Retrospective Review of Pediatric Fractures at King Hussein Medical City, Amman
Introduction: Pediatric bones possess unique anatomical and biomechanical characteristics distinct from adult bones, resulting in specific fracture patterns, healing potential, and treatment. Lower density, higher porosity, and extensive capillary infiltration characterize childhood bone. Diagnosing pediatric fractures can be challenging due to variations in ossification centers, often leading to delayed presentations. Definitions of "children" vary across organizations, influencing research methodologies. Methods: This retrospective study analyzed clinical and radiological records of pediatric patients admitted to the Royal Rehabilitation Center (RRC) at King Hussein Medical City (KHMC) in Amman, Jordan, from July 2020 to December 2023. Patients included were those under 18 with documented injury causes and available radiographs. However, we excluded patients who were discharged from the emergency department, those readmitted for re-operation, and those with poorly recorded injury mechanisms. Results: The study included 863 patients, with males constituting two-thirds. The mean patient age was 8.9 years. School-age children were the most affected, with a slight gender variation in age peaks. Left extremity fractures predominated, and the axial skeleton accounted for 7% of fractures. Simple falls were the leading injury mechanism (68.8%), followed by falls from height (16.6%) and road traffic accidents (6.4%). Upper limb fractures were most common (64.7%), especially distal humerus fractures (40%), followed by forearm shaft fractures (11.2%). High-energy injuries were more prevalent in older children, with distinct fracture patterns linked to specific injury mechanisms. Discussion: This study sheds light on pediatric fractures in Jordan, highlighting key differences in activity levels and risktaking behaviors between genders. While simple falls were most common, older children experienced more high-energy injuries. The findings emphasize the need for targeted injury prevention strategies for school-age children, including safer play environments, use of protective gear, and increased awareness among parents and caregivers about common injury risks.
Almigdad A¹* and Megdadi N²
¹Department of Orthopedic, Royal Medical Services, Jordan ²Department of Pediatric, Royal Medical Services, Jordan Keywords: Pediatric; Fracture; Bone; Jordan
Abbreviations
RRC: Royal Rehabilitation Center; KHMC: King Hussein Medical City; NIH: United States National Institutes of Health; UNICEF: United Nations International Children’s Emergency Fund; EU: European Union; FDA: Food and Drug Administration; PACS: Picture Archiving and Communication System.
Introduction
Pediatric bone has unique anatomical and biomechanical characteristics compared to adult bone, leading to specific fracture patterns, healing mechanisms, and treatment. Childhood bone has much lower density, higher porosity, and is extensively infiltrated by capillary channels [1]. The patterns of fractures in children differ depending on the cause of the damage and the level of skeletal development. Diagnosing these fractures can be challenging due to the resulting changes in the appearance of the ossification centers. Consequently, certain instances of fractures in children may go unrecognized and be presented at a later stage [2].
Various organizations have different definitions of “children”. The United States National Institutes of Health (NIH), the United Nations International Children’s Emergency Fund (UNICEF), and the European Union (EU) consider individuals under 18 as children. However, the United States Food and Drug Administration (FDA) defines pediatric patients as those from birth through age 21. The American Academy of Pediatrics states that the maximum age for pediatric treatment is adaptable and depends on the specific patient [3, 4, 5]. The “child” filter on PubMed encompasses individuals aged 0-18, whereas the “adult” filter encompasses those aged 19 and above [6]. When doing research, writers may use different age ranges according to their personal preferences.
This study aims to analyze fracture patterns and causes in Jordanian pediatric patients to understand injury incidence and characteristics. By identifying common fracture types and risk factors, the research seeks to inform clinical and preventive practices specific to this population and provide insights into the healthcare system’s needs for managing these injuries, ultimately guiding targeted treatment and prevention strategies.
Methods
This study performed a retrospective analysis of the clinical and radiological records of all pediatric patients who were hospitalized to the Royal Rehabilitation Center (RRC) at King Hussein Medical City (KHMC) in Amman, Jordan, due to bone fractures. The study period spanned from July 2020 to December 2023.
The study included all patients under 18 years old who were admitted with fractures, provided the cause of injury was well-documented and radiographs were available in the Picture Archiving and Communication System (PACS). Clear documentation of injury mechanisms was essential to ensure that the data accurately reflected the circumstances of fracture occurrence, facilitating precise identification of patterns and associated risk factors. Patients were excluded if they were discharged directly from the emergency department due to inadequate record details, readmitted for re-operations because of complications such as infection, nonunion, or hardware failure, or if their injury mechanisms were poorly recorded, including cases related to sports injuries or violence. Excluding cases with ambiguous injury mechanisms was intended to improve data accuracy by focusing on well-defined injury circumstances, ensuring the reliability of pattern and mechanism classification.
Patient records were used to extract sociodemographic and clinical data, while radiographs were examined to investigate the sites and patterns of fractures. The data collected encompassed patient age, gender, mechanism of injury, type of fracture, and any accompanying injuries. The age groups were classified as follows: infants (≤1 year), toddlers (1-3 years), preschoolers (3-6 years), school-age children (6-12 years), and adolescents (12-18 years). High- energy injuries were specifically categorized as incidents involving falls from hieght and road traffic accidents, whereas low-energy injuries encompassed simple falls as falls from ground level.
Fractures were categorized into eleven bone groups, with the forearm, leg, hand, and foot each regarded as a single bone. The bones were categorized based on their anatomical position, with long bones being divided into proximal, shaft, and distal sections, and the spine fractures being classified as cervical, thoracic, or lumbar. Sacral and coccygeal fractures were classified along with pelvic fractures because to their frequent association with pelvic injuries. Fractures of the hand and foot were classified as carpal and tarsal fractures, metacarpal and metatarsal fractures, and phalangeal fractures. Neurovascular and open injuries that were related to each fracture type were examined and assessed.
Statistical Data Analysis
Continuous variables were described using the mean and standard deviation, whereas categorical variables were described using frequency and percentages. The chi-squared test of independence was used to evaluate the associations between categorical variables. The data analysis was conducted using the SPSS IBM V21 statistical program, with a significance level of 0.05.
Results
Our study included 863 patients, with males representing two-thirds of the cases (66.6%), Table 1. The mean age of the patients was 8.9 years. School-age children were the most commonly affected group. However, there was a slight difference between females and males; in females, there was no age peak as seen in males. Left extremity fractures were more prevalent, affecting over half of the cases, while the right extremity was affected in 41.1%. The axial skeleton, including the spine and pelvis, accounted for 7% of all fractures. Simple falls were the most common mechanism of Total Female Male p-value Frequency 863 (100) 288 (33.4) 575 (66.6) Age ( years), mean (SD) 8.9 (4.7) 8.5 (5.2) 9.1 (4.5) Extremity Right 355 (41.1) 110 (38.2) 245 (42.6) 0.102 Left 448 (51.9) 144 (50) 304 (51.9) Axial 60 (7) 34 (11.8) 26 (4.5) Age groups Infant (≤1 year) 9 (1) 4 (1.4) 5 (0.9) injury (68.8%), followed by falls from height (16.6%). Road traffic accidents (RTA) accounted for 6.4% of all injuries. There were no statistically significant differences in the mechanisms of injury between the sexes.
- <0.001
- Toddlers ( 1 – 3 year)
- 115 (13.3)
- 51 (17.7)
- 64 (11.1)
- Preschool (> 3 – 5 years)
- 150 (17.4)
- 63 (21.9)
- 87 (15.1)
- School age children (6 – 12)
- 346 (40.1)
- 86 (29.9)
- 260 (45.2)
- Adolescent ( 13 – 18)
- 243 (28.2)
- 84 (29.2)
- 159 (27.7)
- Mechanism of Fracture
- Simple Falls
- 594 (68.8)
- 190 (66)
- 404 (70.3)
- Falls from height
- 143 (16.6)
- 56 (19.4)
- 87 (15.1)
- RTA
- 55 (6.4)
- 23 (8)
- 32 (5.6)
- Direct trauma
- 45 (5.2)
- 13 (4.5)
- 32 (5.6)
- Sport injury
- 21 (2.4)
- 6 (2.1)
- 15 (2.6)
- Others
- 5 (0.6)
- 0 (0)
- 5 (0.9)
Table 1: Bivariate Comparison between Male and Female Bone Injury Patients.
The distribution of fractures was as follows, Table 2: upper limb fractures were the most common, accounting for 64.7% of cases, followed by lower limb fractures at 28.3%.
Spine fractures occurred in 4.6% of all admissions, while pelvic fractures accounted for 2.4%. Upper limb fractures were more common in males than in females, with rates of
68% compared to 58%, respectively. In contrast, spine and pelvic fractures were more common in females, occurring at rates of 8.3% and 3.8% compared to 2.7% and 1.7% in males, respectively.
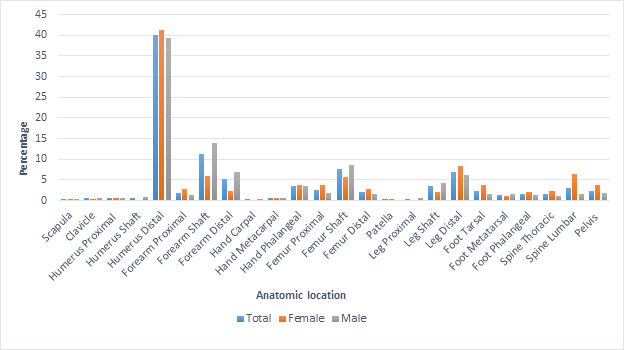
Distal humerus fractures were the most common, representing 40% of all admissions, followed by forearm shaft fractures, which accounted for 11.2%, femur shaft fractures at 7.6%, and distal leg fractures at 6.8%. The distribution of fractures differed between sexes, as shown in the Figure 1. For example, distal radius fractures accounted for 5.3% of all admissions. However, these fractures were more common in males than in females, with rates of 6.8% compared to 2.4%, respectively.
| Total | Female | Male | ||
|---|---|---|---|---|
| Upper Limb 558 = 167 + 391 | ||||
| Scapula | 2 (0.2) | 1 (0.3) | 1 (0.2) | |
| Clavicle | 4 (0.5) | 1 (0.3) | 3 (0.5) | |
| Humerus | ||||
| Proximal | 6 (0.7) | 2 (0.7) | 4 (0.7) | |
| Shaft | 5 (0.6) | 0 (0) | 5 (0.9) | |
| Distal | 345 (40) | 119 (41.3) | 226 (39.3) | |
| Forearm | ||||
| Proximal | 16 (1.9) | 8 (2.8) | 8 (1.4) | |
| Shaft | 97 (11.2) | 17 (5.9) | 80 (13.9) | |
| Distal | 46 (5.3) | 7 (2.4) | 39 (6.8) | |
| Hand | ||||
| Carpal | 1 (0.1) | 0 (0) | 1 (0.2) | |
| Metacarpal | 6 (0.7) | 2 (0.7) | 4 (0.7) | |
| Phalangeal | 30 (3.5) | 10 (3.5) | 20 (3.5) | |
| Lower Limb 244= 86+ 158 | ||||
| Femur | ||||
| Proximal | 22 (2.5) | 11 (3.8) | 11 (1.9) | |
| Shaft | 66 (7.6) | 16 (5.6) | 50 (8.7) | |
| Distal | 17 (2) | 8 (2.8) | 9 (1.6) | |
| Patella | 1 (0.1) | 1 (0.3) | 0 (0) | |
| Leg | ||||
| Proximal | 3 (0.3) | 0 (0) | 3 (0.5) | |
| Shaft | 30 (3.5) | 6 (2.1) | 24 (4.2) | |
| Distal | 59 (6.8) | 24 (8.3) | 35 (6.1) | |
| Foot | ||||
| Tarsal | 20 (2.3) | 11 (3.8) | 9 (1.6) | |
| Metatarsal | 12 (1.4) | 3 (1) | 9 (1.6) | |
| Phalangeal | 14 (1.6) | 6 (2.1) | 8 (1.4) | |
| Spine 40= 24+ 16 | ||||
| Cervical | 0 (0) | 0 (0) | 0 (0) | |
| Thoracic | 13 (1.5) | 6 (2.4) | 7 (1.2) | |
| Lumbar | 27 (3.1) | 18 (6.3) | 9 (1.6) | |
| Pelvis | 21 (2.4) | 11 (3.8) | 10 (1.7) | |
| Injury | Frequency | Females | Males | p-value |
| Open fracture | 68 (7.9) | 17 (5.9) | 51 (8.9) | 0.119 |
| Pathological fracture | 10 (1.2) | 5 (1.7) | 5 (0.9) | 0.276 |
| Vascular injury | 35 (4.1) | 8 (2.8) | 27 (4.7) | 0.292 |
| Neurological injury | 17 (2) | 5 (1.7) | 12 (2.1) | 0.724 |
Table 2: Bivariate Association between Patients’ Age and Associated Injuries with Injury Mechanism.
- Open fractures occurred in 7.9% of cases, while vascular and neurological injuries were associated with 4.1% and
- 2% of all fractures, respectively. Pathological fractures were diagnosed in 1.2% of cases. There was no significant difference between the sexes, (Table 3).
- Simple falls were the most common injury mechanism across all age groups. High-energy injuries, such as falls from height, road traffic accidents, direct trauma, and sports injuries, were more common in older children, including those of school age and adolescents (Table 4).
- Simple Falls
- Falls from height
- RTA
- Direct trauma
- Sport
- Others p-value
- Age ( years), mean (SD)
- 7.85 (4.3)
- 11.05 (4.8)
- 10.95 (5.4)
- 11.02 (4.9)
- 13.52 (2.9)
- 11 (5.7)
- Age groups (years)
- Infant (≤1 year)
- 7 (1.2)
- 2 (1.4)
- 0 (0)
- 0 (0)
- 0 (0)
- 0 (0)
- Toddlers ( 1 – 3 year)
- 94 (15.8)
- 8 (5.6)
- 8 (14.5)
- 4 (8.9)
- 0 (0)
- 1 (20)
- Preschool (> 3 – 5 years)
- 124 (20.9)
- 18 (12.6)
- 5 (9.1)
- 3 (6.7)
- 0 (0)
- 0 (0)
- School age children (6 – 12)
- 254 (42.8)
- 48 (33.6)
- 18 (32.7)
- 19 (42.2)
- 5 (23.8)
- 2 (40)
- Adolescent ( 13 – 18)
- 115 (19.4)
- 67 (46.9)
- 24 (43.6)
- 19 (42.2)
- 16 (76.2)
- 2 (40)
- Associated injuries*
- Open fracture
- 12 (1.4)
- 15 (1.7)
- 13 (1.5)
- 22 (2.5)
- 1 (0.1)
- 5 (0.6)
- < 0.001
- Pathological fracture
- 9 (1)
- 0 (0)
- 0 (0)
- 1 (0.1)
- 0 (0)
- 0 (0)
- 0.29
- Vascular injury
- 28 (3.2)
- 3 (0.3)
- 2 (0.2)
- 0 (0)
- 0 (0)
- 2 (0.2)
- 0.147
- Neurological injury
- 6 (0.7)
- 5 (0.6)
- 2 (0.2)
- 1 (0.1)
- 1 (0.1)
- 2 (0.2)
- 0.01
- * Numbers within bracket represents percentage within all injuries.
Table 3: Bivariate Association between Patients’ Age and Associated Injuries with Injury Mechanism.
<0.001 Table 4: Bivariate Association between Patients’ Age and Associated Injuries with Injury Mechanism.
Table 5 highlights the varying patterns of fractures based on the type of injury mechanism. It reveals that simple falls are responsible for half of all distal humerus fractures. Additionally, lumbar fractures are predominantly associated with falls from height. Road traffic accidents (RTAs) are a common cause of femur shaft and distal tibia fractures. On the other hand, direct trauma is more frequently linked to fractures of the hand and foot phalanges.
| Simple Falls | Falls from height | RTA | Direct trauma | Sport | Others | |
|---|---|---|---|---|---|---|
| Upper Limb | ||||||
| Scapula | 0 (0) | 2 (1.4) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Clavicle | 2 (0.3) | 2 (1.4) | 0 (0) | 0 (0) | 1 (4.8) | 0 (0) |
| Humerus | ||||||
| Proximal | 4 (0.7) | 1 (0.7) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) |
| Shaft | 2 (0.3) | 1 (0.7) | 0 (0) | 2 (4.4) | 0 (0) | 0 (0) |
| Distal | 307 (51.7)) | 33 (23.1) | 1 (1.8) | 2 (4.4) | 2 (9.5) | 0 (0) |
| Forearm | ||||||
| Proximal | 15 (2.5) | 0 (0) | 0 (0) | 0 (0) | 1 (4.8) | 0 (0) |
| Shaft | 77 (13) | 14 (9.8) | 0 (0) | 4 (8.9) | 2 (9.5) | 0 (0) |
| Distal | 33 (5.6) | 10 (7) | 2 (3.5) | 0 (0) | 1 (4.8) | 0 (0) |
| Hand | ||||||
| Carpal | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (20) |
| Metacarpal | 4 (0.7) | 0 (0) | 0 (0) | 1 (2.2) | 0 (0) | 1 (20) |
| Phalangeal | 8 (1.3) | 1 (0.7) | 0 (0) | 19 (42.2) | 0 (0) | 2 (40) |
| Lower Limb | ||||||
| Femur | ||||||
| Proximal | 13 (2.2) | 4 (2.8) | 1 (1.8) | 0 (0) | 4 (19) | 0 (0) |
| Shaft | 34 (5.7) | 10 (7) | 15 (27.3) | 2 (4.4) | 5 (23.8) | 0 (0) |
| Distal | 10 (1.7) | 2 (1.4) | 4 (7.3) | 0 (0) | 1 (4.8) | 0 (0) |
| Patella | 1 (0.2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Leg | ||||||
| Proximal | 3 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Shaft | 12 (2) | 9 (6.3) | 7 (12.7) | 2 (4.4) | 0 (0) | 0 (0) |
| Distal | 36 (6.1) | 6 (4.2) | 11 (20) | 2 (4.4) | 4 (19) | 0 (0) |
| Foot | ||||||
| Tarsal | 5 (0.8) | 12 (8.4) | 2 (3.6) | 0 (0) | 0 (0) | 1 (20) |
| Metatarsal | 9 (1.5) | 1 (0.7) | 0 (0) | 2 (4.4) | 0 (0) | 0 (0) |
| Phalangeal | 8 (1.3) | 0 (0) | 1 (1.8) | 5 (11.1) | 0 (0) | 0 (0) |
| Spine | ||||||
| Cervical | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Thoracic | 2 (0.3) | 9 (6.3) | 0 (0) | 1 (2.2) | 0 (0) | 0 (0) |
| Lumbar | 5 (0.8) | 15 (10.5) | 5 (9.1) | 2 (4.4) | 0 (0) | 0 (0) |
| Pelvis | 4 (0.7) | 11 (7.7) | 4 (7.3) | 1 (2.2) | 1 (4.8) | 0 (0) |
Table 4: Bivariate Association between Bone Fractures with Injury Mechanism. Discussion There is a lacking of epidemiological stu
This review focuses solely on orthopedic fracture admissions that occur within the hospital, excluding cases that are managed conservatively and discharged from the emergency department. This suggests that the reported incidence of fractures may be lower than the actual occurrence. Considering KHMC’s position as a tertiary and referral center, it is anticipated that the occurrence of complex fractures, pelvic fractures, spine fractures, and fractures linked to vascular injuries will be higher.
Our study included 863 patients and provides a thorough examination of fracture patterns and injury mechanisms in pediatric patients in Jordan. In one study from the same center, pediatric fractures represented 23.9% of all admissions to the orthopedic ward across all age groups [7]. The gender disparity may be attributed to the differing activity levels and risk-taking behaviors observed among boys and girls. Notably, males experienced a significant increase in injury rates during their school years (ages 6 to 12), whereas females did not demonstrate a corresponding age-related peak. These findings suggest possible variations in exposure and activity patterns between genders. However, it remains uncertain if this distribution is representative of all fractures seen in the emergency room, as our review only examined admitted patients. Inadequate documentation of injury mechanisms and broad categorization of injuries further complicate interpretation. For example, injuries from falls higher than ground level are categorized as “falling from height,” while falls from ground level are referred to as “simple falls.” Nevertheless, there were no significant variations between genders in terms of injury mechanisms.
Patients admitted for fractures are typically hospitalized for either observation or surgical intervention, which contributes to variations in fracture frequencies observed. For example, there is a higher frequency of fractures requiring surgery compared to those treated and discharged from the emergency room. In the upper limb, distal humerus fractures were the most common in our review, significantly outnumbering distal radius fractures. This disparity arises because many distal radius fractures are managed conservatively and discharged from the emergency room, whereas fractures of the distal humerus, such as supracondylar and lateral condyle fractures, often require surgical intervention.
Similarly, femur shaft fractures were more frequent in our review compared to more common fractures of the leg shaft and distal leg. This is due to the fact that patients with femur shaft fractures are typically admitted for observation or surgical management, whereas many leg fractures can be discharged directly from the emergency room.
In contrast, fractures of the spine and pelvis typically require hospitalization, which accurately reflects their actual occurrence. Nevertheless, it is worth noting that the prevalence of these fractures at our center may seem higher than the actual population rates. This is primarily because our hospital specializes in providing the necessary care for such cases, which often requires referrals from other healthcare facilities.
Cervical spine injuries at our institution are managed by the neurosurgery team in a separate unit, which is why they are excluded from our data. The majority of cases (64.7%) involved upper limb fractures compared to lower limb fractures, likely due to the natural tendency to use the hands to break falls.
Gender differences in fracture types may be explained by anatomical and physiological variations between boys and girls, as well as differences in their physical activities. Socially, boys are more likely to engage in high-risk or physically intense activities, such as sports and climbing, while girls participate in activities associated with lower physical risks.
There is a higher incidence of left limb involvement compared to the right limb, which is likely attributed to the prevalence of right-handedness in approximately 90% of the population. Injuries are more likely to happen in the dominant limb because it is used more actively. On the other hand, the non-dominant limb often takes on a protective role, which can result in more indirect injuries to that limb [8, 9]. This phenomenon mainly pertains to injuries in the upper extremities and, to a certain degree, in the lower extremities as well.
Evaluating injury mechanisms across age groups reveals important insights into sociocultural and environmental factors influencing injury patterns among Jordanian pediatric patients. Simple falls emerged as the most common cause of fractures across all age groups, possibly reflecting a lack of protective or structured environments for young children, such as well-maintained playgrounds or child- safe recreational spaces. Assessing whether playgrounds are equipped with safety measures—such as soft landing surfaces and proper equipment maintenance—could clarify whether these spaces contribute to injuries.
In older children and adolescents, high-energy traumas, including falls from heights and road traffic accidents, were notably more prevalent. This trend may relate to social factors, such as adolescents engaging more often in unsupervised activities or using roads with insufficient safety infrastructure, especially in rural or densely populated urban areas where pedestrian and vehicular interactions pose risks. Safety education programs or encouraging the use of protective equipment could help reduce these incidents.
Direct trauma, such as injuries from using hammers or other heavy objects, was observed in younger adolescents (mean age 11), possibly reflecting engagement in household tasks or responsibilities involving tools. This trend suggests that family dynamics or community expectations may contribute to early exposure to risk-prone activities, often without appropriate safety training or supervision. Additionally, sports-related injuries were more common in older children (mean age around 14), indicating greater involvement in recreational or competitive sports. If organized sports settings—such as schools or local facilities—lack adequate safety guidelines, supervision, or protective equipment, these factors may contribute to the higher injury rates in this group.
Examining these potential sociocultural and environmental influences can guide targeted interventions, such as improved playground safety standards, enhanced education on safe tool use, and stronger regulations around sports facilities and equipment. Understanding these contextual factors is essential for developing effective, culturally relevant injury prevention strategies tailored to Jordanian children’s needs.
Open fractures are commonly linked to high energy trauma, such as direct trauma or falls from heights. The increased occurrence of neurovascular injuries resulting from simple falls can be attributed to the higher frequency of these mechanisms, rather than a direct causal relationship.
When studying mechanisms of injury and their correlation with fractures, it was found that lumbar fractures were mainly associated with high-energy events, such as falls from height. RTAs often result in femur shaft and distal tibia fractures. Additionally, there is a strong correlation between direct trauma and fractures of the hand and foot phalanges.
This study emphasizes the importance of implementing focused injury prevention strategies, particularly for children of school age. Public health initiatives should focus on establishing safer play environments, encouraging the use of protective gear, and increasing awareness among parents and caregivers regarding common injury risks. Gender-specific interventions may be advantageous because boys and girls exhibit distinct fracture patterns and engage in different activities. Additional research is required to gain a deeper understanding of the underlying causes behind these disparities between genders, as well as to create tailored approaches for prevention and treatment. It is advisable to conduct longitudinal studies in order to obtain a more comprehensive understanding of the long- term consequences of pediatric fractures and the efficacy of current treatment methods.
Limitations of the Study
This study’s retrospective design introduces several limitations that may impact the depth and generalizability of the findings. The use of data from a single center, the Royal Rehabilitation Center at King Hussein Medical City, potentially introduces selection bias, as the study sample may not fully represent the broader Jordanian pediatric population. Children with fractures who did not require hospitalization, or those treated at other facilities, were not included, which may limit the findings’ applicability to a wider context. To improve generalizability, future studies could include data from multiple centers or community clinics.
Additionally, limitations in the documentation of injury mechanisms within the archival system restrict the ability to analyze specific causes of fractures comprehensively. Injury mechanisms were categorized broadly (e.g., simple falls, falls from height, traffic accidents), which may obscure more detailed factors influencing fracture risk. Implementing mandatory fields for detailed injury descriptions in electronic medical records would help future research more accurately identify specific risk factors and design targeted prevention strategies.
The broad classification of fractures by anatomical regions (e.g., forearm, hand, leg, foot) also limits the ability to analyze individual fractures in detail. Regional analyses focused on specific fracture sites or areas, such as upper extremity fractures or fractures at particular anatomical locations, would yield a more granular understanding of fracture patterns. Addressing these limitations in future research could enhance the study’s relevance and provide stronger evidence to inform public health interventions and clinical practices tailored to the Jordanian pediatric population.
Conclusions
This study provides key insights into the epidemiology of pediatric fractures in Jordan, revealing notable patterns and risk factors that underscore the importance of targeted prevention strategies. The high incidence of fractures among males, the predominance of upper limb injuries, and the prevalence of simple falls as a primary mechanism of injury point to the need for comprehensive, community- wide preventive measures. To address these trends, public health initiatives could include school-based programs that promote safe play practices and educate children on fall prevention techniques. Additionally, community and parent education programs can emphasize the importance of protective measures in sports and recreational activities, especially for boys who are at higher risk of high-energy trauma. Collaborating with schools, community centers, and local governments to implement safety protocols in playgrounds, sports facilities, and other recreational areas may also reduce the incidence of injuries. By focusing on these specific fracture patterns and mechanisms, targeted interventions can help reduce the burden of pediatric fractures and improve safety for children across Jordan.
References
-
Calmar EA, Vinci RJ (2002) The anatomy and physiology of bone fracture and healing. Clinical Pediatric Emergency Medicine 3(2): 85-93.
-
Hussain S, Dar T, Beigh AQ, Dhar S, Ahad H, et al. (2015) Pattern and epidemiology of pediatric musculoskeletal injuries in Kashmir valley, a retrospective single-center study of 1467 patients. J Pediatr Orthop B 24(3): 230- 237.
-
(2019) Guidelines for the review of inclusion on the basis of sex/gender, race, ethnicity, and age in clinical research. United States National Institutes of Health, USA, pp: 1-8.
-
(1989) Convention on the rights of the child. United Nations International Children’s Emergency Fund (UNICEF).
-
(2022) EU action on the rights of the child. European Commission.
-
(2022) PubMed user guide. National Library of Medicine
-
Almigdad A, Alazaydeh A, Alshawish M, Alfukaha H, Mustafa MB, et al. (2022) An Epidemiological Analysis of Orthopedic Fractures, a Retrospective Single-Center Study from Jordan. International Journal of Orthopaedics Research (IJOR) 5(4): 126-134.
-
Scharoun SM, Bryden PJ (2014) Hand preference, performance abilities, and hand selection in children. Front Psychol 5: 82.
-
Papadatou-Pastou M, Ntolka E, Schmitz J, Martin M, Munafò MR, et al. (2020) Human handedness: A meta- analysis. Psychol Bull 146(6): 481-524.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results