Marginal Adaptation, Fracture Resistance and Failure Patterns of Two CAD/CAM Overlays
Statement of problem Coronal rehabilitation of endodontically treated posterior teeth is still a controversial issue. Purpose: The purpose of this study was to investigate marginal adaptation, fracture resistance and failure patterns of two CAD / CAM overlays compared to direct fiber post reinforced composite (FPR composite). Materials and methods: Fifty maxillary premolars received endodontic treatment and cavity prepared for overlay were used and randomly distributed into 5groups and restored as following: Zirconia overlay (Katana Zirconia HT), Resin Nano Ceramic overlay (Lava Ultimate) , Glass fiber post and composite (Filtek Z250), Direct composite resin (Filtek Z250). While unrestored specimens served as a negative control. Vertical marginal gap was examined under the stereomicroscope. Fracture resistance test was carried out using a universal testing machine, and presence of micro-cracks was detected using a stereomicroscope. The fracture mode of the specimen was identified using scanning electron microscopy: (n=10, α=0.05). Results: Statistical analysis of marginal gaps revealed significant statistical differences as CAD/CAM overlays had higher vertical marginal gap, Katana zirconia (118±39.9), Lava ultimate (107.4±28.9), compared to FPR composite (73.5±21.14) and direct composite (66.6±31) (F=13.1, p =0.022).There was a statistically significant difference (F= 42.9, p<0.001) between fracture resistance of Katana zirconia overlays and all comparing groups, and Katana zirconia overlays did not showed any fracture. Conclusion: CAD/CAM overlays (zirconia and lava ultimate) showed a significantly higher marginal discrepancy than FPR composite and direct composite resin. Fracture resistance of Zirconium overlays was significantly higher than Resin Nano Ceramic and FPR composite which used for restoration of endodontic treated teeth. Clinical Implications: Zirconium overlays, Resin Nano Ceramic overlay are conservative treatment option that could be used to restore damaged endodontic treated teeth in comparison to the full crown restoration.
Introduction
Restoration of endodontically treated teeth is a common problem in restorative dentistry, related to high incidence of fractures occurring in such teeth [1]. Endodontically treated teeth are affected by a higher risk of biomechanical failure than vital teeth [2]. Successful endodontic treatment largely depends on selection of an appropriate restoration that is concerned with efforts to save the tooth structure and the restorative materials used [1, 3]. The preferred final restoration for endodontically treated posterior teeth remains contentious. The conventional means of restoring endodontically treated teeth is a build-up with a post and core, which utilizes adhesive procedures and placement of a full coverage crown with a sufficient ferrule [4]. Traditionally, full coverage cast restorations have been used, even though adhesively placed restorations with total cuspal coverage (overlays) have been proposed as a more conservative alternative. The significant advantage of adhesive restorations is their ability to mimic the natural behavior of enamel and dentin (biomimetic principle) and simultaneously reduce the need for intracanal preparation and unreasonable destruction of remaining tooth substance [5]. In the 1990s, fiber-reinforced composites (FRC) were introduced as post material. The placement of an endodontic post creates an unnatural restored structure since it fills the root canal space with a material that has a defined stiffness unlike the pulp. Hence it is not possible to recreate the original stress distribution of the tooth. Steel posts are the most dangerous for the root, potentially leading to its fracture. Even working on the cement layer stress adsorbing effect by using less rigid cements, it is not possible to improve the stress arising in the system because of the high rigidity of the steel post [6]. Recently, the use of glass fiber posts results in the best stress distribution, since the cement layer rigidity is less relevant compared to steel and carbon post configurations [7]. Posts have often been described as not to reinforce endodontically treated teeth [6]. Moreover, some authors noticed that posts may interfere with the mechanical resistance of teeth, increasing the risk of damage to residual tooth structure [8]. Their role of maintaining the core material is particularly relevant for posterior teeth, where masticatory loads are essentially compressive. Increased demand in recent years for esthetic and metal-free restorations has led to the development of a computer design/manufacturing (CAD/CAM) system for fabricating ceramic inlays, onlays, and veneers. CAD/CAM system generated ceramics are currently available, which provide a novel means of restoring large cavities in posterior teeth and achieving chair-side design and automated production of all-ceramic monolithic single- unit restorations [9, 10]. All-ceramic crown restorations have become an alternative to metal crowns for tooth reconstruction. Recently the introduction of endocrown comprises a circumferential butt margin and a central retention cavity inside the pulp chamber and constructs both the crown and core as a single unit. This approach utilizes the surface available in the pulp chamber to ensure the stability and retention of a restoration through adhesive bonding. However, the biomechanical mechanisms involving CAD/CAM ceramic inlay/onlay, endocrown and classic crown restoration affects the stress transfer in restored teeth are still unclear [11]. Lava ultimate restorative system eliminates many of the drawbacks associated with traditional dental ceramics by combining resin and nano-technologies. Nano ceramic particles are embedded in a highly cross-linked resin matrix (80% wt Nano ceramic and 20% wt resin).It can be more efficient to produce because the firing step is eliminated; cementation and adhesive application procedures are simple. Lava ultimate resin nano ceramic with low modulus of elasticity lower than brittle glass ceramic materials and porcelain fused to metal veneering porcelain that allowed absorption of chewing forces and decrease stresses falling on restoration, this is especially advantageous for crowns over implant [12]. The aim of this study was to investigate, fracture resistance, failure pattern and marginal adaptation of two CAD /CAM overlays. The proposed null hypothesis was that the marginal adaptation, fracture resistance and failure pattern of endodontically treated teeth is not influenced by the use of a fiber post reinforced composite nor by the type of overlay restoration.
Materials and Methods
Preparation of the specimens
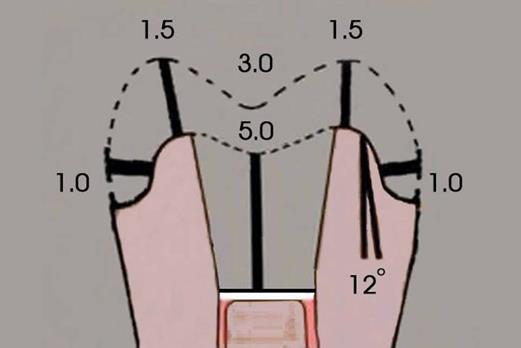
Fifty human maxillary premolars free from caries or previous restorations were selected. They were cleaned of external debris, examined for cracks, and stored at 37°C at (90%) relative humidity before mechanical testing. An x-ray image was taken for each tooth and the pulp chamber was accessed following standardized endodontic procedures (oval on the occlusal surface and should be in the middle third of the tooth, both mesiodistally and buccolingually). Each set of rotary files (ProTaper, Dentsply-Maillefer, Ballaigues, Switzerland) was discarded after four root canal preparations or if it demonstrated a visible deformation. Root canals were regularly irrigated between instrumentation with 2 ml of (5.25%) sodium hypochlorite. All root canal space was obturated using the lateral condensation technique, using calibrated gutta-percha points (F2, Dentsply-Maillefer, Ballaigues, Switzerland) and an endodontic sealer (ADSEAL- META-BIOMED CO.LTD). All endodontically treated teeth were individually mounted in a prefabricated copper cylinder vertically in self-curing acrylic resin blocks (Acrostone) to a depth of 2 mm apical to the cement enamel junction (CEJ) simulating the natural biological width. Before preparation of teeth, a silicone mold was made with normal setting vinyl polysiloxane impression material (Elite HD+ Putty, Zermack, Italy) for the coronal portion of each tooth. These pre-preparation silicon molds were used -later on- as reference guides to assist in reproducing coronal size and morphology during overlays fabrication, and also to standardize dimensions between different fabricated overlays. Mesio-occulso-distal cavities were prepared for the endodontically treated premolars by coarse diamond coated stone 845, DIA. TESSIN, Switzland) using a highspeed hand piece that was placed in a surveyor under water-cooling. The standardized dimensions of the tapered preparation were 3mm in buccolingual width and 3.5 mm in depth at the occlusal isthmus, the depth of the access cavity was 5 mm from the buccal cusp tip till sub pulpal wall, gingival wall was at the junction between the middle and cervical third, all walls had12° divergence toward the occlusal plane. A 1.5 mm occlusal reduction was performed on the buccal and palatal cusps resulting in horizontal flattening of the cusps. A 1mm wide shoulder finish line was then prepared on the entire periphery the junction between the middle and cervical third (Figure 1).
Restoration of the specimens
Group 1, 2: Two types of CAD/CAM blocks were used (Zirconia, Katana Zirconia HT, Kuraray Noritake Dental Supply Co. Ltd., Miyoshi, Aichi, Japan) and Resin Nano Ceramic (Lava Ultimate, 3M ESPE, MI, USA). The specimens were three dimensionally scanned using optical scanner (smart optic-activity 102-Germany) after being dusted by fine powder spray (Hinriscan-spray- Germany) and designed using design tool software (dent Create! Design software) and milled using the CAD/CAM five axis dry milling machine (Roland DWX-50-Japan). Cementation: The inner surface of the Zirconia ceramic overlays was pre-treated with Al2O3 abrasive particles, while Resin Nano Ceramic overlays were coated with primer Scotch bond Universal adhesive mixed with the Scotchbond Universal DCA Dual Cure Activator, 3M ESPE, MI, USA). The restorations were cemented with Rely X U200 self –etch dual resin cement, 3M ESPE, MI, USA) according to the manufacturer’s instructions under fixed pressure 300 g. After light Polymerization for 2 seconds, while the cement was in the gel state, excess cement was removed with an explorer and then polymerization was performed by the application of a LED light Blue phase, Ivoclar Vivadent ) in each tooth face with an intensity of 1200 mW/cm². Group 3: Received a glass fiber post reinforced composite restoration. Root canal filling material was removed from the root using a special reamer for Glassix posts to a depth of 7 mm while keeping at least 4 mm of root filling intact to preserve the apical seal. The post-space was prepared with calibrated drills. Tapered glass fiber- reinforced composite post Glassix post, HaraldNordin SA, Chailly/Montreux, Switzland )was cut to the required length using a diamond stone, ensuring at least 2 mm emergence outside the root canal orifice, the posts were then luted using a resin cement (Rely X U200) using elongation tips and following manufacturer’s instructions. Excess cement was removed using a micro-brush, which was activated with a LED light for 40 seconds with the tip of the unit directly in contact with the post. For the resin composite restorations, a self-etching light- polymerized adhesive resin (Scotch bond Universal adhesive) was applied, after which it was air-thinned and light polymerized according to manufacturer’s instructions. Resin composite (Filtek Z350 XT Flowable Restorative, 3M ESPE, MI, USA) was placed around the post and light polymerized, followed by a 2 mm incremental build-up technique using composite resin (Filtek Z250). A template was used to ensure obtaining identical shape of the overlay.
Group 4: Was restored using direct resin composite (Filtek Z 250). Group 5: Was not restored and served as negative control group. The marginal adaptation was evaluated by measuring the vertical gap between the edge of the overlay and the prepared tooth finish line using stereomicroscope [13] olympus sz100, Japan equipped with cannon E-330 camera, Japan) and image processing software, Cell^A- olympus, Japan). Four landmarks (mesial, distal, buccal, and palatal) were defined. The fractured resistance: Each specimen was inserted into the holding device and a controlled load was applied at the center of the restoration using a stainless steel sphere with a 4mm round tip-diameter in a direction parallel to the longitudinal axis of the restored teeth using a universal loading machine, Comten Industries, Inc., St. Petersburg, Florida, USA) at a crosshead speed of 1 mm/minute. All specimens were loaded until fracture and the maximum breaking loads were recorded in Newton’s (N). The failure pattern was visually evaluated and classified as restorable or un-restorable or catastrophic fracture. Restorable specimens were inspected for the presence of micro-cracks using a stereomicroscope at different magnifications. The fracture origin of the specimen was identified using SEM, JEOL JSM -5300 Scanning Microscope, Japan). Two-way analysis of variance (ANOVA) and Bonferroni post hoc tests (a = 0.05) were used to analyze the data (SPSS 12.0, SPSS Inc., Chicago, IL).
| Katana | Lava | FPR | Direct | Un | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | P | ||||||||||||||||||||||
| zirconia | ultimate | composite | composite | restored | |||||||||||||||||||
| Marginal adaptation (um) | 118±39.9 | 107.4±28.9 | 73.5±21.14 | 66.6±31 | ------- | 13.1 | 0.022* | ||||||||||||||||
| Fracture resistance (N) | 5000±0 | 1320.6±379.7 | 1259±535.76 | 597.9±137.66 | 262.4±170 | 42.9 | 0.001* | ||||||||||||||||
| Fracture mode | 3±0 | 1.8±0.79 | 1.6±0.84 | 1.9±0.31 | 1±0 | 18.4 | 0.001* |
Results
Statistical analysis of marginal gaps revealed a significant statistical differences as CAD/CAM overlays had higher vertical marginal gap: Katana zirconia (118±39.9) Lava ultimate (107.4±28.9) compared to FPR composite (73.5±21.14) and direct composite (66.6±31) (F=13.1, p=0.022). Regarding the Fracture resistance test, the highest force, which can be applied by the universal testing machine, was 5000 Newton. However all Katana zirconia overlays did not fracture. There was also a statistically significant difference (F=42.9, p<0.001) between the mean values of Katana zirconia overlays and all comparing groups. Unrestored specimens were significantly weaker (262.4 Newton). There were statistically significant differences in the mode of failure (F=18.4, P≤ 0.001) between Katana zirconia overlays and all comparing groups, and did not show any catastrophic fracture or un-restorable fracture. There were no statistically significant differences (p=1) between Lava ultimate overlays and both FPR composite and Positive control groups. Also, there were statistically significant differences (p≤ 0.001) between negative control group (un-restored) and all comparing groups and did not show any restorable fracture and showed (70%) catastrophic fracture (Figures 2-4).

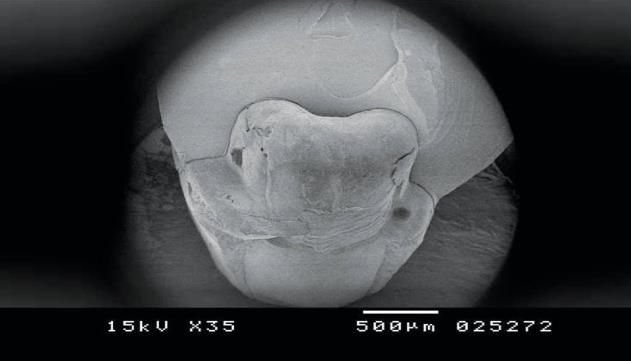
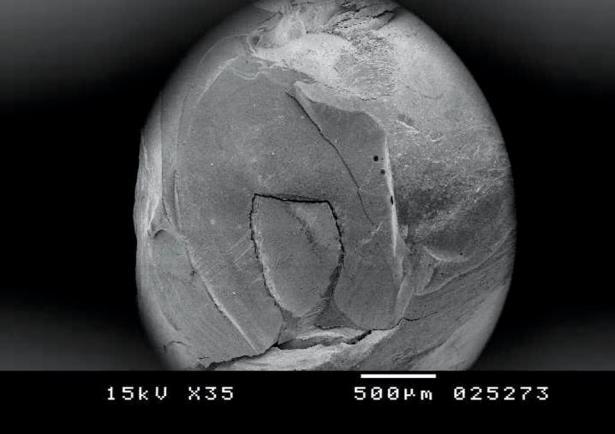
Figure3: SEM image x 35 demonstrating restorable fracture (lava ultimate).
Discussion
Considering the results obtained in this study, the null hypothesis has to be rejected as CAD/CAM overlays showed a significantly higher marginal discrepancy than FPR composite and direct composite .On the other hand, Zirconia overlays showed increase fracture resistance of endodontically treated premolars to a significantly higher level than Resin Nano Ceramic and FPR composite. According to Hickel [14] gaps that deviate from ideal but could be adjusted to ideal by polishing are between 50 and 150 microns; gaps with leakage and discoloration limited to the borders of the restorations are easily perceptible with explorers and are not considered to have a long-term negative impact if they are between 150 and 250; gaps larger than 250 microns should be replaced to prevent secondary caries or large fractures at the margins. All tested groups demonstrated clinically acceptable marginal discrepancies in vitro below 120μ.
zirconia overlays revealed a statistically significant increase vertical marginal gap than FPR composite. Beuer, et al. [15] reported that besides the sintering process; scanning procedure, the processing of the geometric data collected, the calculation of milling parameters, and the actual milling process are factors that affect the fitting accuracy of zirconia restorations. The quality of the 3-D image of a tooth preparation is responsible for the marginal adaptation of the final machined restoration [16]. So the additional steps of scanning and software limitations could partially explain the larger marginal and internal gap found in the CAD/CAM group compared to direct FPR composite overlays. The mean value of vertical marginal gap of direct FPR composite overlays of other surfaces was significantly lower than both CAD CAM overlays. Although CAD/CAM systems have the potential to enhance accuracy by omitting several conventional fabrication methods, they have introduced some additional steps to the fabrication process that may result in inaccuracies, namely scanning, software design, milling and material processing [17]. Reich, et al. [18] also reported that systems; which depend on optical impression, experience problems with rounded edges and positive error (which simulates virtual peaks near the edges, so-called over- shooters). The rounded edges and over-shooters phenomena have been described for the Cerec intraoral camera [19] but they apply to all CAD/CAM systems that acquire their optical impression by means of striation projection such as the scanner (smart optic-activity 102- Germany) used in current study. Since there is no elevation of the tooth geometry in reality, an increase of discrepancy may result. Also the scan spray that used to inhibit the reflection during scanning could somehow increase the internal gap, as it makes a fine layer on the specimen margin. Resin Nano- Ceramic restorations recorded better marginal fit than Zirconium Dioxide, these results are in agreement with the findings of Hamdy A [20] (this might have been a result of differences in composition, Lava ultimate bloc is a millable composite resin formed of (80% nano-ceramic zirconia and silica nano particles, (20%) composite resin). Direct FPR composite overlays recorded better marginal adaptation than CAD CAM indirect overlays .The rigidity of dental restorative materials is considered to be a very important issue when evaluating the adhesive tooth restoration interface. Composite materials are more resilient than zirconia overlays. In a study of posterior teeth, Krejci and others [21] showed an excellent marginal adaptation for adhesive composite restorations. Higher vertical marginal gap of zirconia overlays did not support the results reported by some authors Gonzalo E, et al. [22, 23] although it is difficult to compare the results between these studies, but there is a similarity due to the CAD/CAM systems used in these studies. Almost all of these studies used Procera (Procera; Noble Biocare, Goteburg, Sweden) systems to fabricate either titanium or zirconium crowns or copings. It has been demonstrated that adaptation primarily depended on the type of the computer-aided manufacturing (CAM) system [24]. There are some differences between digitization systems and CAM techniques used by these two systems. Both systems use mechanical scanner to detect and record a surface [16]. Previous studies have demonstrated more precision in mechanical digitalizing than optical scanning [16, 22, 23, 24, 25]. As reported by Martiez-Rus, et al. [26] fewer laboratory steps and the precision of both the digitizing method and the industrial fabrication process for the Procera system resulted in better marginal fit comparing to other systems that had evaluated in the study. Regarding to fracture resistance, all Katana zirconia overlays did not fracture even at the highest force, which can be applied by the universal testing machine, was 5000 N. This result is consistent with a previous report wherein Beuer, et al. [27] demonstrated that 11 out of 12 monolithic zirconia crowns did not fail at 10.5 kN. Also Keisuke Nakamura [28] demonstrated that some of the monolithic zirconia crowns with occlusal thickness of 1.5 mm were not fractured even at 10 kN. The latter result is also in agreement with a study conducted by Hamdy A [20] in which comparison fracture resistance of Zirconium Dioxide and Resin Nano Ceramic CAD-CAM restorations (Lava Ultimate Restorative), Zirconium Dioxide showed a higher resistance to fracture than Resin Nano Ceramic restorations, this is attributed to the very high modulus of elasticity of Zirconium Dioxide due to densely sintered yttria-tetragonal zirconia polycrystal (y- TZP) and its ability to prevent crack propagation [29]. (Poisson’s ratio: 0.33for zirconia vs. 0.43 for Lava Ultimate, Modulus of elasticity: 220 Gpa for zirconia vs. 12Gpa for Lava Ultimate) might give rise to stress build- up, eventually leading to material fracture. Also, this high fracture resistance of Zirconia could be related to its phase transformation toughening phenomenon. Under stresses, when crack propagates within the zirconia mass, the tetragonal grains are transformed to monoclinic with a volume expansion of (3-5%). This expansion of the grains will ultimately lead to compressive stresses at the edge of the induced crack front and so extra energy is required for the crack to propagate [30]. Results of the current study are in agreement with the results of PraffullaM, et al. [31] that showed that Full Zirconia MOD onlays of endodontically treated premolars showed higher statistically significant difference than composite CAD onlays. Our results showed higher statistically significant difference of indirect composite overlay than positive control group direct composite overlay are in disagreement with the results of Sarabi N, et al. [32] in which the use of direct composite onlay in endodontically treated teeth resulted in higher fracture resistance compared to indirect resin composite or ceramic onlay. Resin nano-ceramic (RNC), which is supposed to be shock absorbent, resilient, and not brittle. Katana zirconia overlays did not show any catastrophic fracture or un- restorable fracture. There were no statistically significant differences (p= 1) between Lava ultimate overlays and both FPR composite and positive control groups. There was not much difference in the fracture modes of Lava ultimate and positive control group (composite) the occlusal cavity depth of 5mm in the present study could have altered the stress distribution. This can be supported by Goel, et al. [33] where they suggested that deeper the prepared cavity, the greater the changes in the stress gradient in the dentin. The changes in the stress gradient could initiate fracture of the remaining cusps. The intraoral repair of resin-composite crowns can be accomplished by preconditioning, sandblasting, or bur roughening, followed by the placement of a resin composite with very similar mechanical and optical properties.
Conclusion
Within the limitations of this study, the following conclusions can be drawn:
- CAD/CAM overlays (zirconia and lava ultimate) showed significantly higher marginal discrepancy than FPR composite and direct composite resin.
- 2-Zirconium overlays showed an excellent fracture resistance with no cracks in the restoration at very high loads, compared to Resin Nano-Ceramic and FPR composite.
- 3-CAD/CAM overlays are conservative treatment option that could be used to restore damaged endodontic treated teeth. References
1. Ferrari M, Vichi A, Mannocci F, Mason PN (2000)
Retrospective study of the clinical performance of fiber posts. Am J Dent (13): 9-13.
2. Fennis WMM, Kuijs RH, Kreulen CM, Roeters FJ,
CreugersNH, et al. (2002) A survey of cusp fractures in a population of general dental practices. Int J Prosthodont 15(6): 559 -563.
3. Assif D, Gorfil C (1994) Biomechanical consideration in restoring endodontically treated teeth. J Prosthet Dent 71(6): 565 -567.
4. Bitter K, Kielbassa AM (2007) Post-endodontic
restorations with adhesively luted fiber-reinforced composite post systems: a review. Am J Dent 20(6): 353-360.
5. Magne P (2006) Composite resins and bonded porcelain: the postamalgam era? J Calif Dent Assoc 34(2): 135-147.
6. Akkayan B, Gulmez T (2002) Resistance to fracture of endodontically treated teeth restored with different post systems. J Prosthet Dent 87(4): 431-437.
7. Lanza A, Aversa R, Rengo S, Apicella D, Apicella A
(2005) 3D FEA of cemented steel, glass and carbon posts in a maxillary incisor. Dent Mater 21(8): 709- 715.
8. Guzy GE, Nicholls JI (1979) In vitro comparison of intact endodontically treated teeth with and without endo-post reinforcement. J Prosthet Dent 42(1): 39- 44.
9. Zarone F, Sorrentino R, Apicella D, Valentino B,
Ferrari M, et al. (2006) Evaluation of the biomechanical behavior of maxillary central incisors restored by means of endocrown compared to a natural tooth: a 3D static linear finite element analysis. Dent Mater 22(11): 1035-1044.
10. Castellani D, Bacetti T, Giovannoni A, Bernardini DU
(1994) Resistance to fracture of metal-ceramic and all-ceramic crowns. Int J Prosthodont 7(2): 149-154.
11. Lina CL, Changb YH, Paia CA (2011) Evaluation of failure risks in ceramic restorations for endodontically treated premolar with MOD preparation. Dent mater 27(5): 431-438.
12. Rosenblatt R (2012) A complete ceramic for chair side CAD/CAM restorations. Compend Contin Educ Dent 33(6): 7-9.
13. Holmes JR, Bayne SC, Holland GA, Sulik WD (1989)
Considerations in measurement of marginal fit. J Prosthet Dent 62(4): 405-408.
14. Hickel R, Roulet JF., Bayne s, Heintze SD, Mjor I, et al.
(2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Clinic oral invest 11(1): 5-33.
15. Beuer F, Schweiger J, Edelhoff D (2008) Digital
dentistry: an overview of recent developments for CAD/CAM generated restorations. Br Dent J 204 (9): 505-511.
16. Witkowski S (2005) (CAD-)/CAM in Dental Technology. Quintessence Dent Technol 28: 169-184.
17. Abduo J, Lyons K, Swain M (2010) Fit of zirconia fixed partial denture: a systematic review. J Oral Rehabil 37(11): 866-876.
18. Reich S, Wichmann M, Nkenke E, Proeschel P (2005)
Clinical fit of all-ceramic three-unit fixed partial dentures, generated with three different CAD/CAM systems. Eur J Oral Sci 113(2): 174 -179.
19. Pfeiffer J (1999) Dental CAD/CAM technologies: the optical impression (II). Int J Comput Dent 2(1): 65-72.
20. Hamdy A (2015) Marginal Adaptation and Fracture
Resistance of Resin Nano-Ceramic and Zirconium Dioxide All Ceramic Restorations. J Dent Oral Health 1: 1-5.
21. Krejci I, Duc O, Dietschi D, de Campos E (2003)
Marginal adaptation, retention and fracture resistance of adhesive composite restorations on devital teeth with and without posts. Oper Dent 28(2): 127-135.
22. Gonzalo E, Suarez MJ, Serrano B, Lozano JF (2009) A
comparison of the marginal vertical discrepancies of zirconium and metal ceramic posterior fixed dental prostheses before and after cementation. J Prosthet Dent 102(6): 378-384.
23. Gonzalo E, Suarez MJ, Serrano B, Lozano JF (2009)
Comparative analysis of two measurement methods for marginal fit in metal-ceramic and zirconia posterior FPDs. Int J Prosthodont 22(4): 374-377.
24. Wettstein F, Sailer I, Roos M, Hammerle CH (2008)
Clinical study of the internal gaps of zirconia and metal frameworks for fixed partial dentures. Eur J Oral Sci 116(3): 272-279.
25. Luthardt RG, Sandkuhl O, Herold V, Walter MH (2001)
Accuracy of mechanical digitizing with a CAD/CAM system for fixed restorations. Int J Prosthodont 14(2): 146-151.
26. Martinez-Rus F, Suarez MJ, Rivera B, Pradies G (2011)
Evaluation of the absolute marginal discrepancy of zirconia-based ceramic copings. J Prosthet Dent 105(2): 108-114.
27. Beuer F, Stimmelmayr M, Gueth, JF, Edelhoff D,
Naumann M (2012) In vitro performance of full- contour zirconia single crowns. Dent Mater 28(4): 449-456.
28. Nakamura K (2015) Mechanical and Microstructural
Properties of Monolithic Zirconia Crown Fracture Resistance and Impact of Low-Temperature Degradation. (Master thesis) University of Gothenburg .
29. Tinschert J, Zwez D, Marx R, Anusavice KJ (2000)
Structural reliability of Alumina, Leucite, Mica and Zirconia based ceramics. J Dent 28(7): 529-535.
30. VagkopoulouT, Koutayas SO, KoidisP, Strub JR (2009)
Zirconia in dentistry: Part 1.Discovering the nature of an upcoming bioceramic Eur j Esthet Dent 4(2): 130- 151.
31. Mynampati P, Babu MR, Saraswathi DD, Kumar J R,
Gudugunta L, et al. (2015) Comparison of fracture resistance and failure pattern of endodontically treated premolars with different esthetic onlay systems: An in vitro study. J Conserv Dent 18(2): 140 -143.
32. Sarabi N, Taji H, JalayerJ, Ghaffari N, Forghani M
(2015) Fracture Resistance and Failure Mode of Endodontically Treated Premolars Restored with Different Adhesive Restorations. JDMT 4: 13-20.
33. Goel VK, Khera SC, Gurusami S, Chen RC (1992) Effect
of cavity depth on stresses in a restored tooth. J Prosthet Dent 67(2): 174-183.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells