Epidemiology and Economics of Osteoporosis Management
Osteoporosis is a major public health concern globally more so in India, with a notable increase in hip fractures, among males and Postmenopausal women. These fractures occur 10 to 20 years earlier in the Indian population with peak incidence between 50 to 60 years. The fact that 30% of fracture patients in India die within a year indicates the severity. A meta-analysis of studies from 2010 to January 2021, reported a pooled prevalence of osteoporosis at the lumbar spine region and the femoral neck region as 29%, the hip region as 6%. Similarly, the pooled prevalence of osteopenia at the lumbar spine region and femoral neck region is reported to be 37% each, and the hip as 6%. Osteoporosis diagnosis primarily involves assessing bone mineral density (BMD). In India current guidelines recommend osteoporosis screening for individuals over 65, and postmenopausal women, over 50 years. Lower BMD scores are linked to higher fracture risk, in older adults. For example, at age 50, a T-score of -2.5 correlates to a 12% fracture risk, which can double or triple by age 70. Materials and Methods: An unpleasant surprising diagnosis of osteoporosis in author’s wife following unintended BMD Test is the trigger for this article, complimented by extensive literature review, about the latest treatment approaches. Currently the patient is under treatment with both traditional (Calcium and Vitamin D supplementation) and modern treatment with Denosumab (DENU) a Monoclonal antibodies subcutaneous injection, the cost of which is forbidding for an average Indian. Outcome: The Denu injection was well accepted by the patient with only minor adverse reaction of local pain and fever for a day. Though costly modern treatments is worth investing in elderly post-menopausal women’s Healthy ageing and Healthy Average Life Expectancy (HALE) of women in the country.
Abbreviations
BMD: Bone Mineral Density; HALE: Healthy Average Life Expectancy; BDT: Bone Density Test; DALYs: Disability- Adjusted Life-Years; CQUS: Calcaneal Quantitative Ultrasound; PTH: Parathyroid Hormone; SERMs: Selective Estrogenic Receptor Modulators.
Introduction
Skeleton is a dynamic tissue, getting remodelled constantly throughout life. Compact and cancellous bones are arranged in a fashion to provide tensile strength & density for mobility and protection of the body. Remodelling is achieved by two different cell types: osteoblasts, which synthesize bone matrix, and osteoclasts, which reabsorb it. Osteoporosis in postmenopausal women has been epidemiological studied and a correlation between cardiovascular disease and osteoporosis has been established. There is paucity of studies done for detection of osteoporosis in premenopausal women, and men [1].
The world’s population is aging rapidly, and in 2024, 10.3% of the global population is estimated to be 65 or older, which indicates to have doubled in last 50 years from 1974. It is projected to double again by another 50 years i.e., 2074. As the incidence of osteoporosis is linked to ageing population especially among menopausal women currently roughly 30% of all postmenopausal women are suffering from Osteoporosis and about 40% of these women and another 15–30% of men over 65 years are likely to sustain one or more fractures of wean bones in their remaining lifetime. Fractures of weak and long bones in elderly are a major health challenge contributing to sickness, disability, and increased mortality worldwide. Osteoporosis is a bone disease that causes bones to become weak and prone to break due to reduction in the amount and thickness of bone tissue when the structure or quality of bone changes due to low bone mass or micro-architectural deterioration of bone tissue among post-menopausal women over 50 yrs and men over 60 years [2, 3].
With an estimated population of 1,450,935,791 as on 31 December 2024 India has approximately 250 million over the age of 50 years. Indian comprehensive data for Osteoporosis prevalence is lacking and most of most of our data comes from smaller studies or hospitals across the country. A study in 2021 reported overall prevalence of osteopenia of 50% and osteoporosis 18.3% and in men it was 19.7% in the South India and 15.0% in the North India [4]. Another study reported a prevalence of osteoporosis to be 33.1% among postmenopausal women with an overall prevalence of 18.3% all in women [3], while the global prevalence of osteopenia is estimated to be 40.4%, in India it is the highest at 50%. The global osteopenia among 18-year-old group is estimated to be 21.47% and the same at 75-year-old group 56% [5]. The high prevalence of osteopenia at younger age, leads to increased osteoporotic fractures in 10–12 years younger Indian population than global most Western countries. Globally, there were about 8.6 million cases of vertebral fractures in 2019, of which India contributed nearly half. In India, more than 250,000 people sustain a hip fracture every year due to osteoporosis and 40% of them die within one year [2, 5], Despite marked advances in diagnosis and treatment for osteoporosis, very few patients receive appropriate treatment, even after a fracture [5].
This article is an outcome of an unpleasant but surprising diagnosis of osteoporosis in author’s wife following an unintended BMD Test. The accidental finding led to a literature review, learning and treatment with modern approaches. The cost appears to be forbidding for an average Indian woman, but it is worth the individual and national health mission investing in elderly post-menopausal women’s Healthy ageing and Healthy Average Life Expectancy (HALE) of women in the country.
Case Report
Mrs Prabha, the author’s spouse underwent and Bone density test (BDT) along with a routine annual Mammography being done a preventive screening for last 20 years. To my utter and unpleasant surprise her BD Test report of 5 December 2024 read as following (Table 1).
| Measure type | Region | BMD | T Score | Z Score | Classification |
|---|---|---|---|---|---|
| Spine | L1-L4 | 0.783g/cm2 | -2.4 | 0.7 | Severe Osteopenia |
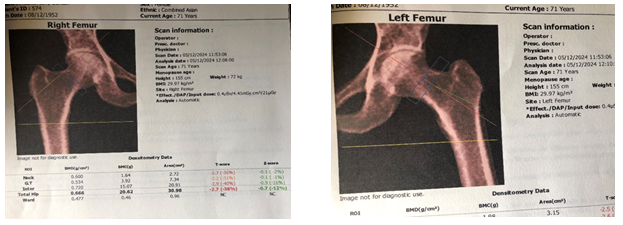
| Right Femur | Total Hip | 0.666/ cm2 | -2.7 | -0.7 | Osteoporosis |
| Right Femur | Neck | 0.600/ cm2 | -2.7 | -0.1 | Osteoporosis |
| Left Femur | Total Hip | 0.655/ cm2 | -2.6 | -0.6 | Osteoporosis |
| Left Femur | Neck | 0.600/ cm2 | -2.5 | -0.1 | Osteoporosis |
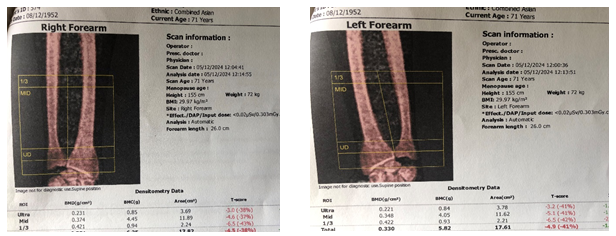
| Right Forearm | Mid-Ultra.1/3 | 0.351./cm2 | -4.5 | -1 | Osteoporosis |
| Left Forearm | Mid-Ultra.1/3 | 0.330./cm2 | -4.9 | -1.5 | Osteoporosis |
Table 1: Mrs Prabha Bone density test report results.
Note: T Score +1 to –1= Healthy Bone Density, -1 to-2.5= Osteopenia & -2.5 to-3= Osteoporosis. T Score: Represents the difference between the patient BMD and the average value of a young and healthy adult with same sex and ethnic group (Asian) Z Score: Represents the difference between the patient BMD and the average value for same age population There were clear signs of Osteoporosis in all sites except the Lumbar spine at L1-L4 level which also had severe Osteopenia (Figure1).
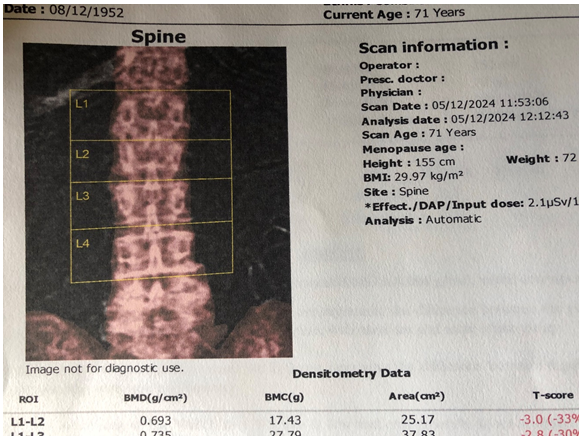
Bone density images were clearly indicating either Osteoporosis or severe osteopenia. Radiologist suggested initiation of immediate modern treatment costing about 28,000 INR monthly for about a year (Figure 2 & 3).
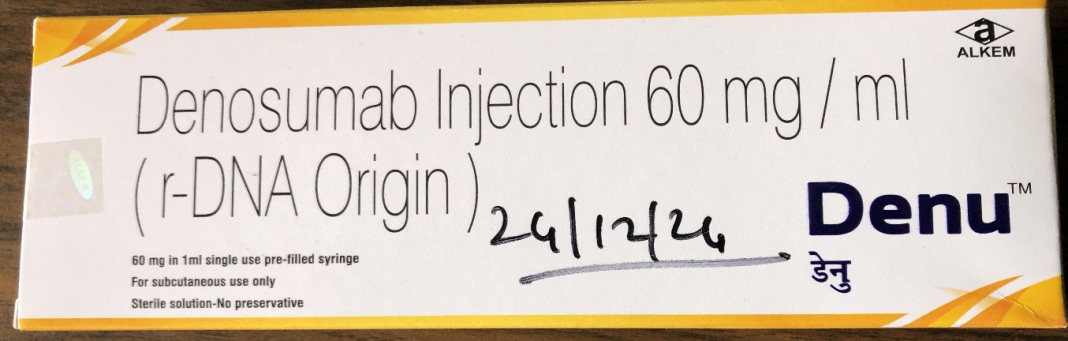
On return to Bengaluru, consulted a renowned Orthopaedic Surgeon who agreed to radiological diagnosis but said that in the absence of symptoms of pain etc, there is no big concern. He has put her on Tab. Supracal 2000 (a combo of Calcium, Vitamin D3, Methylcobalamin, Magnesium and Zinc) supplements from 10 December and Injection Denu at 6 monthly intervals. The first injection was given on 24 December 2024, except for a day’s discomfort, there have been no adverse reactions (Figure 4).
Discussions
Bone, a dynamic tissue in the human body remodels itself, preserving serum calcium, repairing microdamage, and maintaining strength. A decrease in bone strength, manifests clinically as low-energy vertebral and non-vertebral fractures attributable to Osteoporosis.
Osteoporosis, is linked to the aging process, identified as a widespread inflammatory bony tissue loss condition, with its prevalence increasing with age, therefore prevalence is further intensified due to global longevity of life and increasing aging population [2], India, with 1.45 billion people, 250 million among them aged of 50 and beyond, ranked first amongst 204 countries with the highest disability-adjusted life-years (DALYs) burden and death due to low bone mineral density (BMD)-related fractures [2, 3], A study conducted across India reported that osteoporosis & osteopenia affect 20% and 50% individuals respectively and 40% of elderly women and one third elderly men are suffered with osteoporosis [2].
Postmenopausal osteoporosis is a major public health problem around the world. It is characterized by microarchitectural bone tissue deterioration and bone mass loss or porous bone, a hallmark that, increases bone breakage risk [1], About 9 million fractures are caused annually by osteoporosis worldwide, and more than 4.5 million of them occurring in America Europe and India. It affects about a quarter of women aged 50–84 years, affecting over 12 million women in Germany, France, Italy, Spain, and the United Kingdom [3], in developing countries, the lifetime risk of a fracture of wrist bones, femur in hip, or vertebral column is closer to the risk of heart disease of 30% and 40%, [4].
Signs & Symptoms: Osteopenia and osteoporosis are conditions that cause bone loss, and symptoms can be non- existent or subtle in the early stages. Osteopenia’s common symptom is height loss, a sign of bone health issues. Other symptoms to suspect include stress fractures in the feet during normal activity. Osteoporosis on the other hand can also be symptomless and remains undetected until a fracture occurs after a minor fall or accident. Other explicit symptoms include a stooped posture, loss of height of two inches or more, back pain, in the mid or lower back, shortness of breath if the spine is compressed.
Recent research has highlighted that individuals’ reporting falls within the past year faced significantly heightened risks of various types of fractures, including clinical, osteoporotic, major osteoporotic, and hip fractures. Interestingly, men exhibited greater predictive values compared to women, and this increased fracture risk tied to prior falls remained significant even after accounting for bone mineral density, underscoring falls’ independent role as a risk factor. Integrating this insight into tools like Fracture Risk Assessment (FRAX) Tool holds potential to improve predictive precision, aiding healthcare professionals in better assessing fracture risk and customizing preventive measures to optimize patient outcomes [6].
Risk Factors: Indian observational studies point to certain risk factors for developing osteoporosis such as i) Being female ii) Being over the age of 35in general and over 60 year in men iii) Having a smaller, thinner frame iv) Having Asian ancestry, v) Having a history of poor nutrition especially Calcium and Vit D deficiency, vi) Having a sedentary lifestyle, vii) Smoking viii) Consuming alcohol ix) Going through menopause and x)Having thyroid disease. Medical conditions-like Cushing’s disease, medications like steroids or immunosuppressants, also elevate risk, but symptoms can include back pain, loss of height, and recurrent fractures with minimal trauma [2, 5, 6, 7, 8, 9].
Dyslipidaemia- A Risk Factor for Osteoporosis in Women: A study conducted at Lady Hardinge Medical College, New Delhi for six months from November 2013 of 60 patients (30 premenopausal and 30 postmenopausal) with no comorbidity and not using any drugs influencing lipid or bone metabolism were evaluated for lipid profile and BMD [10]. This study reported that in premenopausal women, there was a negative correlation between very low-density lipoprotein cholesterol (VLDL-C), triglycerides (TGs) and Lumbar Vertebral BMD (VLDL-BMD r -0.363, p = 0.049; TRI- BMD r -0.363, p = 0.049), but a statistically significant positive correlation between high-density lipoprotein cholesterol (HDL-C) and BMD –(HDL-BMD r 0.359, p = 0.05). Similarly, in postmenopausal women, the negative correlation between VLDL, TG, and BMD was statistically significant (TG-BMD r -0.377, p = 0.04; LDL-BMD r 0.415, p = 0.02), as was the positive correlation between HDL and T-score (HDL-BMD r 0.366, p = 0.04). Thus, Lipid profile variables showed a significant association with BMD to use them as risk factors for osteoporosis [10].
Osteoporosis Diagnosis: A bone density test, called “dual emission x-ray absorptiometry (DEXA) scan” of the spine, hips and forearms is necessary to confirm the diagnosis of osteoporosis or osteopenia, as was done in our case. The test measures bone mineral density (BMD) of the candidate & compares it to the average for people of the same age, sex, and race. A T-score between -1 and -2.5 indicates osteopenia, and a t-score of -2.5 or lower indicates osteoporosis. A portable X ray machine, measures bone density in the wrist and heel, but the results are not reliable. Current guidelines recommend osteoporosis screening for individuals over 65, postmenopausal women- over 50 yrs [2].
Data obtained from in-clinic screening camps conducted among apparently healthy adults (aged 18 years and above) for the prevalence of both osteopenia and osteoporosis at national and regional levels in India, of bone mineral density (BMD) using Calcaneal quantitative ultrasound (CQUS) of left foot. Among a total, of 31238 participants with mean age of 47.8±14.2 years, 47.6% were females and mong them,38.8% were postmenopausal women (age >50 years). Overall prevalence of osteopenia and osteoporosis was 49.9% and 18.3% respectively. The highest prevalence of osteopenia of 55.6% was in North, followed by East-51.3%, West- 47.9%, and 47.4% in South India. Similarly, prevalence of osteoporosis was N=20.7%, E= 18.4, W=16.3, and S=16.4 respectively. Osteoporosis was slightly higher in females than males (19.4 vs 17.3%). Among high-risk population - postmenopausal women, overall osteoporosis was 33.1% and ranged from 16.9% in North region to 21.8% in South region. Prevalence of osteoporosis in elderly (≥60 years) was 37.0% compared to just 12.5% than in adults (<60 years) [8].
Management of Osteopenia: Osteopenia is a condition of low bone density, doesn’t necessarily mean bone will break, but it is a risk factor. The condition is usually managed through lifestyle changes, exercise, and supplements [4]: Diet: A well-balanced diet that’s rich in calcium, with a daily intake of 1G for adult men and women and 1.3 G for women over 50 and men over 70. One can get some calcium from dairy products like yogurt, low-fat milk, and cheese. Vitamin D: Though getting it through safe exposure to sunlight, given the current lifestyle of most people find it difficult. A 30 minutes of sun exposure in the summer, or slightly longer in the winter, between 10 am and 3 pm, as the UVB rays are strong in these hours, therefore, the body produces vitamin D more quickly. Everyone must avoid UV index above 3. Alternately taking a supplement after a Lab’s Biomarker test confirms a deficiency. Exercise: Weight-bearing, resistance, and balance exercises strengthen our bones and muscles. Activities like walking, yoga, Pilates, and tai chi improve our balance and strength without putting too much stress on bones. Supplements: Take calcium or vitamin D supplements if found deficient after a lab test as recommended by a doctor. Other lifestyle changes: Stop smoking, limit alcohol consumption, and minimize steroid dosages.
Management of Osteoporosis
Non-Pharmacologic Management: Non-pharmacologic strategies are like those listed for Osteopenia and include dietary measures such as consuming low-fat dairy products, high-protein foods, and vegetables. Regular physical activity, particularly weight-bearing and muscle-strengthening exercises, are crucial for enhancing bone strength and minimizing the risk of falls leading to fractures. However, activities involving heavy lifting should be avoided by those with spinal osteoporosis [4].
Pharmacologic Treatments: Treatment options include hormonal therapies like estrogenic therapy, though these may vary in effectiveness and can lead to side effects. Bisphosphonates are commonly used to stabilize bones, while parathyroid hormone (PTH) and selective estrogenic receptor modulators (SERMs) may be considered in specific cases. Calcitonin is used primarily for pain relief, with limited effects on bone density improvement.
Bisphosphonates treat osteoporosis by slowing or stopping the process of bone resorption, which is the breakdown of old bone cells. Bisphosphonates attach to hydroxyapatite binding sites on bones, particularly in areas where bone resorption is active. They are then absorbed by osteoclast cells, which break down old bone, and their activity is reduced. This slows down bone breakdown and helps prevent bones from losing calcium and other minerals. Studies have inferred that bisphosphonates can reduce the risk of breaking vertebrae by up to 50% and other bones by 30-49%. Bisphosphonates come as a weekly pill called Alendronate (Raloxiheal= Raloxifenes Hydrochloride Tablets IP 60 Mg or OsteoCare Tablet 70 mg), OsteoCare Tablet 70 mg Or Osteofit HD, - A weekly or monthly pill, Ibandronate (Boniva): A monthly pill or quarterly intravenous (IV) infusion and Zoledronic acid (Reclast, Zometa): An annual IV infusion. Oral Bisphosphonates should be taken after an overnight fast, with only water, 30 to 60 minutes before eating or drinking anything else [4].
Advanced Therapeutic Options: Advanced therapies include Romosozumab, Denosumab and teriparatide, administered as subcutaneous injections. Denosumab, given biannually, has been shown to increase spinal BMD by 9% and hip BMD by 4-5% over two years use. significantly reducing fracture risks. Teriparatide, taken daily for up to two years, enhances BMD by 9-13% and reduces vertebral fracture incidence. Both treatments require careful consideration of contraindications, such as hypocalcaemia, and patient education on proper administration and potential side effects.
Denosumab: Denusumab known as Denu is a human monoclonal immunoglobulin G2 (IgG2) antibody that binds to RANKL, the principal regulator of osteoclastic bone resorption. Denu is the cheapest at a cost of 8500/injection followed by other substitutes like per injection and cost Odensomab 60mg Lupin Ltd =₹19600/injection, Densurank 60mg Injection, RPG Life Sciences Ltd=₹23500 / & Denbri = ₹25845/, Abbott- Denaxa = ₹17000 and Denorange n of Biorange Biologicals Private Limited= ₹21000/injection Osteoblasts produce RANKL, a member of the tumour necrosis factor protein family. It is a soluble protein responsible for encouraging bone resorption by stimulating a signalling cascade in osteoclasts. Osteoclast development, activity, and survival are inhibited by denosumab’s high- affinity binding to RANKL. This interaction leads to enhanced cortical and trabecular bone mass and strength. Denosumab is administered by subcutaneous injection of 60 mg every six months in the upper arm, upper thigh, or abdomen [9], The cost for Denu (60 mg/ml), subcutaneous solution in prefilled syringe is around INR 7500. Each Denu dose consists of a single shot given subcutaneously every 6 months. With a half- life of approximately 26 days, it circulates in the bloodstream, binds to RANKL in the extracellular fluid, and is eliminated through the reticuloendothelial system [6], Denosumab does not reside in the skeleton and has a biological effect that lasts only if it is in systemic circulation, because of its distinct method of action in the extracellular environment. Multiple studies infer that denosumab is both effective & safe, exhibiting higher adherence rates and greater patient satisfaction.
Teriparatide (Forteo®)
Teriparatide is commonly known by the brand name Forteo®, is medicine used to treat osteoporosis due to use of prednisone, for several months, who cannot use other osteoporosis treatments. It is a synthetic form of parathyroid hormone (PTH) and stimulates the formation of new bone to increase bone mineral density. Forteo® 20 mcg is administered by injection once a day in the thigh or abdomen. As its long-term treatment effects are not known currently, therapy for more than two years is not recommended [11]. It is contra-indicated for persons with elevated calcium levels, pregnant or nursing women, or persons who have ever been diagnosed primary or secondary bone cancers.
A retrospective, multi-centre observational, study of 378 osteoporosis patients treated with 20 µg of subcutaneous TPTD daily for 6 months and monitored with DEXA scores of the hip joints both before and after TPTD treatment. The DEXA scores of the total population pre- and post- treatments were -2.75+0.58 and -2.15+0.95 respectively, with a statistically significant p-value of <0.001. In women the pre- and post-treatment scores were -2.728+0.52 and -2.276+0.49, with a significant p-value of <0.001. In males, the scores were -2.756+0.72 and -2.108+1.29 respectively, with a significant p-value of <0.05, thus confirming that 6-month treatment with TPTD significantly improved DEXA scores in osteoporosis [11].
Evenity (Romosozumab): is a member of the miscellaneous bone resorption inhibitors drug class. The cost for Event of 105 mg/1.17 mL subcutaneous solution in prefilled syringe is around $2,646 (INR 225,000) for a supply of 2.34 millilitres as each dose consists of 2 shots given subcutaneously per month for 12 monthly doses.
Evidence from the ARCH and FRAME trials suggests that use of Romosozumab followed by either alendronate or denosumab results in better outcomes (fewer fractures) compared to alendronate alone or placebo in patients with a prior fracture or at high risk of fracture. Patients had described “tolerable” or “inconsequential side effects such as joint, muscle, groin, or leg pain; soreness; achiness; and burning at the injection site following administration of Romosozumab. After completing 12 months of treatment, 1 out of 2 patients had increases in bone mineral density (BMD) in the hip and spine compared to other treatment options. The other patient on bisphosphonate and denosumab was intolerant to both [12].
Conclusion
Considering the surgical costs of fractured bones, limitation of the movement of the affected part for months and the fear of malunion and failure to revert to full movements, it makes sense to prevent, identify by screening menopausal women and men over 65 years every he recommendations are to get a central DEXA scan every two years for high risk, every 3 to 5 years for moderate risk, and every 10 to 15 years for low risk and treat osteoporosis, with available options [13].
Economic of Osteoporosis induced Fractures in India
Cost of Fixing Femur Fractures in India: A femoral neck fracture in elderly patients (> 65 years) is treated with an endoprosthesis with some cases, with a partial replacement. If the hip joint shows signs of osteoarthritis, a full replacement is taken up in India as the goal of treatment is to quickly stabilise the fracture and spare long periods of complete immobility. Depending on the location of the fracture, osteosynthesis of fixing the femoral neck with plates and screws or the femoral neck and a hip replacement is done. The distal femur is fixed with metal plates and screws or intramedullary nails. If the break involves the joint or is around a joint a total knee replacement is done with metal plates and screws placed through incisions on the side of the leg. Surgery usually takes 1 to 2 hours. The cost of such surgeries will be around 150,000-200,000 depending upon various other factors. Revision-free long-term survival was reported between 50-70% at 10 years, with the overall survival of the total femoral replacement (TFR) implant being around 80-90%.
Cost of Fixing Spinal Cord Fractures in India: Spinal fusion surgery is a procedure that involves fusing two vertebrae together to stop motion in a specific region of the spine. The surgeon may access the spine from the neck, behind the spine, on or off the vertebrae, or in the abdomen or throat. The surgeon may use a bone graft from the patient’s body, a bone bank, or the pelvis. For people with severely damaged vertebral discs, a synthetic implant to help restore vertebral height & movement is offered. The cost of spinal fusion surgery ranges from INR 2,50,000 to INR 5,00,000, depending on several factors like i) Surgical facility -location and accreditation, ii) Surgeon’s fees based on experience and known success rates, iii) The number of levels of fusion affects the cost iv) Depends on whether the surgery is open or minimally invasive, v) Diagnostic tests also affect the final cost vi) Pre & post-surgical expenses.
Forearm bone Fracture fixing: Our forearms have two bones the ulna on inner side, & the radius on outer side.
Both or either of them break and often bone ends are out of line or even be overlapping. If not interfered, the bones would heal, in incorrect position, leading to inability of turning hand from palm up to palm down. The best option is a surgery called internal fixation, to put the bone ends into their correct position and then fix them with steel plates & screws. It costs about INR 50,000-250,000 [14, 15, 16, 17, 18].
Conclusions
With an increasing aging population worldwide, an increase in the incidence of osteoporosis up to 30% of all postmenopausal women (PMW) and men over 60 years is reported. Almost 40% of PMWs and 15–30% of elderly men are sustaining one or more fragility fractures in their remaining lifetime.
A pooled prevalence of osteoporosis at the lumbar spine & femoral neck to the tune of 29% each and 6% at the hip region is a public health challenge. The prevalence of osteopenia at the lumbar spine and femoral neck is 37% each followed by the hip at 6%.
A statistically significant correlation between BMD & serum lipid levels in both pre & Post menopausal women is worth using it as an independent risk factor for osteoporosis.
Only a DEXA scan of the spine, hips and forearms is the way to diagnose Osteopenia and osteoporosis. Lower BMD scores are linked to higher fracture risk, especially in elderly. A T-score between -1 and -2.5 indicates osteopenia, a T-score of -2.5 or lower is osteoporosis. However, BMD alone does not determine fracture risk as overall strength play crucial role.
Osteopenia is a condition of low bone density, a risk factor for fractures, that is usually managed through lifestyle changes, exercise, and supplements.
Osteoporosis management begins with dietary measures like consuming low-fat dairy products, high- protein foods, vegetables, with tailored calcium & Vitamin D supplementation, with regular physical activity, weight- bearing & muscle-strengthening.
Aggressive treatment options include hormonal therapies like estrogenic therapy, Bisphosphonates to stabilize bones, and parathyroid hormone (PTH) and selective estrogenic receptor modulators (SERMs) in specific cases. Calcitonin is used primarily for pain relief, with limited effects on bone density improvement.
Advanced therapies include Ramucirumab, Denosumab and Teriparatide, administered as subcutaneous injections.
- Denosumab, given biannually, has been shown to increase spinal BMD by 9% and hip BMD by 4-5% over two years, significantly reducing fracture risks.
- Teriparatide Forteo®. a synthetic form of parathyroid hormone (PTH) is used for postmenopausal women at high risk of fractures & ineligible for other treatments.
- Romosozumab is the latest and costliest drug used for Osteoporosis, costing about 2 million INR (US$ 25,000) over a year for 12 monthly injections. Failure to treat osteoporosis may lead to fractures, the surgical management of which, is not only cost much more but also 100% success is not guaranteed. Limitation of the movement for the affected part due to malunion of the fractured ends is possible.
References
-
Florencio-Silva R, da Silva Sasso GR, Sasso-Cerri E, Simões MJ, Cerri PS (2015) Biology of bone tissue: structure, function, and factors that influence bone cells. Biomed Res Int 2015: 421746.
-
Bhadada SK, Chadha M, Sriram U, Pal R, Paul TV, (2021) The Indian Society for Bone and Mineral Research (ISBMR) position statement for the diagnosis & treatment of osteoporosis in adults. Archives of Osteoporosis 16: 102.
-
Shen Y, Huang X, Wu J, Lin X, Zhou X, et al. (2022) The Global Burden of osteoporosis, low bone mass, and its related fracture in 204 countries and territories, 1990- 2019. Front Endocrinol (Lausanne) 13: 882241.
-
Imran M, Singh A, Bhardwaj A, Agrawal D (2023) Prevalence of Osteoporosis & Associated Risk Factors among Postmenopausal Women: A Cross-Sectional Study from Northern India. Mohammad Imran, J Midlife Health 13(3): 206-212.
-
Aggarwal V, Muthukrishnan J, Manrai M, Chauhan P, Vasdev V, et al. (2021) The prevalence of osteoporosis & its association with serum testosterone & vitamin D in the elderly male population: A cross-sectional study. Med J Armed Forces India 79(2): 189-193.
-
Upadhyaya GK, Iyengar K, Jain VK, Vaishya R (2020) Challenges & strategies in management of osteoporosis & fragility fracture care during COVID-19 pandemic. J Orthop 21: 287-290.
-
Babhulkar S, Seth S (2021) Prevalence of osteoporosis in India: an observation of 31238 adults. International Journal of Research in Orthopaedics 7(2): 362-368.
-
Sinha A (2024) Osteoporosis and Bone Health: An Overview. MediNexus.
-
(2024) Men More Prone to Fractures from Falls. MediNexus.
-
(2023) Sun exposure for healthy vitamin D levels. Times of India.
-
Meena RK (2024) Dyslipidaemia – A Risk Factor for Osteoporosis in Women.
-
Saghafi H, Hossein-nezhad A, Rahmani M, Larijani B (2008) Relationship between lipid profile and bone turnover in pre and postmenopausal women. Iran J Public Health 37(2): 23-29.
-
Krishnan J, Santhanam S, Singh B, Patel S, Bhojwan DG, et al. (2024) Denosumab: A Useful Addition to the Armamentarium for the Management of Male Osteoporosis. Cureus 16(6): e62736.
-
Silverman S, Agodoa I, Kruse M, Parthan A, Orwoll E, et al. (2015) Denosumab for Elderly Men with Osteoporosis: A Cost-Effectiveness Analysis from the US Payer Perspective. J Osteoporosis 2015: 627631.
-
Anastasilakis AD, Toulis KA, Goulis DG, Polyzos SA, Delaroudis S, et al. (2009) Efficacy & safety of denosumab in postmenopausal women with osteopenia or osteoporosis: a systematic review and a meta- analysis. Horm Metab Res 41: 721-729.
-
Roy AN, Mazumdar I (2023) Effects of Teriparatide Treatment on Bone Mineral Density in Patients with Osteoporosis. Cureus 15(9): e45662.
-
(2022) Romosozumab (Evenity): CADTH Reimbursement Review. Canadian Agency for Drugs and Technologies in Health.
-
Periodicity of Bone Density Scanning. MedlinePlus.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results