The Use of Botox Injection to Treat Cerebral Palsy in Children
Background: Cerebral Palsy is the most common neuromuscular disability in children. It is a group of permanent disorders related to development of movement and posture that occurs in the infant’s brain. Cerebral Palsy results in spascitiy, along with many different abnormalities such as visual impairment, hearing loss salivation and speech problems. Although, these symptoms were previously treated by surgical intervention, during the recent years Botulinum Toxin A (BTXA) has gained popularity and acceptance from FDA and proved to a more superior approach in treatment of cerebral palsy when applied through a multilevel integrated approach. Objective: To understand the mechanism of action of BXA, to find out the recommended age, dose and technique and evaluate the advantages and disadvantages of BTXA. Methodology: A literature review of more than 60 articles that were classified into 20 literature review, 20 RCT and others case control or cohort studies using a medical engine (Pubmed) were analyzed, organized and summarized. Results: Many studies have recommended earlier intervention for treatment of children with BTXA as children with younger age (2-6 years) show better response as their motion and gait patterns are still flexible. Furthermore, no technique or dose has proven to be more effective in treatment of cerebral palsy, even though literature shows the short life of BTXA (3 months) more established studies have found that repeated injections (up to 3 injections) have shown to increase the quality of life and gross motor function of these children up to 18 months after their injection. Conclusion: BTXA injections have proven to be effective in improving the gross motor function and quality of life of children with Cerebral Palsy. Also, BTXA injections have shown to be effective in treating dental symptoms of children with CP such as sialorrhea. The recommended approach for BTXA injections is a multilevel approach this can be done by combining the injections with conservative therapies such as physiotherapy, orthodontic management or casts. All adverse events associated with BTXA have been rated mild to moderate; no severe effects were reported.
Introduction
Cerebral palsy is a group of permanent disorders of development of movement and posture that occur in infant’s brain. It is the most common motor disability in children; it is a neuromuscular condition that affects speech, posture and gait. The cause of cerebral palsy is either due to damage in a portion of brain or spinal cord [1]. Cerebral palsy results in spasticity, a condition that causes muscles to contract continuously.
However, children with cerebral have varying degrees of physical disabilities and often this physical disability has other health implications than brain damage as their condition is associated with visual impairment, hearing loss, food aspiration, excessive salivation, speech problems, tooth decay and sleep disorders [2]. Although there is no permanent cure for the treatment of cerebral palsy, it is now common to use Botulinum Toxin A (BTXA) for the treatment of the majority of these symptoms.
The use of BTXA in treatment of cerebral palsy first got approval by FDA in 1989. One of the first to experiment the therapeutic use of BTXA to treat children with cerebral palsy was Koman in 1993. This study aims to provide a detailed study to evaluate the effectiveness of botox injections in treatment of cerebral palsy, the mechanism BTXA in treatment of children with cerebral palsy and the advantages and disadvantages and role in treatment of sialorrhea in children.
Review of Literature
Cerebral palsy can be categorized into different types according to defect in anatomical part of the brain. There is a spastic type which is due to a defect in cerebral cortex, dyskinetic type associated to damage in basal ganglia, ataxic type which is due to damage to cerebellum and can be mixed.
Although no permanent cure is available for cerebral palsy, botox injections have shown to be effective to provide relief for children with cerebral palsy on many levels. BTXA has been preferred in treatment of children with cerebral palsy over alternative treatment options such as surgery, due to the fact that surgery is a risk factor for relapse and failure [3]. A multilevel BTXA approach has been recommended by researchers for more than 15 years to limit the side effects of botox, this can be done by using conservative therapies such as physiotherapy, orthodontic management or casts [3]. This will help reduce the risk of persistent increased muscle tone of botox and will help the child to maintain his functional ability for a longer time after the temporary effect of botox diminishes as they have shown better results than using botox solely.
The mechanism of action of BTXA is that it targets the neuromuscular junction, preventing the release of acetylcholine from the nerve terminals, which allows the child to have better motor control. This can increase the child’s self-esteem and functional ability. According to many literature reviews, the ideal age for botox injections is from 2-6 years where child’s motor, speech and gait patterns are still flexible [4]. The temporary effect of botox varies based on many factors such as the individual, the amount injected and the purpose of the injection. The relaxing effect of Botox injection lasts approximately for 3 months [5].
While considering the advantages of Botox in increasing a child’s self-esteem and motor function and allowing him to participate in a wider range of motion activities [6]. It is also important to undermine the side effects of that can be classified into minor effects such as pain and mild flu like symptoms, there are also major side effects such as muscle contractures and bony deformities.
A common dental symptom Sialorrhea which is drooling or excessive saliva has been correlated to cerebral palsy. This is due to the fact that the defect caused by neuromuscular condition results in impaired swallowing; about 10% to 37.5% of patients with cerebral palsy have sialorrhea. There are different treatment approaches such as anticholinergic drugs, which have shown many side effects such as constipation, irritability and blurred visions or surgical procedures. However, in children invasive treatments are often unacceptable to the patients and their families. Also according to a study done on 50 children of cerebral palsy through the surgical, oral contraceptives and BTXA to treat sialorrhea in children with neuromuscular conditions, BTXA showed better results in control of saliva and for a longer period of time. Therefore, BTX A has proven to be a better option in treating sialorrhea. The severity and frequency of sialorrhea in these patients is then evaluated every 2-4 weeks until 20 weeks after injection.
Materials and Methods
This research is a literature review about the use of BTXA to treat children with cerebral palsy. A medical engine “PUBMED” was used to search recent articles within the past 10 years. Using the following keywords “Botulinum Toxin A”, “Cerebral palsy”, “children”, “Sialorrhea”. More than 60 articles that were classified into 20 literature review, 20 RCT and others case control or cohort studies. These articles followed the inclusion criteria any studies that include information about the usage of BTXA in treatment of children with cerebral palsy, studies that include advantages and disadvantages of BTXA, studies that include information about treatment of sialorrhea using BTXA and studies that were done in the past few years. On the contrary, studies that include any information about the usage of botox in adult group, the use of botox in treatment of neuromuscular conditions other than cerebral palsy and studies that include any information regarding alternative spasticity treatments were excluded.
Results and Discussion
There is specific criteria that BTXA follow in order to be a successful treatment, these characteristics are: long term applicability, sustainability and individual and flexible planning. This can be achieved through applying BTXA as an integrated treatment approach, with the prospective of standing and weight bearing and providing the children with cerebral palsy with the best locomotion [7].
Many studies have suggested that the treatment of cerebral palsy is an age related procedure, where children with younger age (2-6 years) show better response to treatment to older children as their gait, walking and motion patterns are still flexible and the side effects of developing bony or muscle contractures with botox increase with age [8]. However, studies have also shown that timing of intervention is also dictated by the severity of the neurological condition, children who are more severely affected require earlier intervention. Also, children who are older than 6 years old can still benefit from the use of BTXA as it can be used to target specific muscles in order to maximize their function and reduce their pain.
Another rationale that one article had suggested for starting treatment at an earlier age is purely based on neurological studies that revolve around neuroplasticity because the younger brain has a higher potential for motor learning. This is suggested because children can learn new and more rapid movements that will improve their coordination [9].
Furthermore, there is no specific recommended dose for BTXA in treatment of cerebral palsy. Over the recent years, specifically from 2010 onwards it was suggested to increase the dose of BTXA (in kg/ body weight) in treatment of cerebral palsy to increase the effectiveness of Botox. As shown in the Figure 1.
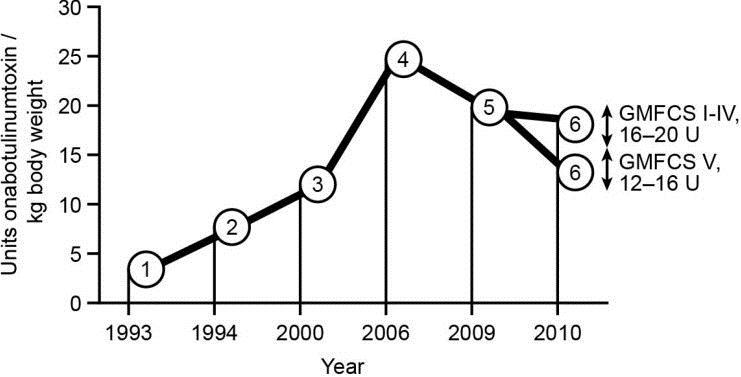
However, based on more recent studies (in the past 5 years specifically) that the dose is not always an indicator for improving the condition of gait and motor flexibility of a child. Controlled studies have experimented with a wide range of doses from (10 U/kg to 25 U/Kg) and both lower doses and higher doses from (10 U/kg to 25 U/kg), all doses proved to be safe and have a significant effect on reducing spasticity and improving gait, speech [10]. The only significant finding established from studies is that multilevel BTXA injections (repeated botox injections) proved to be more beneficial and therapeutic for treatment of children with cerebral palsy than single injections. Also, using repeated botox injections does not increase the risk of any side effects according to a study to one study with 20 sample size of children with cerebral palsy receiving multiple BTXA injection and 18 sample size receiving single BTXA injection, there was no difference in risks for cerebral palsy children for those who received one or two cycles of BTXA.
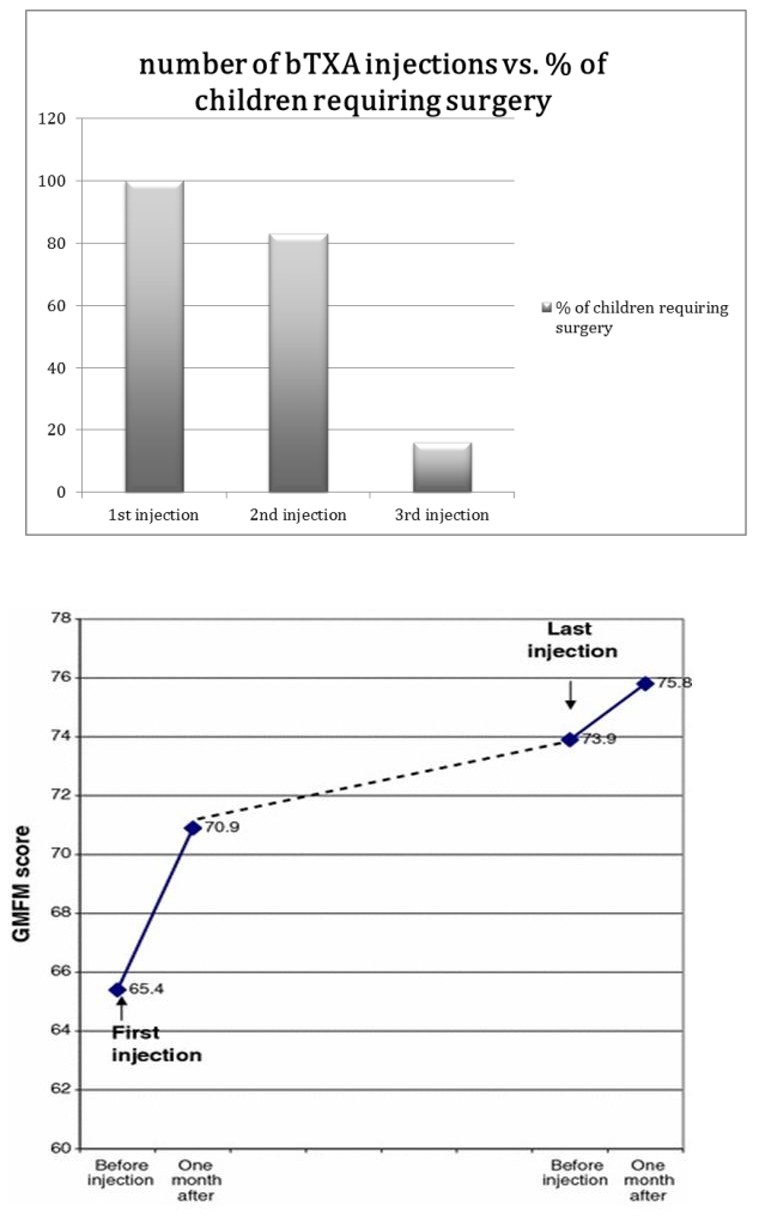
According to one study done on 23 children categorized into: 5 children who received one injection, 12 received 2 injections, and 6, which received 3 injections. After results were collected, 5 children who stopped treatment after first injection had to undergo orthopedic surgery within one year, which shows 100% percentage of failure and 12 children who discontinued treatment after two injections underwent an orthopedic surgery within one year, which shows 83% of failure of treatment. However, the 6 who received 3 injections only one had to undergo orthopedic surgery within a year, which is only a 16% percentage of failure. However, it is important to note that for children who still need orthopedic for treating musculoskeletal deformities and contractures associated with cerebral palsy they still benefit from BTXA treatment, as the goal is to avoid multiple operations as this can weaken muscles excessively.
The studies have suggested that the ideal number of injections for Botox is up to 3 injections with a time interval of 3-6 months between each injection [11]. However, due to the side effects of Botox, more than 3 injections have been associated with bony fractures, muscle contractures, and flu like symptoms, irritation and redness.
In theory, BTXA is more efficient if injected near the motor endplate areas, these are located in midpoint in striated muscles. BTXA’s injection can be guided by many different technique approaches, which include palpation, ultrasound and EMG. By using palpation, target muscles can be identified. According to studies EMG is only beneficial in dystonia; however spastic cerebral palsy muscles do not allow differentiation. Also, studies have recommended the use of palpation as it less invasive for children and other methods do not prove to be superior. After, guiding the site of injection the mechanism of action of BTXA is that it targets the nerve terminals and prevents the release of acetylcholine which prevents the continuous contraction of muscles and allows the muscles to be paralyzed [12], this allows the child to improve his motor control and help increases his self-esteem.
The results obtained from the studies shows the long- term effect of BTXA in treatment of children with cerebral palsy. Even though BTXA effect is known to be temporary and muscle tone is known to return to its original state a few months after the effect of Botox injection diminishes, the studies collected show that Botox injections can be long lasting if child benefits up to three injections. Even though muscle tone significantly reduced after 3 months of Botox injection [13], there was a significant change in the children’s motor function. This was established through measuring the Gross Motor Function Measure , is a 5 level clinical classification system that describes gross motor function of people with cerebral palsy on the basis of self-initiated movement abilities. This is demonstrated in Table1.
| Gross Motor Function Classification System (GMFCS) Expanded and Revised | |
|---|---|
| Level | Description |
| Level I | Walks without limitations |
| Level II | Walks with limitations |
| Level III | Walks using a hand-held mobility device |
| Level IV | Self-mobility with limitations |
| Level V | Transported in a manual wheelchair |
Table 1: GMFCS classification.
*GMFCS- E & R © Robert Palisano, Peter Rosenbaum, Doreen Bartlett, Michael Livingston, 2007 CanChild Centre for Childhood Disability Research, McMaster University. Table 1: GMFCS classification.
More than 30 studies use GMFCS scores pre and post BTXA treatment to show the significant change those children with cerebral palsy may experience in terms of their motor function after receiving injections [8], as children have a higher GMFM score after Botox injection before receiving Botox treatment. The effect on motor function had shown to be persistent for 19 months after receiving BTXA. This is demonstrated below Figure 2.
Furthermore, studies established from more than 20 articles have shown that BTX-A injections show long lasting effects when used as a combined therapy. Combined P receive BTXA injections followed by alternative conservative support therapies which are non- surgical such as physiotherapy, exercises for muscles or orthotic management such as casts, it is believed that this strengthens their extensor muscles. This should occur after the first few weeks of receiving BTX-A injection, as the toxin is still pharmacologically active, it can also be done before the course of Botox.
According to one case control study, a study group of 6 years old children with CP received 6 months of pre injection physiotherapy and continued to be treated with conservative therapies for 11 groups. The study concluded that all children who underwent conservative therapies showed better results than children who solely depended on the BTXA injections from other studies. However, the limitation of the study is that only children from 6 years were evaluated, better results could be established from younger patients as the risk of fractures and bony deformities increase with age [14].
In addition, another study was conducted that explicitly focuses on quality of life among children with cerebral palsy treated with BTXA. This study included fifty seven patients who used BTXA whose quality of life was assessed through questionnaires handed to their parents before the first use of BTXA and after a year of follow up. The study used statistical analysis as a non- parametric Wilcoxon test was used to compare the 2 different time points. The sample study was retrieved from 57 patients (34 Males) with a mean age of 6 years and 2 months. The number of BTXA injections varied from 1 to 4. 20 of the sample only underwent one session of BTXA, 30 underwent 2 to 4 sessions [15].
According to the study findings, the researchers established that younger age demonstrates a greater reduction in spasticity than older patients, the number of BTXA injections is positively correlated with reduction in spasticity this means that a multilevel BTXA injections means an increase in the quality of life of the children, also children with educated caregivers showed a greater gain in quality of life.
Moreover, 44% of these children showed a significant improvement in the level of GMFC score as ten patients at level II reached level I, 9 patients at level IV reached level III and 1 patient in level III reached level I. However, the limitation of the study is that a larger group should be assessed for their GMFC scores to confirm these findings.
BTX-A has also proven to be effective in treating a dental implication of children with CP (Sialorrhea). Sialorrhea, which is a dental condition in which a child has excessive salivation/ drooling has been reported to be one of the main symptoms of CP children who have mental or abnormalities in their facial morphology as 40% suffer from sialorrhea. This is due to the fact that they have a lack of control or coordination over their swallowing patterns that cause them to have excessive pooling of saliva in the oral cavity. Persistent drooling of saliva causes major psychosocial and hygienic problems. In the past, Sialorrhea was treated by pharmacological means with anticholinergic drugs however this has shown to be ineffective and has been associated with many side effects such as constipation, irritability, urinary retention and blurred vision [16]. Other methods have been surgical procedures of resecting the salivary gland, however most parents find this treatment unacceptable as it very invasive.
The modern approach of treating Sialorrhea is with BTX- A injections, this is guided by ultrasound machine to detect glands, a tiny needle is inserted through the skin into glands and a tiny amount of botox is injected into space. According to a case control study, degree of sialorrhea was evaluated before injection, 1, 2, 4, 6 and 9 months later, the sample study included 17 children with cerebral palsy, There were significant improvements of reduction in their saliva as 12 of 17 cases (70.5%) showed more than 50% reduction of salivary flow than they did prior to Botox injections. as shown below in Figure 3.
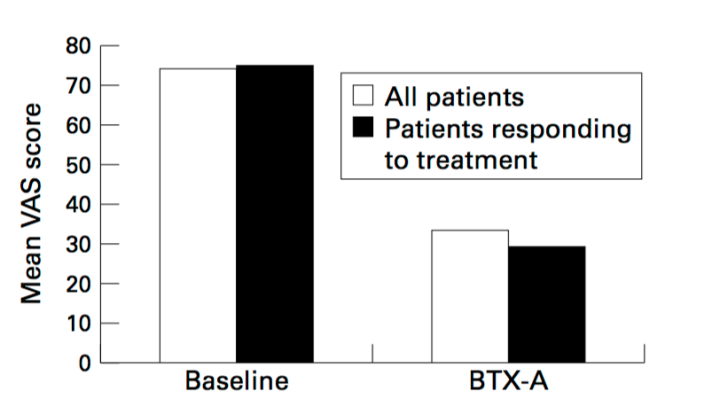
The limitations to the study mainly were that three patients had spastic cerebral palsy and had received anticonvulsant medications, which had an effect on their drooling; therefore they did not show any improvement with BTXA in saliva control. Furthermore, other studies have suggested that it is recommended to inject does of 10-50 u A/one into each submandibular gland or each parotid gland alone or into all four salivary glands, but there is no definitive conclusion regarding to the dose. There were moderate side effects reported in terms of eating or swallowing only during first week after injection.
Although, BTX-A has shown to have many advantages superior to other treatments that makes it ideal for most children with CP as it is both a conservative and cost effective approach and can help increase a child’s self- esteem and motor abilities, Botox remains to be a controversial topic for treatment of Cerebral Palsy is the adverse effects of Botox [17].
According to most studies, local adverse effects at the injection site included bruising, pain, edema and erythema. However, systemic adverse reactions were categorized into flu-like symptoms, fatigue, generalized weakness, malaise and nausea [13]. Sometimes it may be difficult to separate systemic adverse events from local diffusion into the autonomic nervous system nerve endings (urinary or fecal incontinence, dry mouth). The severity and frequency of adverse events depend on the injection site and technique and the indication. As demonstrated in Table 2.
| Local | Adverse | ||||
|---|---|---|---|---|---|
| Bruising | Fatigue | ||||
| Pain | Generalized weakness | ||||
| Edema | Malaise | ||||
| Erythema | Nausea |
Table 2: Local and adverse effects of BTXA.
The safety of Botox was assessed in a meta-analysis comprising 36 randomized clinical trials. The incidence of adverse events was 25% for Botox and 15% for controls (placebo or other control group for comparison). Focal weakness was the specific adverse event occurring significantly more frequently in Botox treatments; this is a cause of mechanism of action. All adverse events were rated mild to moderate; no severe or systemic adverse events were reported.
Conclusion
In conclusion, although no permanent cure has been found for cerebral palsy. BTXA injections have proven to be effective for providing relief and improving the gross motor function of these children. It would be more ideal to start an earlier intervention as children from ages (2- 6 years) still have flexible gait and motion patterns and respond better to BTXA treatment than those who are older. Also, BTXA injections have shown to be effective in treating dental symptoms of children with CP such as sialorrhea. The recommended approach for BTXA injections is a multilevel approach this can be done by combining the injections with conservative therapies such as physiotherapy, orthodontic management or casts. Furthermore, there is no dose or technique that proves to be superior to others however repeated injections of BTXA up to 3 injections has shown to have a more long lasting effect than a single injections.
Limitations
Our study has some limitations as the follow up on majority of children with cerebral palsy was ≤2 years, therefore it would be beneficial to have studies with a longer follow up period to ensure the longevity of BTXA treatment.
Future Direction
It would be beneficial to expand these studies to include a vast area of dental symptoms for example knowing which gland is most effective to inject for treatment of sialorrhea, also other dental anomalies that could be correlated to cerebral palsy. Another suggestion would be to have longer post botox treatment results for instance after 10 years to see the long term results.
References
-
Cerebral Palsy Foundation (2017) The use of botulinum toxin to treat children with cerebral palsy. pp: 3-8.
-
Bjornson K, Hays R, Graubert C, Price R, Won F, et al. (2007) Botulinum toxin for spasticity in children with cerebral palsy: a comprehensive evaluation. Pediatrics 120(1): 49-58.
-
Criswell S, Crowner B, Racette BA (2006) The use of botulinum toxin therapy for lower-extremity spasticity in children with cerebral palsy. Neurosurg Focus 21(2): 1.
-
Batman Friedman (2018) The ideal age for the treatment of children with cerebral palsy. Physical therapy.
-
Karen W Nolan, Lynn L Cole, Gregory S Liptak (2006) Use of Botulinum Toxin Type A in Children With Cerebral Palsy. Physical Therapy 86(4): 573-584.
-
Kumar R, Wadhwa S, Singh U, Yadav S (2015) Clinical outcome with Botulinum toxin-A in spastic cerebral palsy children with equinus gait. Astrocyte 2(1): 4-7.
-
Slawek J, Klimont L (2003) Functional improvement in cerebral palsy patients treated with botulinum toxin A injections-preliminary results. Eur J Neurol 10(3): 313-317.
-
Desloovere K, Molenaers G, De Cat J, Pauwels P, Van Campenhout A, et al. (2006) Motor function following multilevel botulinum toxin type A treatment in children with cerebral palsy. Dev Med Child Neurol 49(1): 56-61.
-
Pavone V, Testa G, Restivo D, Cannavò L, Condorelli G, et al. (2016) Botulinum Toxin Treatment for Limb Spasticity in Childhood Cerebral Palsy. Front Pharmacol 7: 29.
-
Molenaers G, Desloovere K, De Cat J, Pauwels P, et al. (2001) Single event multilevel botulinum toxin type A treatment and surgery: similarities and differences. Eur J Neurol 5: 88-97.
-
Mathews J, Balaban B (2009). Management of spasticity in children with cerebral palsy. Eur PMC 43(2): 81-86.
-
Boyd RN, Hays RM (2001) Current evidence for the use of botulinum toxin type A in the management of children with cerebral palsy: a systematic review. Eur J Neurol 5: 1-20.
-
Akkaya R (2005) Efficacy of botulinum toxin type A in the management of children with cerebral palsy.
-
Stockman J (2009) Botulinum Toxin for Spasticity in Children with Cerebral Palsy: a comprehensive evaluation. Pediatrics 120(1): 49-58.
-
Dimitrijevic L, Stankovic I, Zivkovic V, Mikov A, Colovic H, et al. (2007) Botulinum toxin type A for the treatment of spasticity in children with cerebral palsy. Vojnosanit Pregl 64(8): 513-518.
-
Vaile L, Finlay F (2006) Is injection of botulinum toxin type A effective in the treatment of drooling in children with cerebral palsy?. Arch Dis Child 91(10): 862-863.
-
Fattal-Valevski A, Domenievitz D, Giladi N, Wientroub S, Hayek S (2008) Long-term effect of repeated injections of botulinum toxin in children with cerebral palsy: a prospective study. J Child Orthop 2(1): 29-35.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells