Infective Spondylodiscitis of Unknown Origin in A Patient with Chronic Kidney Disease
Infective spondylodiscitis is a rare but serious condition characterized by the involvement of the intervertebral disc and adjacent vertebral bodies. The late discovery of this infectious process has been attributed to its delayed and sneaky beginning and ambiguous symptoms. Here, we looked at the clinical traits and prognoses for haemodialysis patient who suffered spondylodiscitis and was diagnosed with it. This report delves into a challenging case of infective spondylodiscitis in a 53-yearold male with chronic kidney disease (CKD) undergoing hemodialysis. The patient's complex presentation, diagnostic journey, and treatment outcomes are meticulously examined, highlighting the intricacies of managing this condition in individuals with underlying health issues.
Introduction
Infective spondylodiscitis is a challenging condition that results from the bacterial or fungal infection of the intervertebral disc and adjacent vertebral bodies [1]. The usual manifestation includes pain, elevated body temperature, and neurological symptoms. Due to the disease’s infrequency and insidious manifestation of symptoms, the identification of the condition may become delayed. Hence, significant concerns such as the occurrence of an abscess in adjacent tissue, irreversible permanent neurological abnormalities, or even mortality may arise prior to the identification of a diagnosis. Although there have been advancements in prolonging the lives of patients undergoing haemodialysis for end-stage renal disease, the mortality rate for those who develop bacteraemia or sepsis due to repeated vascular access, medically induced immunosuppression, and urinary tract infections remains elevated at 9.7% [2, 3]. This report describes the case of a 53-year-old male with infective spondylodiscitis complicated by chronic kidney disease, highlighting the importance of a multidisciplinary approach in managing such complex cases.
A 53 years old male presented to the outpatient department of our institution with complaints of significant neck pain affecting his daily activities for the past 3 months. Pain has since been radiating to both the arms (left > right) which was associated with tingling sensation. Upon
evaluating the neurology, the MRC (Medical Research Council) grade of both upper limbs was found to be 4/5 with finger grip weakness was observed more pronounced on the left side. Patient also had increasing gait imbalance while walking contributing to significant problems at workplace. There was no history of fall, trauma, or any significant strain to the cervical spine. On analysis of past history, revealed to be a known case of chronic kidney disease (CKD) and was on renal dialysis, since the past 5 years. Patient’s blood reports had an evident finding of raised serum creatinine (7.1) and borderline elevated serum ESR and CRP. Other blood parameters were within normal limits. Pre op x-ray showed reduced disc space in C5-C6 with partial destruction of C4 and C5 vertebral body following collapse of the vertebrae (Figure 1). MRI revealed a foci of infection in C5-c6 disc space with fluid collection with cord compression.
Treatment
Patient was planned a staged treatment protocol, in which first was surgical intervention followed by intravenous antibiotics treatment. After medical optimisation was completed and fitness was received a standard Southwick -Robinson approach was taken following which meticulous dissection was carried out. After exposure C4-C5, C5-C6 junction was identified and confirmed under fluoroscopy. Suspected infective tissue along with disc and bone samples was collected un sterile container for investigations. After thorough debridement and wash end plates were prepared, dead necrotic tissue removed followed by C5 corpectomy. Mesh cage was placed with acdf at C6-C7 vertebral bodies supplemented with anterior plate was fixed from C4 to C7 vertebra. Thorough wash was given and closure was done in layers. Post operative we administered intravenous broad spectrum antibiotic Cefaperazone-Sulbalctum intravenous for 2 weeks. He underwent heparin free dialysis post- surgery and was hemodynamically stable after which he was discharged. The peculiar characteristic in this case was the intraoperative culture reports were negative for Mycobacterium to or any other bacteria. Hence the continuation of broad spectrum was given IV for 2 weeks and then followed up by oral antibiotics for a duration of 4 weeks.

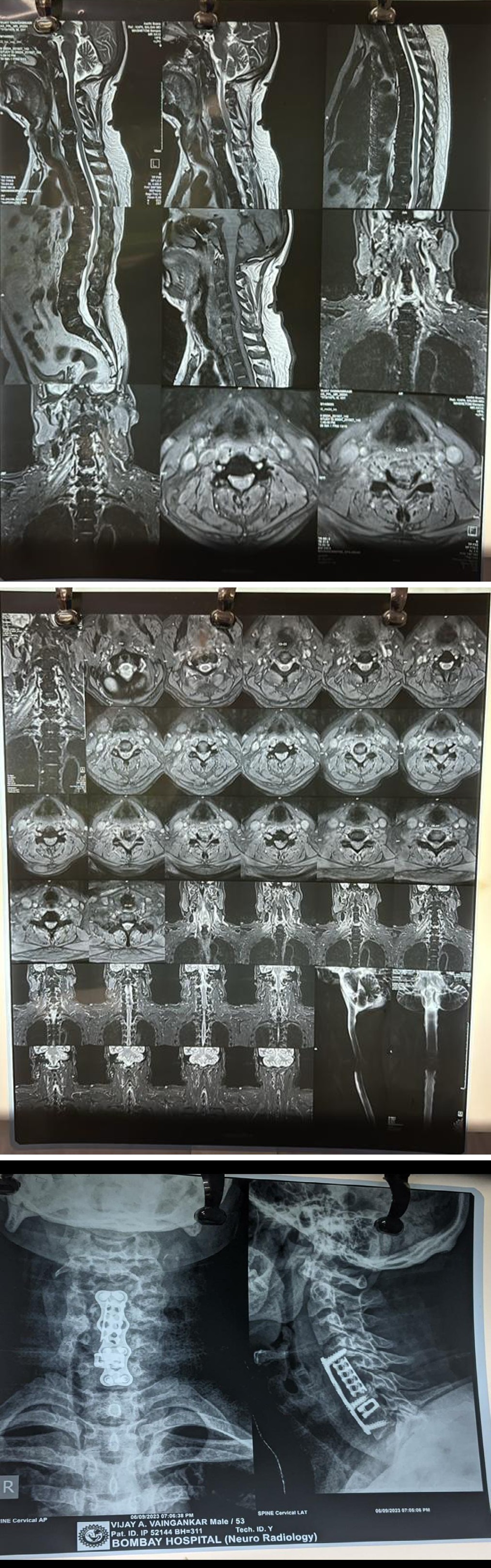
Figure 2 &3: MRI revealing foci of infection with fluid collection with cord compression.
Discussion
According to a study of the literature, intravenous drug use, poorly managed or uncontrolled diabetes mellitus, catheter- associated infection problems, infective endocarditis, history of spine surgery, and immune compromised condition are common risk factors for infective spondylodiscitis [4]. Prior research on dialysis patients and the general public on infectious spondylodiscitis revealed that the majority of infections occurred in the lumbar spine (58–68%), thoracic spine (27–30%), and cervical spine (5-81%) [5]. According to previous research on spinal osteomyelitis, 85% of the organisms found in blood cultures were also found in biopsy specimens. Consequently, it can be recommended that, wherever possible, all patients with suspected infective spondylodiscitis have their blood and tissue cultures taken. In this case the samples that were sent were negative for any kind of bacterial or fungal infection. Mycobacterial tuberculosis was not isolated from the specimen of isolated disc or vertebral bone [6]. Patient was followed up regularly in the outpatient department after 2 weeks, 1 month and 2 months. Upon neurological assessment his finger grip had improved which was found to be 5/5.In people with ESRD (End stage renal disease), a number of risk factors contribute to the illness’s development and antibiotic failure. Difficult- to-diagnose conditions include imprecise initial symptoms, concurrent destructive spondyloarthropathy, weakened immune system, persistently elevated inflammatory markers, and recurrent bacteraemia. Permanent brain abnormalities are more likely to result from infectious processes than from temporary ones [7, 8]. Even in situations of severe destructive osteomyelitis, fever may not be the first symptom to appear, and it occasionally manifests as a latent infection. Therefore, even in patients who do not have a fever when they present with end-stage renal disease (ESRD), a spinal infection should be considered as a potential cause of back pain, and an MRI should be done to make an early diagnosis. In all cases of spondylodiscitis, surgical intervention with debridement and posterior instrumentation should be taken into consideration as a modality of treatment. This approach has better clinical outcomes in terms of functionality, disability, and rehabilitation, as well as acceptable perioperative complication rates that can be tailored to the specifics of each case [9]. Despite the instrumented group having a greater degree of neurological deficit, more involved levels, and an increased kyphotic angle, the results of instrumented surgery for haemodialyzed patients with pyogenic spondylodiscitis were comparable to those of non-instrumented surgery, including recurrence and mortality [10].
Conclusion
This case study is a testament that patients who receive long term haemodialysis or are in hospital based environments for longer periods, it is crucial to identify spondylodiscitis in such patients. Classical features should be looked for: the classic triad of pain, fever, and neurological deficits. Optimal use of enhanced MR scans in patients presenting with significant neck pain can help establish the diagnosis, which can then guide the best course of treatment.
References
-
Lu YA, Hsu HH, Kao HK, Lee CH, Lee SY, et al. (2017) Infective spondylodiscitis in patients on maintenance hemodialysis: a case series. Ren Fail 39(1): 179-186.
-
Cassó-Troche LR, Echavarría-Uceta JA, Quiñones-Robles J, Haché-Pagan C, Herrera I, et al. (2022) Infective spondylodiscitis in hemodialysis patients. Surg Neurol Int 13: 549
-
Chen LH, Fu TS, Kao YH, Tsai TT, Lai PL, Niu CC, et al. (2010) Surgical treatment of infectious spondylitis in patients undergoing hemodialysis therapy. Eur Spine J 19(12): 2223-2228.
-
Kapsalaki E, Gatselis N, Stefos A, Makaritsis K, Vassiou A, et al. (2009) Spontaneous spondylodiscitis: Presentation, risk factors, diagnosis, management, and outcome. Int J Infect Dis 13(5): 564-569.
-
Saran R, Li Y, Robinson B, Abbott KC, Agodoa LYC, et al. (2016) US Renal Data System 2015 Annual Data Report: Epidemiology of kidney disease in the United States. Am J Kidney Dis 67(3S1): S1-S305.
-
Afshar M, Reilly RF (2011) Spondylodiscitis in a patient on chronic hemodialysis. Nat Rev Nephrol 7: 599-604.
-
Faria B, Canto Moreira N, Sousa TC, Pêgo C, Vidinha J, et al. (2011) Spondylodiscitis in hemodialysis patients: A case series. Clin Nephrol 76: 380-387.
-
Madhavan K, Chieng LO, Armstrong VL, Wang MY (2019) Spondylodiscitis in end-stage renal disease: a systematic review. J Neurosurg Spine 15: 1-9.
-
Vinay Jain K, Ravikumar TV (2020) Surgical Management of Thoracolumbar Spondylodiscitis in End-Stage Renal Disease. Indian J Orthop 55(S1): 176-181.
-
Kim J, Lee SY, Jung JH, Kim SW, Oh JK, et al. (2019) The outcome following spinal instrumentation in haemodialyzed patients with pyogenic spondylodiscitis. Bone Joint J 101-B(1): 75-82.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results