent screw removal surgery at less than 8 weeks (P=0.241). On the other hand, in the group of patients operated on between 8-12 weeks, there were 5 cases with signs of osteoarthritis (6%) versus 15 (18.2%) who showed no sign of osteoarthritis (P= 0.008). The same was true for the third group of patients operated on at more than 12 weeks, who showed signs of osteoarthritis in 36 patients (44.4%) versus 23 patients (28.2%) who had no signs of osteoarthritis. But this difference was significant (P= 0.002). There is every reason to believe that the closer you are to the twelfth week with a syndesodesis screw still present in the ankle, the greater your risk of developing osteoarthritis. The fact that such a high proportion of patients did not develop osteoarthritis after 12 weeks is evidence that there are other factors to be taken into account in the development of osteoarthritis, which is why there is no consensus on the exact time frame for removal of the syndesodesis screw [17, 18, 19].
Our results differ from those reported by Klepacki, et al. [20] who report that radiological results are similar regardless of the time taken to remove syndesmosis screws [20]. Other factors influencing the onset of osteoarthritis include the presence of infra-radiological cartilage microlessions, often present in bi-malleolar fractures associated with dislocations, which can adversely affect the functional prognosis [21].
Conclusion
The repair of syndesmosis lesions is a controversial subject in terms of choice of implant type, technique and duration of fixation. In our study, we demonstrated that prolonged fixation beyond 12 weeks increases the risk of ankle osteoarthritis. For this reason, we recommend removal of the screw within 8-12 weeks, although this surgery is costly. However, further work will be undertaken to investigate the impact of screw size and number, and mode of fixation (quadri or tri cortical) on the outcome of a traumatized ankle with syndesmosis lesions.
References
-
Wuest T (1997) Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop 5 (3): 172-181.
-
Needleman RL, Skrade DA, Stiehl JB (1989) Effect of the syndesmotic screw on ankle motion. Foot Ankle 10: 17- 24.
-
Prediger B, Mathes T, Probst C, Pieper D (2020) Elective removal vs. retaining of hardware after osteosynthesis in asymptomatic patients a scoping review. Syst Rev 9(1): 225.
-
Zhang P, Liang Y, He J, Fang Y, Chen P, et al. (2017) A systematic review of suture-button versus syndesmotic screw in the treatment of distal tibiofibular syndesmosis injury. BMC Musculoskelet Disord 18(1): 286.
-
Li H, Chen Y, Qiang M, Zhang K, Jiang Y, et al. (2018) Computational biomechanical analysis of postoperative inferior tibiofibular syndesmosis: a modified modeling method. Comput Methods Biomech Biomed Engin 21(5): 427-435.
-
Amin A, Janney C, Sheu C, Jupiter DC, Panchbhavi VK (2019) Weight-Bearing Radiographic Analysis of the Tibiofibular Syndesmosis. Foot and Ankle Spec 12(3): 211-217.
-
Xu K, Zhang J, Zhang P, Liang Y, Hu JL, et al. (2021) Comparison of Suture-Button Versus Syndesmotic Screw in the Treatment of Distal Tibiofibular Syndesmosis Injury: A Meta-analysis. J Foot Ankle Surg 60(3): 555- 566.
-
Wang Q, Liu S, Wang Z, Li A, Ding JH (2024) Meta-analysis of elastic versus rigid fixation in the treatment of acute tibiofibular syndesmosis injury. Syst Rev BMC 13(1): 51.
-
Tucker A, Julia R, Kealey D, McDonald S, Stevenson M (2013) Functional outcomes following syndesmotic fixation: A comparison of screws retained in situ versus routine removal - Is it really necessary Injury 44(12): 1880-1884.
-
Khurana A, Kumar A, Katekar S, Kapoor D, Vishwakarma G, et al. (2021) Is routine removal of syndesmotic screw justified? Ameta-analysis. The Foot 49: 101776.
-
Kaftandziev I, Spasov M, Trpeski S, Zafirova-Ivanovska B, Bakota B (2015) Fate of the syndesmotic screw-search for a prudent solution. Injury 46 (6): S125-S129.
-
Ngo Yamben MA, Eone DH, Farikou I, Domra E, Guifo Ml, et al. (2017) Epidemiological, diagnostic and therapeutic aspects of bimalleolar fractures: Experience of a reference center in Cameroon: about 160 Cases. Algerian Journal of Medicine 25(5): 247-252.
-
Schepers T, Van Lieshout EMM, de Vries MR, Van der Elst M (2011) Complications of Syndesmotic Screw Removal. Foot Ankle International 32(11): 1040-1044.
-
Dingemans SA, Birnie MFN, Sanders FRK, van den Bekerom MPJ, Backes M, et al. (2018) Routine versus on demand removal of the syndesmotic screw; a protocol for an international randomised controlled trial (RODEO-trial). BMC Musculoskeletal Disorders 19(1): 35.
-
Kaftandziev I, Spasov M, Trpeski S, Zafirova-Ivanovska B, Bakota B (2015) Fate of the syndesmotic screw-Search for a prudent solution. Injury 46(S6): S125-S129.
-
Tourné Y, Molinier F, Andrieu M, Porta J, Barbier G (2019) Diagnosis and treatment of tibiofibular syndesmosis lesions. Orthopaedics & Traumatology: Surgery & Research 105(S8): S275-S286.
-
Fort NM, Aiyer AA, Kaplan JR, Smyth NA, Kadakia AR (2017) Management of acute injuries of the tibiofibular syndesmosis. Eur J Orthop Surg Traumatol 27(4): 449- 459.
-
Stiene A, Renner CE, Chen T, Liu J, Ebraheim NA (2019) Distal Tibiofibular Syndesmosis Dysfunction: A Systematic Literature Review of Dynamic Versus Static Fixation Over the Last 10 Years. J Foot Ankle Surg 58(2): 320-327.
-
Walker L, Willis N (2015) Weber C ankle fractures: A retrospective audit of screw number, size, complications, and retrieval rates. J Foot Ankle Surg 54(3): 454-457.
-
Klepacki K, Kowal I, Konieczny G, Tomczyk L, Miękisiak G, et al. (2022) Radiographic Assessment of Tibiofibular Syndesmosis Injury with Different Durations and Types of Fixation. J Clin Med 11(21): 6331.
-
Fonkoue L, Sarr L, Muluem OK, Gueye AB, Dembele B, et al. (2021) Early post traumatic ankle osteoarthritis following ankle fracture dislocation in a subsaharan African. Journal of orthopaedics and traumatology surgery and research 107(6): 759-765.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results