Why Hba1c is an Unpredictable Marker for the Outcome of Wound Healing Disorders before Total joint Arthroplasty
Background: Notwithstanding the fact that Hba1c is frequently used as a marker for glycaemic control in the pre-operative period of surgery, there is no common and direct concordance regarding its actual role for the same. This study was done to ascertain the role of Hba1c as a harbinger for the outcome of wound healing disorders before total joint arthroplasty. Methods: The data of 100 patients undergoing uni/bilateral TJA in one/staggered sitting in the year 2022 was collected in our hospital. Out of them, 50 were TKA while the other 50 were THA. Patient specific data were collected from the data record system of our hospital, including data of HbA1C from biochemistry department, patient records from dressing room data register and wound culture reports details from microbiology department and patient prescriptions. Results: There was 6% incidence of wound healing disorders among 100 patients who were part of our study. The incidence of wound healing disorders in non-diabetic patients was 5.95% and was 6.25% in diabetic patients; whereas incidence in patients with normal random blood sugar was 12.12%, those with high random blood sugar was that of 2.99%.
Abbreviations
Hba1c: Glycated haemoglobin; TJA: Total Joint Arthroplasty; TKA: Total Knee Arthroplasty; THA: Total Hip Arthroplasty; SSI: Surgical Site Infection; PJI: Peri-prosthetic Joint Infection.
Introduction
The relationship between elevated HbA1c and postoperative SSI or PJI after THA and TKA is controversial [1]. Diagnosis of diabetes, preoperative hyperglycemia and elevated HbA1c are not likely direct risk factors for PJIs, but more likely to be indirect markers of more serious comorbid conditions (e.g. chronic kidney disease, peripheral vascular disease, etc.). Patients, with a sole diagnosis of well- controlled diabetes, do not confer a clinically significant risk for PJIs. For those with HbA1c ≥ 8 to 9% or glucose levels above 200 mg/dL, optimization may be a consideration in the preoperative period [2]. The aim of this study is to determine and investigate the association between postoperative wound complications (SSI/PJI) and elevated HbA1c in TJA patients.
Materials and Methods
We collected data of 100 patients undergoing uni/ bilateral TJA in one/staggered sitting in the year 2022 in our hospital. Out of them, 50 were TKA while the other 50 were THA. Patient specific data were collected from the data record system of our hospital, including data of HbA1C from biochemistry department, patient records from dressing room data register and wound culture reports details from microbiology department and patient prescriptions. Wound Healing Disorder (WHD) was considered if any of the following complications occurred: prolonged wound drainage, wound dehiscence, signs of erythema or necrotic changes at the wound edges.
Statistical Analysis
The presentation of the Categorical variables was done in the form of number and percentage (%). On the other hand, the quantitative data were presented as the means ± SD and as median with 25th and 75th percentiles (interquartile range). The association of the variables which were qualitative in nature were analyzed using Fisher’s exact test as at least one cell had an expected value of less than 5. Univariate logistic regression was used to find out significant risk factors of wound healing disorders (Figures 1-5).
The data entry was done in the Microsoft EXCEL spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA, ver 25.0. For statistical significance, p value of less than 0.05 was considered statistically significant.
Results
Diabetes mellitus (DM) was reviewed by physician or endocrinologist once the preoperative investigations reports were made available one day before elective surgery using fasting glucose or HbA1c tests, considering the patient’s history. A cut off of 126mg% was kept for fasting glucose level and of 6.5 for hba1c level, for the diagnosis of Diabetes Mellitus. The patients were divided into 2 groups based on HbA1c levels as per CDC guidelines: Category 1 - Hba1c less than or equal to 6.5% and Category 2 - Hba1c above 6.5%. Patients were explained in the post-operative hospital visits regarding the objectives of the study and appropriate consents were taken. They were then assessed. Based on their assessments, the following information was collected: postoperative WHD, culture reports, need for readmission, need for revision surgery. The main point of this study was to analyze increased HbA1c and the risk of postoperative WHD, surgical site infection (SSI) or early peri-prosthetic infections (PJI), need for revision surgery and readmission due to injury or infectious complications. Then we observed the occurrence of WHD in all the patients distributed in these 2 categories (Tables 1-7).
| Categories | Wound Healing Disorders |
|---|---|
| Category 1 (Hba1c <= 6.5) | 5 |
| Category 2 (Hba1c > 6.5) | 1 |
Table 1: Presence of wound healing disorder distribution.
| Presence of wound healing disorder | Frequency | Percentage |
|---|---|---|
| Absent | 94 | 94.00% |
| Present | 6 | 6.00% |
| Total | 100 | 100.00% |
Table 2: Presence of wound healing disorder distribution.
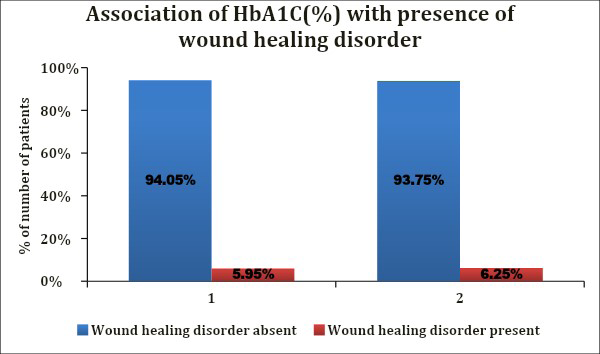
| Wound healing | Wound healing disorder absent (n=94) | Wound healing disorder present (n=6) | Total | P value |
|---|---|---|---|---|
| <=6.5% | 79 | 5 | 84 | |
| -94.05% | -5.95% | -100% | ||
| >6.5% | 15 | 1 | 16 | 1* |
| -93.75% | -6.25% | -100% | ||
| Total | 94 | 6 | 100 | |
| -94% | -6% | -100% |
Table 3: Association of HbA1C(%) with presence of wound healing disorder.
Fisher’s exact test
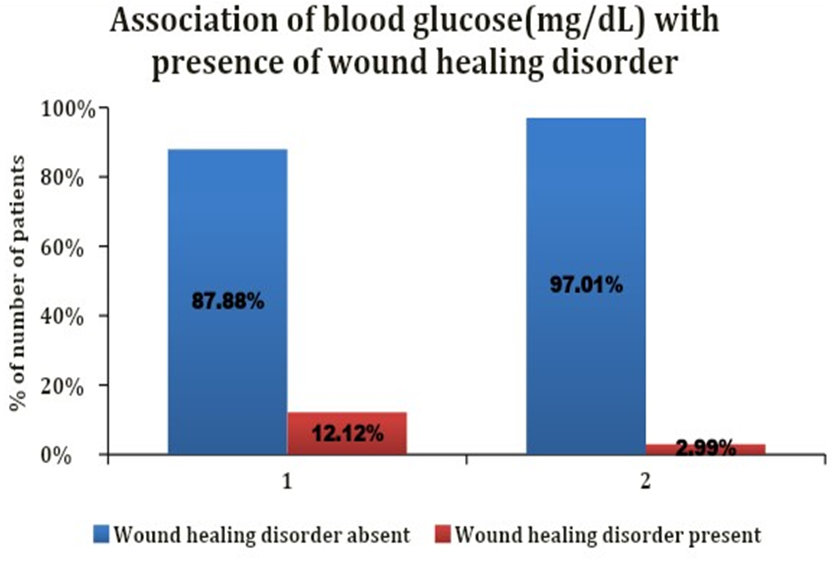
| Blood glucose(mg/ dL) | Wound healing disorder absent(n=94) | Wound healing disorder present(n=6) | Total | P value |
|---|---|---|---|---|
| <=200 mg/dL | 29 (87.88%) | 4 (12.12%) | 33 (100%) | |
| >200 mg/dL | 65 (97.01%) | 2 (2.99%) | 67 (100%) | 0.09* |
| Total | 94 (94%) | 6 (6%) | 100 (100%) |
Table 4: Association of blood glucose(mg/dL) with presence of wound healing disorder.
Fisher’s exact test
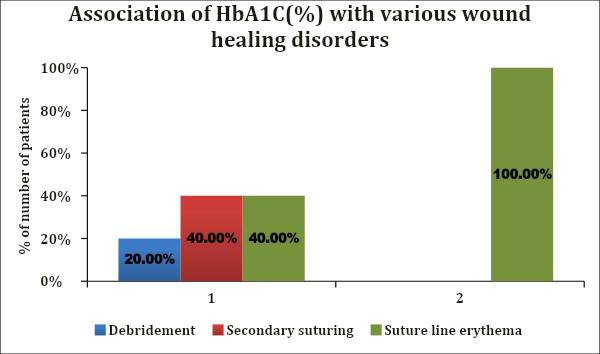
| HbA1C (%) | Debridement (n=1) | Secondary suturing (n=2) | Suture line erythema (n=3) | Total | P value |
|---|---|---|---|---|---|
| <=6.5% | 1(20%) | 2 (40%) | 2 (40%) | 5 (100%) | |
| >6.5% | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 1* |
| Total | 1 (16.67%) | 2 (33.33%) | 3 (50%) | 6 (100%) |
Table 5: Association of HbA1C (%) with various wound healing disorders.
Fisher’s exact test
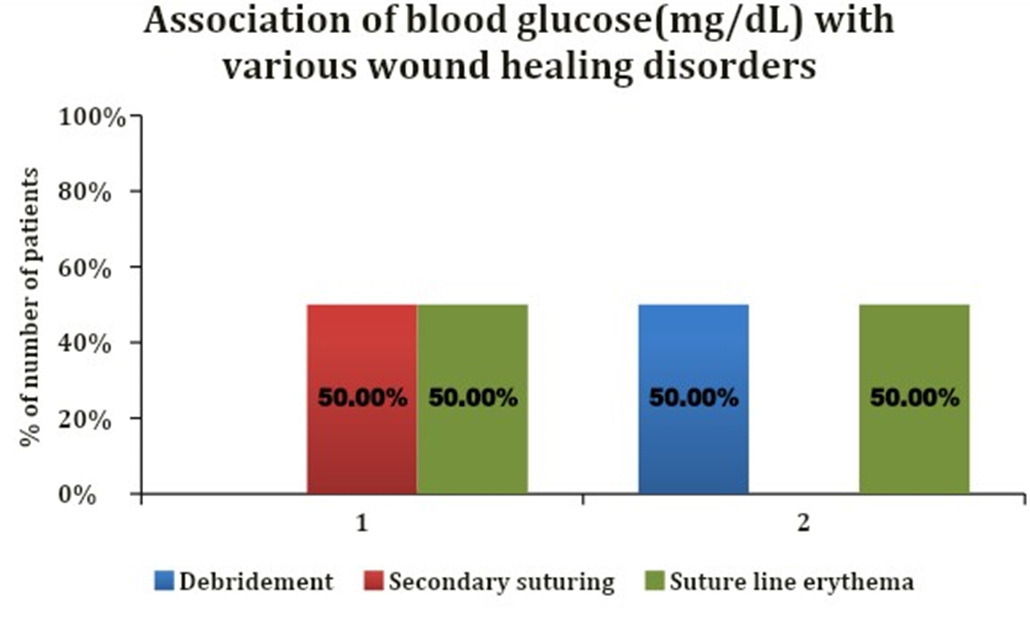
| Blood glucose(mg/dL) | Debridement(n=1) | Secondary suturing(n=2) | Suture line erythema(n=3) | Total | P value |
|---|---|---|---|---|---|
| <=200 mg/dL | 0 (0%) | 2 (50%) | 2 (50%) | 4 (100%) | 0.6* |
| >200 mg/dL | 1 (50%) | 0 (0%) | 1 (50%) | 2 (100%) | |
| Total | 1 (16.67%) | 2 (33.33%) | 3 (50%) | 6 (100%) |
Table 6: Association of blood glucose(mg/dL) with various wound healing disorders.
Fisher’s exact test
| Variable | Beta Coefficient | Standard Error | P value | Odds Ratio | Odds ratio Lower bound (95%) | Odds ratio Upper bound (95%) |
|---|---|---|---|---|---|---|
| Age(years) | -0.009 | 0.045 | 0.84 | 0.991 | 0.907 | 1.083 |
| Gender | ||||||
| Female | 1 | |||||
| Male | -0.473 | 0.966 | 0.624 | 0.623 | 0.094 | 4.141 |
| HbA1C(%) | ||||||
| >6.5% | 1 | |||||
| <=6.5% | -0.031 | 1.133 | 0.978 | 0.97 | 0.105 | 8.93 |
| Blood Glucose(mg/dL) | ||||||
| <=200 mg/dL | 1 | |||||
| >200 mg/dL | -1.386 | 0.828 | 0.094 | 0.25 | 0.049 | 1.267 |
Table 7: Univariate logistic regression to find out significant risk factors of wound healing disorders.
Discussion
Careful preoperative evaluation and investigation are necessary to identify most susceptible patients before these elective operations. Hence, it is important to optimize their perioperative general, metabolic and local conditions to reduce the risk of postoperative side effects [3]. In our study, the majority of the patients lie in Category 1 (84%) while in category 2, only 16% of the patients lie with the values of Hba1c ranging from 4 to 11.8. In our study, 67% of the patients had their blood sugar level more than 200mg% while 33% had their level less than 200mg%. The maximum value being 560mg%. In our study, the wound healing disorders were present in about 6% of the total. Study demonstrates 20% wound healing disorders in total tkrs [4]. Study demonstrates 10% WHD in TKRs [5]. In our study, various wound healing disorders comprised debridement (16.67%), secondary suturing (33.33%) and stitch line erythema (50%) of the total complications.
In our study, category 1 had wound healing disorders in 5.95% of its total patients. Category 2 had wound healing disorder in 6.25% of its patients. Study shows incidence of WHD of 1.2% in patients [6]. Study shows WHD in 7% [7].
In our study, high random blood sugar was associated with 2.99% of WHDs. Study demonstrates WHDs in 6.6% of patients [8].
In our study, blood glucose level > 200mg% was present in 33.33%% of wound healing disorder; whereas a level of <200mg% was present in 66.67% of patients with wound healing disorder, with 2% in those needing secondary suturing and 2% in those with stitch line erythema.
Conclusion
Despite many studies investigating the relationship between higher peri-operative HbA1c and fasting blood glucose levels and the risk of postoperative SSI, PJI or wound complications, some did not show significant correlations and many focused only on the presence of deep infections [9]. In addition, the specific threshold of HbA1c to predict postoperative SSI or PJI remains controversial.
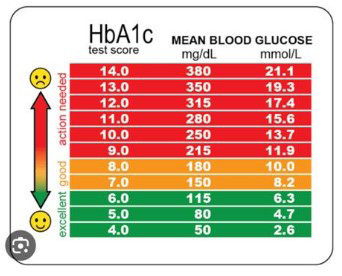
It is well established that poorly controlled diabetes mellitus is associated with worse surgical and medical outcomes in patients undergoing TJA. PJI is particularly high in this patient population. Several studies have already reported that optimal perioperative control of serum glucose levels reduces the risk of postoperative infections and improves overall surgical outcomes [10]. However, there is controversy regarding the association of elevated HbA1c, which shows the mean plasma glucose concentration (Figure 6) and postoperative SSI or PJI in TJA procedures [11].
Most of the current literature supports that elevated HbA1c levels contribute to postoperative complications after TJA. On the other hand, there are also studies in which there is no association between high HbA1c levels and postoperative SSI or PJI [12]. According to the guidelines of the American Diabetes Association (ADA), the HbA1c levels should be lower than 7% (53mmol/mol) to reduce postoperative complications [13]. However, the optimal HbA1c cut-off value is still controversial in the orthopedic literature. In this context, we conducted this single-center prospective study to determine the prevalence of undiagnosed and uncontrolled diabetes and to investigate the association between postoperative wound complications or SSI/PJI and elevated HbA1c in patients with TJA. In addition, the aim was to identify the HbA1c threshold for postoperative complications in patients undergoing TJA. We showed that routine preoperative determination of HbA1c to avoid possible postoperative injuries or infectious complications is still controversial. Larger studies on optimal HbA1c levels and other predictors are needed.
References
-
Yang L, Sun Y, Li G, Liu J (2017) Is hemoglobin A1c and perioperative hyperglycemia predictive of periprosthetic joint infection following total joint arthroplasty?. Medicine (Baltimore) 96(51): e8805.
-
Kunutsor S, Iorio R, Feng JE, Cizmic Z (2018) Prevention: Host Related, General Factors.
-
Cancienne JM, Werner BC and Browne JA (2017) Is there a threshold value of hemoglobin A1c that predicts risk of infection following primary total hip arthroplasty. J Arthroplasty 32(9): S236-S240.
-
Amin NH, Speirs JN, Simmons MJ, Lermen OZ, Cushner FD, et al. (2018) Total Knee Arthroplasty Wound Complication Treatment Algorithm: Current Soft Tissue Coverage Options. The Journal of Arthroplasty 34(4): 735-742.
-
Gaine WJ, Ramamohan NA, Hussein NA, Hullin MG, McCreath SW (2000) Wound infection in hip and knee arthroplasty. J Bone Joint Surg Br 82(4): 561-565.
-
Meding JB, Reddleman K, Keating ME, Klay A, Ritter MA, et al. (2003) Total Knee Replacement in Patients With Diabetes Mellitus. Clinical Orthopaedics and Related Research 416: 208-216.
-
Stephen EP, Stern SH, Insall JN, Windsor RE, (1990) Total Knee Arthroplasty in Diabetes Mellitus. Clinical Orthopaedics and Related Research 260: 130-134.
-
Han HS, Kang SB (2013) Relations between long- term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin Orthop Surg 5(2): 118-123.
-
Chrastil J, Anderson MB, Stevens V, Anand R, Peters CL, et al. (2015) Is hemoglobin A1c or perioperative hyperglycemia predictive of periprosthetic joint infection or death following primary total joint arthroplasty?. J Arthroplasty 30(7): 1197-1202.
-
Hwang JS, Kim SJ, Bamne AB, Na YG, Kim TK (2015) Do glycemic markers predict occurrence of complications after total knee arthroplasty in patients with diabetes? Clin Orthop Relat Res 473(5): 1726-1731.
-
Shohat N, Muhsen K, Gilat R, Rondon AJ, Chen AF, et al. (2018) Inadequate glycemic control is associated with increased surgical site infection in total joint arthroplasty: a systematic review and metaanalysis. J Arthroplasty 33: 2312-2321.e3.
-
Adams AL, Paxton EW, Wang JQ, Johnson ES, Bayliss EA, et al. (2013) Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001 to 2009. J Bone Joint Surg Am 95(6): 481-487.
-
Baek SH (2014) Identification and preoperative optimization of risk factors to prevent periprosthetic jointinfection. World J Orthop 5: 362-367.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results