The Menstrual Cycle
This study examines menstrual cycle characteristics and associated symptoms in 200 females aged 18 to 45 with regular menstrual cycles. Using a dedicated app, participants meticulously recorded menstrual syndromes over three months. Results show a mean cycle length of 28.5 days (SD = 2.3) and an average cessation duration of 5.2 days (SD = 1.1). Common symptoms include cramps (85%, severity = 6.2), mood swings (70%, severity = 5.8), and bloating (60%, severity = 4.5). Correlation analysis indicates a positive association between cycle length and cramp severity (r = 0.42, p < 0.01). However, no significant correlations are found between cycle length and mood swing (r = 0.12, p > 0.05) or bloating severity (r = 0.18, p > 0.05). This study provides nuanced insights into menstrual cycle variability, emphasizing the necessity of individualized symptom assessments for comprehensive reproductive health. The findings highlight the complexity of symptom manifestation and suggest that factors beyond cycle duration influence mood swing and bloating severity. This research lays the groundwork for future investigations into the multifaceted dynamics of menstrual health.
Introduction
The human female is a monotonous. The complex and well-controlled order of occurrences that exhibits a regular monthly period lies in guaranteeing that a singular oocyte is ovulated in some individual phases. Information designed to mislead or persuade an early fetus can arrest the process of endometrial peeling and guarantee its continuation. The monthly period is an apparent indicator of the miscellaneous levels of interplay between the hypothalamus, pituitary gland, ovary, and uterus. Interruption of this stem always leads to disordered periods. Gynecologists repeatedly search for and treat specific disorders. Therefore, a clear understanding of the management of the usual era is inevitable to guide realistic administration when things are miscalculated.
Although called the ‘period’ because menstruation is the apparent weekly occurrence all the while generative growth, the usual menstrual cycle is generally a reflection of ovarian occurrences. The election and tumor of the main follicle leads to increasing concentrations of hereditary estrogens, exciting endometrial development. Later, following the luteinizing birth control method (LH) surge, ovarian estrogens and progesterone from the entire luteum induce Endome-trial secretory changes, and the decline in luteal steroids results in a deficiency of gestation, leading to the beginning of the period. Hence, writing of dispassionate pertinence of the period requires devoting effort to something ovarian physics, while not disregarding events in the hypothalamus and pituitary and at the level of the uterus. The period was controlled at the endocrine and paracrine levels. Endocrinologically, skilled are the chaste response loops that harmonize the release of gonadotropin hormones from the pituitary with the ovarian steroids affecting the animate nerve organ arm. More recent studies have begun to elaborate on a complex succession of paracrine processes that operate inside the tissues of the ovary and uterus to establish a local organization.
Step 1: Ensuring Mon Ovulation Folliculogenesis and the ‘Follicular Phase’
In the beginning, human ovaries hold approximately 1,000,000 earliest follicles, jailed at the pro phase of the first meiotic separation. This number earlier reflects considerable regret from the maximum intensity of about 7,000,000 in the blood vessel ‘pool’ at 5 months of fetal existence [1]. Further exhaustion of the smallest living organism pool will persist during the whole of generative history, with the balanced escape of follicles from the earliest ‘situated chapter’ by re- effort into the formation of cells by dividing. The process of ‘escape’ from the situated state is not dependent on extra- ovarian influences: follicle exhaustion happens before and subsequently after menarche, all along the use of the spoken- contraceptive medicine and before birth and whether a suggestion of correction consistent period happens. Follicle adulthood will never evolve further in the pre-antral stage, traveling alternatively towards atresia. Of the original pool of 7,000,000 earliest follicles, only approximately 400 will always receive gonadotropin receptors and have a chance of ovulation. This exciting regret defines the female arm of natural selection, copied apiece immense ‘use without thought’ of spermatogenesis in the male at which point heaps of semen are produced each epoch all the while rich history accompanying only a teeny fraction ever fertilizing an oocyte.
Gonadotropins facilitate the inception of blood vessel incidents in humans. Studies utilizing transgenic animal varieties have begun to elucidate the contribution of regionally acting event-ovarian paracrine regulators of the earliest and smallest living organisms, including progress differentiation determinant 9 (GDF-9), antagonistic- Mullerian birth control method (AMH), and the Bax offspring of managers of apoptosis (Table 1 & Figure 1).
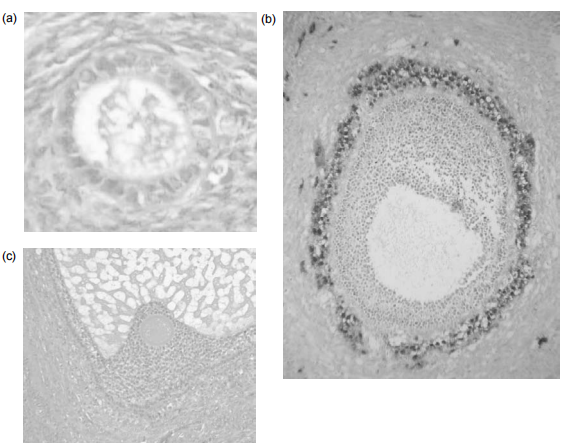
Figure 1: The development of a follicle, from (a) primordial, (b) small antral and (c) pre-ovulatory stages. (a) The primordial follicle is surrounded by a single layer of undifferentiated epithelial cells and is insensitive to gonadotropins. (b) The early antral follicle has well-differentiated theca (immunostained brown) and granulosa cell layers surrounding the developing antral cavity with the oocyte. (c) The pre-ovular follicle with the oocyte surrounded by the cumulus oophorus with well-differentiated granulosa and theca cell layers.
| Transgenic/Mutant Mouse | Ovarian Phenotype |
|---|---|
| C-kit Deficiency, Kit ligand Deficiency | Loss of germ cells (Migration/Proliferation Failure) |
| Zfx, Atm, Dazla knockout | Loss of germ cells (Proliferation Failure) |
| WT-1 knockout | Failure of Gonadal Development |
| GDF-9 Knockout | Folliculogenesis Arrest (Primary Stage) |
| IGF-1 Knockout | Folliculogenesis Arrest (Before Antral Follicle Stage) |
| Fsh-Bita Knockout | Folliculogenesis Arrest (Preantral Stage) |
| ER-Knockout | Failure to Ovulate |
| Wnt-4 Knockout | Reduced Germ Cell Number Masculinization |
Table 1: Specific Gene ‘Knockouts’ and their Effects on Ovarian Function in the Mouse.
Such studies are of additional hypothetical interest: understanding the mechanisms organizing rate of access into the pool of increasing follicles will help to disclose aforementioned ordinary clinical questions such as ‘basic’ premature ovarian defeat and early attack of midlife depression, as as well as suggesting the benefits of extending reproductive age [2].
Once an expanding blood vessel reaches the pre-antral stage of the incident, further progression to the antral and pre-ovulatory stages gives the impression that it is dependent on the demeanor of gonadotropins. The transitory elevation in the flowing aggregation of blood vessels stimulating the birth control method (FSH) visualized in the early follicular time of the ovarian phase allows a restricted number of pre-antral follicles to reach this stage of adulthood, establishing a ‘follower’ of practically synchronously expanding follicles. However, a singular ‘lead’ blood vessel will acquire significant aromatase catalyst exercise inside allure granulosa cells, chief to raised synth- friend, and discharge of estradiol from the androgenic precursor. The ‘two-container, two gonadotropins’ theory specifies the need for two together LH, to stimulate the result of forerunner androgens, specifically androstenedione, apiece theca cell tier, accompanying FSH forceful aromatization to oestradiol within abutting-granulosa container coatings [3]. FSH, LH, and human chorionic gonadotropin (HCG) are structurally similar, with an identical beginning subunit. Their specificity displays or exhibits fundamental public dissimilarities in the beta subunit (Figure 2). Hence, assays for these fragments use antibodies supervised against the tested-subunit epitopes.
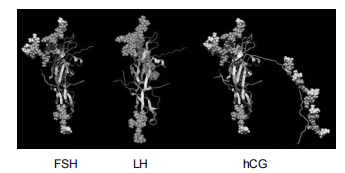
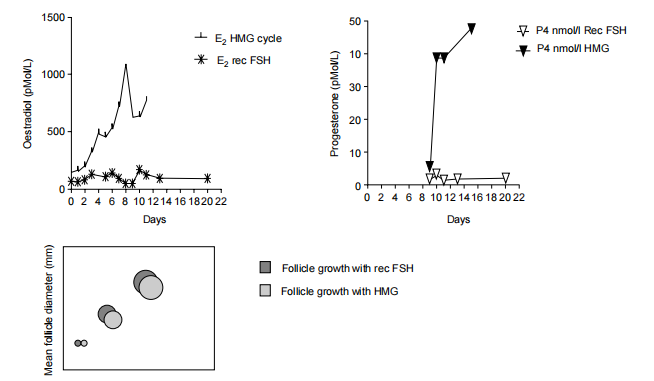
Figure 2: Molecular structure of FSH, LH and hCG. (Reproduced by kind permission of Dr Bernadette Mannaerts, Organon Ltd.) The essentiality of LH and FSH at this stage of the cycle is demonstrated when exogenic gonadotrophin substitutes are likely to be administered to subjects with Kallmann’s syndrome. These subjects are side-lined to emit gonadotropins into the distribution but have common ovarian physiology. The results of the study on a specific patient are shown in (Figure 3). The patient had Kallmann disease with anosmia, basic amenorrhea, and hypogonadal hypogonadism.
Ovulation initiation was performed by utilizing two different arrangements of gonadotropin. Treatment with FSH and LH in the form of human menopausal gonadotropins (HMG) induces both common blood vessel tumors, listened to by transvaginal ultrasound (bottom committee) and estradiol discharge (top left committee), superior to extreme luteal progesterone concentrations following in position or time an artificial LH surge accompanying hCG injection. This indicates that profitable ovulation and luteinization had occurred. In contrast, the situation accompanying FSH in the dearth of LH, using a recombinant FSH arrangement managed to equal little incident on ultrasound but little height in flowing estradiol concentration at the time of follicular progression and no increase in progesterone following in position or time hCG needle.
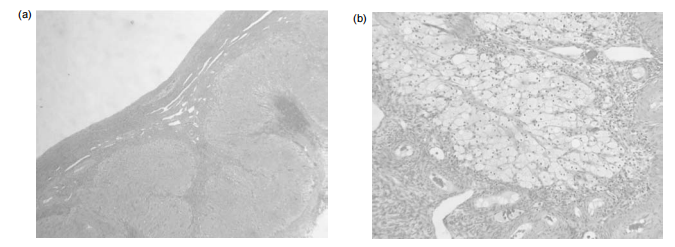
![Figure 4: Histological appearance of (a) late secretory and (b) menstrual endometrium (see p. 354). (Courtesy of Professor M Wells, University of Sheffield.) The pituitary secretes the gonadotropin hormones LH and FSH in response to pulses of gonadotropin release (GnRH) from the hypothalamus that travel to the beginning pituitary through the hypothalamo-hypophysial opening lot. LH secretion appears to be carefully contingent on GnRH pulsatility, while the discharge of FSH is co-regulated by hypothalamic GnRH and added determinants that act directly on the pituitary, possibly including inhibins and activins. At the usual follicular point, GnRH rhythm repetitiveness is approximately per 90-second brief period. GnRH pulses were less frequent in the luteal chapter, occurring approximately every 4 h. Disorders that slow GnRH pulsatility, in the same way, that eating disorders influence the loss of secretion of pituitary gonadotropins and a state of hypogonadal hypogonadism accompanying imperceptible antitoxin LH and FSH and amenorrhea, Once the aggregation of serum estradiol starts to rise in the intervening follicular step, hasty suppression of pituitary FSH results in a negative response. Recent studies have suggested that suppression of pituitary FSH discharge in the follicular phase may be co-intervened by increasing antitoxin concentrations of inhibin B, a glycoprotein hidden by the granulosa containers of the cultivating organism’s smallest living organism. It is not surprising that a two-fold device to control follicular- time FSH discharge has evolved [4]. The decrease in the flowing aggregation of FSH withdraws gonadotropin ‘drive’ from the balance of the increasing cohort of follicles. The result is progression to atresia for almost the smallest living organism, leading to mono-ovulation.](/fulltextimages/11847/fig_4.png)
Figure 4: Histological appearance of (a) late secretory and (b) menstrual endometrium (see p. 354). (Courtesy of Professor M Wells, University of Sheffield.) The pituitary secretes the gonadotropin hormones LH and FSH in response to pulses of gonadotropin release (GnRH) from the hypothalamus that travel to the beginning pituitary through the hypothalamo-hypophysial opening lot. LH secretion appears to be carefully contingent on GnRH pulsatility, while the discharge of FSH is co-regulated by hypothalamic GnRH and added determinants that act directly on the pituitary, possibly including inhibins and activins. At the usual follicular point, GnRH rhythm repetitiveness is approximately per 90-second brief period. GnRH pulses were less frequent in the luteal chapter, occurring approximately every 4 h. Disorders that slow GnRH pulsatility, in the same way, that eating disorders influence the loss of secretion of pituitary gonadotropins and a state of hypogonadal hypogonadism accompanying imperceptible antitoxin LH and FSH and amenorrhea, Once the aggregation of serum estradiol starts to rise in the intervening follicular step, hasty suppression of pituitary FSH results in a negative response. Recent studies have suggested that suppression of pituitary FSH discharge in the follicular phase may be co-intervened by increasing antitoxin concentrations of inhibin B, a glycoprotein hidden by the granulosa containers of the cultivating organism’s smallest living organism. It is not surprising that a two-fold device to control follicular- time FSH discharge has evolved [4]. The decrease in the flowing aggregation of FSH withdraws gonadotropin ‘drive’ from the balance of the increasing cohort of follicles. The result is progression to atresia for almost the smallest living organism, leading to mono-ovulation.
The machine by which this option of a sole main follicle occurs has existed since the ‘thresh-traditional’ idea, at which point the climbing aggregation of FSH exceeds the beginning and opens a ‘bow, admitting one blood vessel in the second- place tumor and expansion. Suppression of FSH aggregation then closes the bow, preventing the progress of diversified mature follicles (Figure 5).
The threshold idea is beneficial for understanding the traps of ‘super ovulation’,’ at which point regular injections of high doses of FSH are likely to be part of an artificial pollination (IVF) situation. The aim was to support a follower of eight or more follicles suitable for ultrasound-guided oocyte retrieval. However, if the blood vessel pool is narrow (for instance, if the patient is near the end of the menstrual cycle), the yield of mature follicles will be unsatisfactory, whereas if the smallest living organism pool is large (e.g. if the patient has polycystic ovary disease), there is a risk of over-response accompanying the energetic-provocation condition.
![Figure 5: The ‘threshold concept’ illustrating dependence of advanced follicle growth and maturation on a rise in circulating FSH concentration above an arbitrary threshold, with subsequent suppression of FSH preventing multiple follicle development. (Reproduced with kind permission from ‘Archives of Medical Research’)[5].](/fulltextimages/11847/fig_5.png)
Step 2: Ensuring Maintenance for Very Early Pregnancy the LH Surge and Ovulation
The final development of oocytes occurs only after the start of the LH surge. This guarantees that oocytes are mature and ready for fertilization when they are freed from blood vessels. The LH surge showed a matched discharge of LH from the gonadotrophic containers of the prior pituitary gland. This occurs in response to the expeditious rise in estradiol levels during the concluding days of the follicular state of the ovarian phase. Pulses of GnRH from the hypothalamus increase in importance and frequency, causing the LH surge to accompany an expeditious outflow of LH and, in an inferior range, FSH from the pituitary.
The LH surge is attributed to an increase in antitoxin aggregation of progesterone. The gift concerning this rise to the fairy-ovulatory phase of the era is unsure but stops the pre- ovular rise in antitoxin progesterone aggregation utilizing the progesterone receptor adversary oral contraceptive pill bars efficlient ovulation. Compounds accompanying belongings analogous to oral contraceptive pills are being proven as attainable contraceptive powers, perhaps acting together by preventing ovulation and information that is designed to mislead or persuade.
The LH surge introduces final development of the oocytes, accompanied by the formation of cells by dividing and banishing of the first opposite crowd, which holds one of two haploid sets of chromosomes from the oocyte. The LH surge still induces an inflammatory backlash situated above the blood vessel adjininsignificant value to the exposed surface of the ovarian rind. A process of new elements bowl establishment, accompanying mixed release of Prostaglandins (PGs) and cytokines lead to rupture of the blood vessel obstruction and ovulation about 38 hours after the introduction of the LH surge. The chemotactic effect of ovarian cytokines draws the fimbria of the Fallopian hose to proximity to the smallest living organism. A thin-gelled waste rope appears to touch the opening of the Fallopian hose to the ovular blood vessel, making a bridge for the transportation of the oocyte into a television set.
The ‘empty’ blood vessel expeditiously fills accompanying ancestry and the theca and granulosa container coatings of the smallest living organism obstruct luteinization, accompanied by the composition of luteum (Figure 6). A fast combination of progesterone and estradiol was observed. Concentrations of progesterone in antitoxin rise to above 25 nmol/l in individuals undergoing extreme treatment of psychotic states, with electrical shock concentrations visualized for some birth control methods in the circulation.
These concentrations increased in addition to those observed in gestational trials
Endometrial Development during the Menstrual Cycle and Early Pregnancy
Progression through the follicular phase of the cycle is characterized by the appearance of increasing amounts of estradiol in circulation. This acts on the basal layer of the endometrium, which persists from cycle to cycle, in contrast to the monthly shedding of more superficial layers of the endometrium. The new proliferative endometrium grows rapidly under the influence of estradiol, in synchrony with the growth and maturation of the oocyte endometrial glands and stromal compartments, in preparation for the occurrence of secretory endometrium lenient of principle following the LH surge, luteinization of the ruptured blood vessel, and composition of the corpus luteum, accompanied by the discharge of large amounts of progesterone.
A vital element in tumors of the athletic endometrium is the composition of new vessels (endometrial angiogenesis), which appears to occur by extension and grow from pre- existing narrow containers in the basal area. Endome- trial angiogenesis may be divided into three stages: first, throughout the period to correct the vascular bed; second, the proliferative point to expand the Endome-trial vascular supply; and third, finally accompanying spiral arteriole development and coiling to provide an adequate vascularized section for impregnation of the ovum (Figure 7) [6].

Figure 7: The histological appearances of the endometrial cycle, showing proliferative, early secretory, mid-secretory phase’s equivalent to the images a, b and c. (Kindly provided by Professor M Wells, University of Sheffield.) Therefore, in contrast to most vascular beds, which maintain a determined structure throughout their existence, the endometrial vascular network evolves and regresses during each brother-stroll era. Numerous angiogenic and angiostatic factors have been identified in the human endometrium. Most some of these studies have focused on vascular endothelial progress determinants (VEGF) and interleukins that grant permission to be straightforwardly compassionate to varying concentrations of ovarian steroids.
The growth of a healthy secretory endometrium is essential for the principal and profitable incidence of gestation. In humans, the oocyte is fertilized in the ampullary portion of the fallopian tube and travels to the uterus, eventually reaching stage 3 at the morula stage of development. The blastocyst, with its specific trophectoderm and central bulk container, eventually forms 4. The blastocyst sheds the zona pellucida and stands by the endometrial epithelium, which is the origin of the process of information that is designed to mislead or persuade. Implantation is the first step in the interplay between the containers of the blastocyst and endometrium, that is to say, ‘tween the mom and the unborn young. Hence, this interplay is fault-finding for successful gestation, and endometrial proteins have been identified as potential regulators of blastocyst growth and opinion. They contain endome-trial integrins, glycosylated container stickiness fragment 1 (GlyCAM-1), and osteopontin [7]. Continuous exposure of the endometrium to progesterone in early gestation downregulates progesterone receptors in the epithelium, a process that guides the deficiency of the container-surface mucin MUC1 and the initiation of hidden attachment proteins. ‘Rescue’ of the bulk luteum by hCG secreted from the trophoblast of the expanding gestation is essential for allure duration.
Interruption of the progesterone combination and discharge of the entire luteum, for example, utilizing the supporting progesterone receptor for the oral contraceptive pill, is secondhand in dispassionate practice to encourage the end of early pregnancy. In contrast, ‘luteal state support, ’ in the form of an hCG needle or introduced vaginal progestin, is used to support IVF pregnancies because usual luteinization is stopped by one GnRH agonist drug used to bar rash LH surges and undesirable ovulation.
Menstruation
Menstruation refers to the peeling of the excellent social tiers of the endometrium, with the expected regrowth from the basal layer afterward. Menstruation begins by obeying the rules of flowing concentration of progesterone that understand luteal regression—a decline of ‘rescue’ of the bulk luteum by an inserted early gestation. Luteal progesterone synthesis is absent in LH from the pituitary gland. During luteolysis, progesterone discharge falls regardless of the upholding antitoxin concentrations of LH because the body of the luteum is less sensitive to gonadotrophic support and is progressively unfit to assert the production of progesterone. In contrast, in the birth era, the growing block to progesterone combination overcomes the promptly growing concentrations of hCG that act in the bulk luteum through all LH receptors.
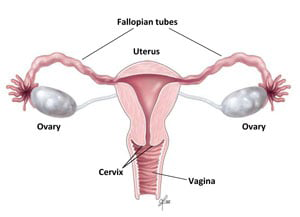
Female Reproductive Organs
In the next premenstrual phase, progesterone retraction activates a complex succession of intrauterine signals that contain chemotactic determinants that draw leukocytes into the uterus, mold metallo proteinase (MMP) enzymes, PGs, and different compounds that act on the uterine vessels and smooth influence. The ‘encroachment’ of leukocytes and after verbalization of inflammatory mediators has surpassed to menstrual- action being likened to an inflammatory occurrence [8, 9]. The PGs of the E and F succession are present in extreme concentrations in the endometrium and their combination is contingent on the ovarian steroids. Increased results un productiveness of PGF2∞ supporting- duces the myometrial shortenings and vasoconstriction visualized at period, while E-order PGs increase pain and edema and are vasodilatory. PGE2 still performs to encourage a combination of the cytokine IL-8 (interleukin-8), another key inflammatory and chemotactic judge [10]. Pronounced vasoconstriction in proper sequence leads to local fabric hypoxia, further augmenting the release of inflammatory mediators. The result concerning this cascade of events is blockage of the spiral arterioles accompanying shortening of the uterine power, chief to the banishing of the discarded fabric (Figure 4).
These studies have clear relevance to the dispassionate study of menorrhagia and different menstrual disorders. Inhibitors of PG combining are established in these conditions, with good scientific footing. However, PG combining is more a main component of ovulation, and the use of strong inhibitors of PG combination, to a degree non- steroidal antagonistic-inflammatory powers, can bring about anovulatory cycles and automatic un productiveness.
Research Method
Participants: The study included 200 females aged 18 to 45 with regular menstrual cycles. Participants were recruited based on self-reported menstrual regularity.
Procedure: Over three months, participants documented menstrual syndromes and utilized a dedicated app for cycle tracking. Data collected included cycle length, cessation characteristics, and the intensity of common symptoms.
Data Analysis: Descriptive statistics, including means and standard deviations, were calculated for cycle characteristics and symptom severity. A correlation analysis explored connections between cycle length and symptom intensity.
Results
Cycle Characteristics: The mean cycle length was 28.5 days (SD = 2.3), and the average cessation duration was 5.2 days (SD = 1.1).
Symptom Severity: Cramps were reported by 85% of participants, with an average severity of 6.2. Mood swings were reported by 70%, with an average severity of 5.8. Bloating was reported by 60%, with an average severity of 4.5.
Correlations: A positive correlation was found between cycle length and cramp severity (r = 0.42, p < 0.01). No significant correlations were observed between cycle length and mood swing (r = 0.12, p > 0.05) or bloating severity (r = 0.18, p > 0.05).
Discussion
The results offer valuable insights into menstrual cycle variations and symptom severity. The observed mean cycle length aligns with existing literature, emphasizing the normalcy of the sample. The positive correlation between cycle length and cramp severity supports previous research linking hormonal fluctuations to symptom intensity. However, the lack of significant correlations with mood swing and bloating suggests multifactorial influences beyond cycle duration. This warrants further investigation into individual variations and external determinants, such as lifestyle and contraceptive use.
Limitations
While this study provides valuable insights, limitations include potential recall bias in the data collection process and the non-representative nature of the survey sample. The intricacies of menstrual health warrant further investigation, necessitating future research beyond the scope of this study.
Conclusion
In conclusion, this study advances our understanding of menstrual cycles and associated symptoms. The findings highlight the complexity of symptom manifestation and underscore the need for personalized assessments. While providing valuable baseline data, the study suggests avenues for future research into the intricate interplay of hormonal, psychological, and lifestyle factors influencing menstrual health. These insights contribute to the ongoing dialogue in reproductive health, emphasizing the importance of tailored approaches for comprehensive care.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project we also thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout this study. Their insights and expertise were instrumental in shaping the direction of this project Declaration of Interest I at this moment declare that: I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management.
References
-
Baker TG (1963) A Quantitative and Cytological Study of Germ Cells in Human Ovaries. Proc R Soc Lond B Biol Sci 158: 417-433.
-
Block E (1951) Quantitative Semantic Analyses of the Follicular Whole in Girls. Acta Endocrinol 8: 33.
-
Baird DT (1987) A Model for Follicular Selection and Ovulation: Lessons from Superovulation. J Steroid Biochem 27(1-3): 15-23.
-
Groome NP, Illingworth PJ, Brien M, Pai R, Rodger EF, et al. (1996) Measurement of Dimeric Inhibin B Throughout the Human Menstrual Cycle. J Clin Endocrinol Metab 81(4): 1401-1405.
-
Macklon NS, Fauser BCJM (2001) Follicle-exciting Birth Control Method and Leading the Smallest Living Organism’s Growth in Humans. Arch Med Res 32: 595- 600.
-
Rogers PAW, Gargett CE (1998) Endometrial Angiogenesis. Angiogenesis 2: 287-294.
-
Lessey BA (2002) Adhesion Fragments and Impregnation of the Ovum. J Reprod Immunol 55: 101-112.
-
Kelly RW (1994) Pregnancy Sustenance and Childbirth: The Act of Prostaglandin in Maneuvering the Invulnerable and Angering Answer. Endocr Rev 15: 684-706.
-
Kelly RW, King AE, Critchley HO (2001) Cytokine Control in Human Endometrium. Reproduction 121(1): 3-19.
-
Sales KJ, Jabbour HN (2003) Cyclooxygenase Enzymes and Prostaglandins in Pathology of the Endometrium. Reproduction 126(5): 559-567.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City