Results of LRS (Limb Reconstruction System) in Management of Infected Non Unions of Femur
Introduction: Infected non-union needs prolonged treatment and repeated surgeries which significantly impacts patient’s social, financial, physical and mental life. In relation to Ilizarov technique monolateral external fixator is less bulky, more comfortable and better tolerated by patient. In this study we aim to assess the union rates, infection control, alignment, complications and the functional outcome of infected femoral non-union managed with monolateral external fixator. Material and methods: This is a prospective interventional study carried out between June 2017 and June 2021 at tertiary care centre operated by a single surgeon. Patients diagnosed as infected non-union of femur clinically and radiologically and operated with monolateral external fixator were assessed. Functional and radiological assessment was done using ASAMI classification. Results: In our study 21 patients were operated which included 20 males (95.2%) and one female with mean follow up is 29.85 ± 11.42 months. The most common site of non-union is mid-shaft of the femur. The mean bone defect after debridement is 3.52 ± 2.23cm (1 -10cm). The mean time of bony union in our study is 180.65 days (range 95-740 days). The ASAMI classification of bone results is Excellent to good in 90% of patients. Conclusion: Our study suggested that the Limb reconstruction system can be successfully used in the management of infected non-union of femur as a stable fixation modality and achieve satisfactory outcome in terms of bony union and functional results. Pre-operatively planning of the LRS frame, radical debridement and maintaining stability of the LRS frame are key steps of the treatment.
Jenil Patel1*, Chetan Puram2, Yogesh Panchwagh3, Parag Sancheti4 and Ashok Shyam5
Keywords: Infected Non Union; External Fixator; LRS; Femur Non Union; Septic Non Union
Introduction
Infected non-union needs prolonged treatment and repeated surgeries which significantly impacts patient’s social, financial, physical and mental life [1]. Multiple factors like high energy trauma, poly trauma, comminuted and compound fractures, patient/systemic host factors, inadequate fixation, bone defect, poor blood supply, and infection contributes to poor bone healing and non union [2, 3]. Modalities of fixation like plating and nailing further jeopardise the periosteal and endosteal blood supply of the bone and leads to a non-union [4, 5, 6]. The infected non-union of femur accounts for 2.24% of all long bones non-union [7]. The non union is associated with other complications like deformity, limb length discrepancy, joint stiffness and disuse osteoporosis which needs to be addressed simulatneosuly [8, 9].
Presently in literature there are two schools of thought in the treatment of infected non-union [1]: the ‘union-first’ strategy and the ‘infection-elimination first’ strategy. The union first strategy aims at achieving union first and then dealing with the problem of infection as the problem presents itself. On the other hand infection-elimination first strategy aims at elimination of infection as the first and major objective and bone union as the next objective. The bone defect that results from bone debridement can be managed by various techniques like - the llizarov, intramedullary device with or without external fixator, free tissue transfer, Papineau-type open cancellous bone grafting, bone transport through an external fixator / nail or Ilizarov external fixator [1, 8, 9, 10, 11]. Ilizarov technique depends on the principle of distraction osteogenesis and is being widely used in management of infected non-union of long bones [11]. However, the circular external fixator devise is cumbersome, expensive, time consuming, complex with a steep learning curve, not so patient friendly [12].
Thus in cases of femoral non-union where Ilizarov ring fixator is cumbersome, surgeons prefer bone elongation technique using monolateral external fixator developed by the Orthopaedic Institute of Verona [13]. Monolateral external fixator is less bulky, more comfortable and better tolerated by patient as compared to Ilizarov external fixator. It is simple in design, easy to learn and carry out surgical procedure, also easier to remove [12, 13, 14, 15, 16]. Associated complications like infection, deformity, limb length discrepancy can be tackled with monolateral external fixator. In this study we aim to assess the union rates, infection control, complications and the functional outcome of infected femoral non-union managed with monolateral external fixator.
Aims and Objectives
1. To review the incidence, diagnosis, treatment, and functional outcome of LRS in management of infected non unions of femur. 2. To study the different complications of LRS.
Material and Methods
This is a prospective interventional study carried out between June 2017 and June 2021 at tertiary care centre which included a size of 21 patients operated by a single surgeon. Ethical committee approval was sought for the study.
Inclusion Criteria
- Age group: 18 years to 70 years .
- Clinically, radiologically and microbiologically diagnosed as infected non-union of femur.
- Patient willing to give written informed consent.
Exclusion criteria
- Skeletally immature patients (<18 yrs) .
- Patients with neurological impairment of the ipsilateral lower extremity.
- Tuberculous non-union.
- Patients with aseptic non-union of femur.
Informed consent for participation in the study was taken from all the patients. Patients were assessed clinically, radiologically for the signs and symptoms of infected non- union. Demography of patients, duration of signs and symptoms, mode of injury, medical history, number of previous surgeries, the presence of tenderness, sinus, and pus discharge, shortening, deformity, bone defect and neurovascular status of the lower limb were recorded. The diagnostic workup of all the patients were done which included haemoglobin, total leukocyte count, differential leukocyte count, erythrocyte sedimentation rate (ESR) and C- reactive protein (CRP), sample for culture from the discharging sinus. Antero-posterior x-rays of the affected femur were done and the patients were graded as per the Jain AK17 classification for infected non-union. Surgical intervention in form of debridement and application of monolateral external fixation using Limb Reconstruction System (LRS) were performed with informed surgical consent. All the surgeries were performed by single surgeon trained in limb reconstruction techniques.
Operative Procedure
All the patients were operated under spinal anaesthesia in lateral position, with affected side facing up on a radiolucent table. (Figure 1) Painting and draping was done to keep the thigh exposed from the anterior superior Iliac spine till the Knee joint. In patients with sinus tract formation, intra- operative sinography with Methylene Blue was done to excise sinus tract in toto. Incision was taken on the previous scar unless contraindicated. Implant removal was done first followed by removal of the non-viable soft tissue, fibrosis and the dead necrotic bone. Debridement was done till the cortical bleeding known as the ‘paprika sign’ was seen. (Figure 2) Intraoperative samples thus obtained were sent for Gram staining, culture and sensitivity and mycobacterial cultures. The bone ends were freshened, the medullary canal was reconstituted (Figure 3,4) and open reduction of the main fragments was performed (Figure 5) to achieve the best possible contact between them and temporary fixation was performed using K-wires under c-arm guidance. Mono-focal procedures was performed when the bone defect was equal to or less than 2 cms. Bifocal procedures were performed when bone defect was more than 2 cms. A single-level bone transport was performed using either the ascending technique or the descending technique through healthy tissue. In all the patients the precise position of the clamps and the Schanz pins were determined according to the site of non-union, bony defect, corticotomy site and the LRS frame was assembled pre operatively on the trolly and kept ready (Figure 6). The preassembled LRS frame was applied. Corticotomy (Figure 7) was done at the site decided pre-operatively as per the location of the non-union which included a total of 10 patients. Osteoperiosteal flap was raised at the non union site. (Figure 8) The wound was lavaged thoroughly and closed in layers over a suction drain. In patients with long standing resistant infection without significant bone loss, antibiotic impregnated beads or the biologically absorbable antibiotic impregnated stimulan was used. In cases with delayed union and persisting bone defect, secondary procedure of bone grafting was carried using autograft or allograft.
| 1. Positioning on the operative table | 2. Paprika sign |
| 3. Intramedullary reaming | 4. Freshening of the bone edges with sharp cutting saw and osteotome |
| 5. Open reduction of the fracture ends | 6. Preassembled LRS frame. |
| 7. Corticotomy with osteotome | 8. Osteoperiosteal flaps |
Post operatively intravenous antibiotics in the form of Cefuroxime (1.5gm/12hrly) were started empirically. Antibiotics were modified according to the culture and sensitivity report of the intra operative samples and were given for period of 6 weeks or until the ESR and CRP level returned to normal. Drain removal was done on 2nd post- operative day and Hip/Knee joint movements was started as early as possible after the operation. Partial weight bearing with walker support was started for all cases depending on patient’s pain, compliance, local soft tissue condition and quality of bone. Full weight bearing was started after three cortex healing was seen on radiographs and as tolerated by the patient. Distraction at the rate of 0.25 mm four times a day [one-quarter rotation of compression–distraction unit] was started on 7th post-operative day.
Outcome measures
Patients were followed up on OPD basis at 2 weeks, 6 weeks, 12 weeks and then every month till radiological sign of union was obtained (at least three out of four cortices united) then 3 monthly thereafter. The quality and pattern of the distraction callus was evaluated on radiographs and the distraction rate was modified accordingly. Patients were assessed clinically for signs of healing and infection in the form of discharging sinus, fever, tenderness. Pin tract discharge, pin loosening, limb length discrepancy and any other complications were examined. Monolateral external fixator was maintained till radiologically 3 cortex healing and clinical signs of union were seen by checking for active straight leg raising after removing the rail with pins in situ. Functional assessment was done using ASAMI (Application of the method of Ilizarov) classification [18] at final follow up.
Treatment index (or radiographic consolidation index) was defined as the time (in days) for the appearance of consolidation of at least 3 cortices on the anteroposterior and lateral radiographs divided by the total amount of bone transported and/or the amount of lengthening (in cm). Lengthening index was measured as the days of bone transport/lengthening per cm gain in length. Healing index (external fixator index) was determined as days of fixator used / centimetres of length gained. The radiological results were assessed with ASAMI classification [18]. The independent sample t test was used for comparison of continuous variable and for categorical variables chi square test (or Fisher exact test) was used. P values less than or equal to 0.05 was considered statistically significant .The entire data was statistically analysed using Statistical Package for Social Science (SPSS ver. 20)
Results
In our study 21 patients were operated which included
20 males (95.2%) and one female with mean follow up is 29.85 ± 11.42 months. The mean age is 36.68 ± 9.63 years (range 19-51). The majority of the patients are in age group of 31-40 years accounting for 38.1 % of patients followed by 41-50 years of age group accounting for 28.6% of patients. The mean BMI is 26.36 ± 4.87 kg/m2 (range 17.7-38.3). Three patients (14.28%) had comorbidities in the form of diabetes, 1 patient (4.76%) had both diabetes and hypertension, 1 patient (4.76%) had hypothyroidism, 1 patient (4.76%) had post traumatic seizure.
Road traffic accident is the primary cause of fracture in all the patients, with 12 patients (57.1%) sustaining compound fracture while 9 patients (42.9) sustaining closed fracture. According to the AK Jain classification, maximum patients are in Type B group (with draining sinus), accounting for 61.9 % (13 patients), in which B1 type (bone gap less than 4cm) is most common (38.1%). Remaining 8 patients (38.1%) are in Type A group (without discharging sinus) in which A1 type is most common, accounting for 33.3% (7 patients).
The mean duration of non-union is 11.76 months (range 3-36 months) with maximum patients (42.9%) presenting with non-union for a duration of 6-12months, 33.3% patients presented with non-union for more than 12 months while 23.8% patients presented with non-union for less than 6 months. The mean previous surgical procedures performed are 2 ± 1.09 (range 1-5). The clinical and radiological signs of infection in the form of discharging sinus in various stages are present in 13 patients (61.90%), fever in 17 patients (80.95%), increased local temperature is present in 17 The intra-operative sample is positive in 17 patients (80.95%) while it is negative in 4 patients (19.05%). The most common organism found is Methicillin resistant Staphylococcus aureus (MRSA) in 5 patients (23.8%). The organisms cultured in our study population are mentioned in following table (Table 1).
patients (80.95%), tenderness at non-union site is present in all patients and clinical shortening is seen in 15 patients (71.42%).
| Number of patients | Percentage (%) | |
|---|---|---|
| E Coli | 1 | 4.8 |
| Enterobacter Cloacae | 2 | 9.5 |
| Enterococcus | 1 | 4.8 |
| Isolated | 2 | 9.5 |
| Klebsiella Pneumoniae | 1 | 4.8 |
| Mrsa | 5 | 23.8 |
| Mssa | 1 | 4.8 |
| Pseudomonas | 1 | 4.8 |
| Pseudomonas Aeruginosa | 1 | 4.8 |
| Serratia. Marcescens | 1 | 4.8 |
| Staphylococcus Epidermidis | 1 | 4.8 |
| Total | 17 | 81 |
Table 2: Organisms isolated from the infection site.
The mean bone defect after debridement is 3.52 ± 2.23cm (1 -10cm) and corticotomy for lengthening is done in 9 patients. The treatment index (radiographic consolidation index) is 28.58 ±1.37 days/cm, lengthening index is 11.58 ± 5.48 days/cm and healing index (external fixation index) is 32.16 ± 10.34 days/cm. The mean time of bony union in our study is 180.65 days (range 95-740 days) i.e 6 months. All the infected non-unions in our study united except one patient who had bifocal femur fracture with persistent infection.
According to the ASAMI classification of bone results the outcome is Excellent in 10 patients (47.6 %), good in 9 patients (42.9%) and one patient (4.8%) had fair and poor result each. Bony union is not achieved in one patient who is a case of bifocal femur shaft fracture. As per the ASAMI classification for functional results the outcome ware Excellent in 8 patients (38.1%) and Good in 13 patients (61.9%). Infection is eradicated in 18 patients (85.71%) of the patients and it remained persistent in 3 patients due to drug resistant organisms.
As per the correlation between the type of infected non-union and the ASAMI bone and functional grading the p value was 0.114 and 0.273 respectively which is not statistically significant suggesting no association between the type of infected non-union and the ASAMI bone and functional outcome. The complications noted in our study are mentioned below [Table 2].
| Complication | Number of patients | Percentage (%) |
|---|---|---|
| Knee Stiffness | 8 | 47.06 |
| Hip Stiffness | 4 | 23.53 |
| Limb Length discrepancy | 6 | 35.29 |
| Pin tract infection | 2 | 11.76 |
| Pin loosening | 3 | 17.65 |
Table 3: Complications.
Case Examples
Illustrations of Cases: Case: 1
A 28 yrs old male patient with alleged history of road traffic accident, sustained compound distal femur fracture which was operated with Open reduction and internal fixation with plating and got infected. Staged surgeries were performed, initially implant removal was done and later fixation with LRS and corticotomy was done. Patient had excellent outcome at final follow up as per ASAMI functional and bone score .
| Primary surgery | Pre op |
| LRS Application | 3 months post op |
| 7 months follow up | Post LRS removal |
| 1 year follow up | 15 months follow up |

Illustrations of Cases: Case: 2
surgeries and finally was operated with implant removal and LRS fixator application. As per ASAMI functional score the patient had good outcome and poor outcome as per ASAMI bone score.We suspect the involvement of bifocal fracture causing poor outcome.
A 49 yrs male patient with alleged history of road traffic accident,sustained left bifocal femur fracture for which was operated with closed reduction and internal fixation with interlocking nail got infected and then underwent staged
| Pre op | Implant-removal and LRS application |
| 6 months follow up | 5 months post lrs removal -11 month follow up |
| 2 Year follow up |
Discussion
Management of the infected non-union of long bone like femur is technically demanding for the surgeon, needs prolonged time, may need multiple interventions and if not treated properly can land up in amputation of lower limb. The associated conditions like the discharging sinus, previous scars, atrophy, bony defect, multiplanar deformities, multidrug resistant infection, limb length discrepancy, adjacent joint stiffness, etc. make the management more challenging for the surgeon [17]. Also it has a devastating effect on patient’s social and financial status. Most of this patients are previously operated for stabilisation, eradication of infection, which causes compromise in the soft tissue and the vascularity of the bone which complicates healing. Eradication of the infection and achieving the union are the two important goals of the treatment for a functional limb along with secondary factors like deformity correction, limb length correction, soft tissue coverage etc.
Ilizarov technique which includes distraction osteogenesis have revolutionized the management of the complex non-union of long bone and associated ailments likes bony defect, infection, deformity, limb shortening etc.
[3, 19, 20]. It is based on the law of tension stress [21] which includes gradual traction on living tissues creating necessary stress that stimulates histogenesis, promotes regeneration and active growth of tissues. However Ilizarov technique is complex and technically difficult to perform, need prolong time to achieve union, is associated to chances of pin-tract infection and is inconvenient to patient to carry and maintain it [15]. LRS can be used in management of the complex non- union. It is based on the same principal of Ilizarov distraction osteogenesis, has uniplanar frame, light weight, easy to construct, with short learning curve and convenient to the patient.
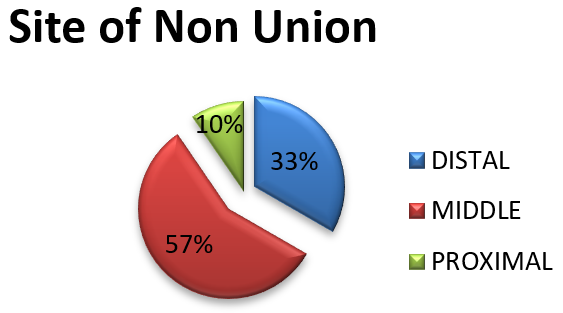
Our study proves that monolateral external fixator (LRS) can be successfully used in the management of the infected non-union of the femur. According to the AK Jain classification, maximum patients in our study are in Type B group (61.9 %), in which B1 type (bone gap less than 4cm) is most common (38.1%) and the most common site of non- union is mid-shaft of the femur in 12 patients (57.1%). The mean previous surgical procedures performed in our study population are 2 ± 1.09. It is comparable to the previous studies [10, 22].
Radical debridement, complete excision of the bacterial biofilm is essential in order to prevent persistent and recurrent infection [23]. The mean bone defect after debridement in our study is less as compared to other studies, while treatment index (radiographic consolidation index), lengthening index and healing index (external fixation index) in our study is comparable to other similar studies (Table 3).
| Mean bone defect | Treatment index | Lengthening index | Healing index | |
|---|---|---|---|---|
| (consolidation index) | (External fixation index) | |||
| Arora S, etal. [10] | >5cm | 27.9 days /cm (24-40) | 12.3 days/cm (11.5-15) | |
| Agrawal HK etal. [22] | 5.83cm | 23.51 days/cm (17-45.5) | 13.06 days/cm | 36.53 days/cm (28-61.5) |
| Yin P, et al. [24] | 6.15cm | 10.47 days/cm | 45days /cm | |
| Our study | 3.52 ± 2.23cm | 28.58 ±1.37 days/cm | 11.58 ± 5.48 days/cm | 32.16 ± 10.34 days/cm. |
Table 6: Comparison of various parameters.
The mean time of bony union in our study (180.65 days) is less as compared to previous studies [10, 22] who noted bony union in 7.3 months and 204 days respectively. This might be probably due to less bone defect in our study. All the infected non-unions in our study united except one patient who had bifocal femur fracture with persistent infection. According to the ASAMI classification of bone results the outcome is excellent too good in 90% of the study group. Our results are comparable to previous studies [22, 24] who too achieved excellent to good results in 90% of their study population (Table 4).
The ASAMI classification for functional outcome is excellent too good in 99% of the patients in our study. (Table 4) Infection was eradicated in 85.71% of the patients and it remained persistent in 3 patients due to drug resistant organisms. The functional results are better than other similar study [10, 22, 24] which might be probably due to lesser bone defect in our study as compared to other studies, achieving early limb lengthening and mobilisation as compared to other studies. Also our study did not have patients with gunshot and cylinder blast injury which are high velocity injuries with considerable soft tissue damage, which takes longer period to recover. The bone result did not correspond with the functional outcome as it was also determined by condition of joints, limp while walking. Also the correlation between the type of infected non-union and the ASAMI bone and functional grading is not statistically significant (p value is 0.114 and 0.273 respectively) suggesting no association between the type of infected non-union and the ASAMI bone and functional outcome.
| Results | Arora S, etal. [10] | Agrawal HK, etal.[22] | Yin P etal. [24] | Our study |
|---|---|---|---|---|
| %(n) | %(n) | %(n) | %(n) | |
| Bone | ||||
| Excellent | 80% (12) | 56.66% (17) | 57.89% (22) | 47.6% (10) |
| Good | 20% (3) | 30% (9) | 28.94% (11) | 42.9% (9) |
| Fair | 10% (3) | 13.15% (5) | 4.8% (1) | |
| Poor | 3.33% (1) | 4.8% (1) | ||
| Functional | ||||
| Excellent | 33.33% (5) | 30% (9) | 31.57% (12) | 38.1% (8) |
| Good | 53.33%(8) | 46.66% (14) | 39.47% (15) | 61.9% (13) |
| Fair | 13.33%(2) | 16.66% (5) | 21.05% (8) | |
| Poor | 6.66% (2) |
Table 7: Comparison of ASAMI outcome.
None of the patients in our study had neurovascular complication, joint instability, newly formed bone fracture or angular deformity. The knee stiffness is present in 8 patients (47.06%) and hip stiffness is present in 4 patients (23.53%). Other complications like Limb length discrepancy is present in 6 patients (35.29%), pin tract infection is present in 2 patient (11.76%) and pin loosening is present in 3 patients (17.65%) (Table 2). The limb length discrepancy in all the patients is less than 2cms and is manged with appropriate shoe raise, patients are functionally comfortable with the same. Pin tract infection is managed with appropriate sensitive antibiotics and the loose pins are exchanged. Even though we paid more attention to pin-track care, there was still a high incidence of pin tract infection, which also depends on the immunity and bone quality of patient. The complications in our study are comparable to other studies in the literature [10, 22, 24]. Active involvement and participation of the patients, early mobilisation and monitored physiotherapy are paramount important to avoid joint stiffness and the success of the LRS. Nearly all of our patients are able to stand and walk with partial weight bearing immediately after LRS application. Patient should be involved in regular cleaning of the pin tract and maintain proper hygiene. Also they must be advised to monitor the inflammation, tenderness, and discharge around the pin tract and sought medical care immediately.
The small sample size and short term follow up are shortcomings of our study. However all surgeries were performed at a single institution by single surgeon, and we aim to continue follow up for long term results. The LRS is more suitable for infected non-union of femur as it has extensive soft tissue envelope and the neurovascular structure making it difficult and challenging for Illizarov technique. LRS is a dynamic frame which is simple in design and application and easy to carry out during a surgical procedure while maintaining it, and it can also alleviate pain caused by pin during the distraction period compared to the Ilizarov external fixator [23]. With LRS multiple issues can be addressed simultaneously like deformity correction, regenerate new bone by distraction osteogenesis, correction of limb length discrepancy, bone transport, early mobilisation and rehabilitation to avoid joints stiffness. Also it’s necessary to maintain and restore the soft tissue envelope around the non-union site which vascularises the site, improves antibiotic delivery, fills the dead space and prevents further contamination.
Conclusion
Our study suggested that the Limb reconstruction system can be successfully used in the management of infected non- union of femur as a stable fixation modality and achieve satisfactory outcome in terms of bony union and functional results. Pre-operatively planning of the LRS frame, radical debridement and maintaining stability of the LRS frame are key steps of the treatment. It is a prolonged treatment which need longer follow up, monitoring, motivated and complaint patients along with physical rehabilitation. Complications like pin tract infection and pin loosening must be addressed immediately. It is a simple and more acceptable alternative to Illizarov fixation in management of infected non-union of femur. However in some patients the infection may still remain persistent even after achieving bony union, which may need multidisciplinary approach, further intervention and prolong period of treatment.
Conflict of interest: On behalf of all authors, the corresponding author states that there is no conflict of interest.
References
-
Motsitsi NS (2008) Management of infected nonunion of long bones: the last decade (1996-2006). Injury 39(2): 155-160.
-
Nicoll EA (1964) Fracture of tibial shaft. A survey of 705 cases. J Bone Joint Surg 46B: 373-87.
-
Saleh M (1992) Non-union surgery. Part 1. Basic principles of management. IJOT 2: 4-18.
-
Chao EYS, Aro HT (1989) Biomechanics and Biology of external fixation. In: Coombs R, Green S, et al. (Eds.), External fixation andfunctional bracing. London: Orthotext, UK, pp: 67-95.
-
McKibbin B (1978) The biology of fracture healing in long bones. J Bone Joint Surg 60B(2): 150-162.
-
Ilizarov G (1989) The influence of stability of fixation and soft tissue preservation. The tension- stress effect on the genesis and growth of tissues. Cl Orthop R Res 238: 249-281.
-
Mills LA, Hamish A (2013) The relative incidence of fracture non-union in the Scottish population: a 5-year epidemiological study. BMJ Open 3.
-
Charles RA, Green DP, Bucholz RW (2006) Rockwood and Green’s Fractures in Adults. In: 6th (Edn.), Philadelphia: Lippincott Williams & Wilkins.
-
Dendrinos GK, Konto S, Lyritsis E (1995) Use of Ilizarov technique for treatment of nonunion of tibia associated with infection. J Bone joint Surg 77(6): 835-846.
-
Arora S, Batra S, Gupta V, Goyal A (2012) Distraction osteogenesis using a monolateral external fixator for infected non-union of the femur with bone loss. J Orthop Surg 20(2): 185-190.
-
Spiegelberg B, Parratt T, Dheerendra SK, Khan WS, Jennings R, et al. (2010) Ilizarov principles of deformity correction. The annals of the royal college of surgeons of England 92(2): 101-105.
-
Marsh JL, Nepola JV, Meffert R (1992) Dynamic external fixation for stabilization of nonunion. Clin Orthop (278): 200-206.
-
De Bastiani G, Aldegheri R, Renzi-Brivio L, Trivella G (1987) Limb lengthening by callus distraction (callotasis). J Pediatr Orthop 7(2): 129-134.
-
Sangkaew C (2008) Distraction osteogenesis of the femur using conventional monolateral external fixator. Arch Orthop Trauma Surg 128(9): 889-899.
-
Paley D (1990) Problems, Obstacles and complications of limb lengthening by the Ilizarov technique. Clin orthop Relat Res 250: 81‐104.
-
Hashmi MA, Ali A, Saleh M (2001) Management of non- unions with mono-lateral external fixation. Injury Int J Care Injured 32(S4): SD30-SD34.
-
Jain AK, Sinha S (2005) Infected nonunion of the long bones. Clinical Orthopaedics and Related Research. 431: 57-65.
-
Yin P, Zhang Q, Mao Z, Li T, Zhang L, et al. (2014) The treatment of infected tibial nonunion by bone transport using the Ilizarov external fixator and a systematic review of infected tibial nonunion treated by Ilizarov methods. Acta Orthop Belg 80(3): 426-435.
-
Ilizarov GA (1989) The tension‑stress effect on the genesis and growth of tissues. Part I, The Influence of stability of fixation and soft tissue preservation. Clin Orthop Relat Res 238: 249‑281.
-
Lynch JR, Taitsman LA, Barei DP, Nork SE (2008) Femoral nonunion; risk factors and treatment options. J Am Acad Orthop Surg 16(2): 88‑97.
-
Charnley J, Baker Sl (1952) Compression arthrodesis of the knee. A clinical and histological study. J Bone Joint Surg 34B(2): 187-199.
-
Agrawal HK, Garg M, Singh B, Jaiman A, Khatkar V, et al. (2016) Management of complex femoral nonunion with monorail external fixator: A prospective study. J Clin Orthop Trauma 7(S2): 191-200.
-
Patzakis MJ, Zalavras CG (2005) Chronic posttraumatic osteomyelitis and infected non-union of the tibia: current management concepts. J Am Acad Orthop Surg 13(6): 417-427.
-
Yin P, Zhang L, Li T, Zhang L, Wang G, et al. (2015) Infected nonunion of tibia and femur treated by bone transport. J Orthop Surg Res 10: 49.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results